
Remember me



To investigate the health and nutritional status of mothers and infants, a cross-sectional survey was conducted in two prefecture-level cities located within the Qinba Mountains area, situated in the southern region of Shaanxi province. The Qinba Mountains area spans six provinces of western China located in Qinling and Bashan Mountains, which was one of the eight multidimensional Poverty in Regions of Contiguous Distress in 2019 [21]. In 2019, the annual per capita disposable income in the Qinba Mountains area was USD1,659.00, similar to that of rural residents in poverty-stricken counties (USD1,677.00). Our study selected all 13 of the national-level poverty-stricken counties in two prefectures in this area [22].
SampleThe study inclusion criteria were as follows: (a) the infant resided in the sample village from birth onwards; (b) the age of the infants ranged from zero to six months (0 to 180 days). The exclusion criteria included: (a) absence or incapability of the infant’s mother to provide care for them; (b) cognitive impairment exhibited by the mother, determined by an inability to comprehend our structured questionnaire after three repetitions and verified with involvement from their families; (c) divorce or death of at least one parent. Interviews were conducted with both the mother and primary family caregiver of each infant (further details on definition provided below).
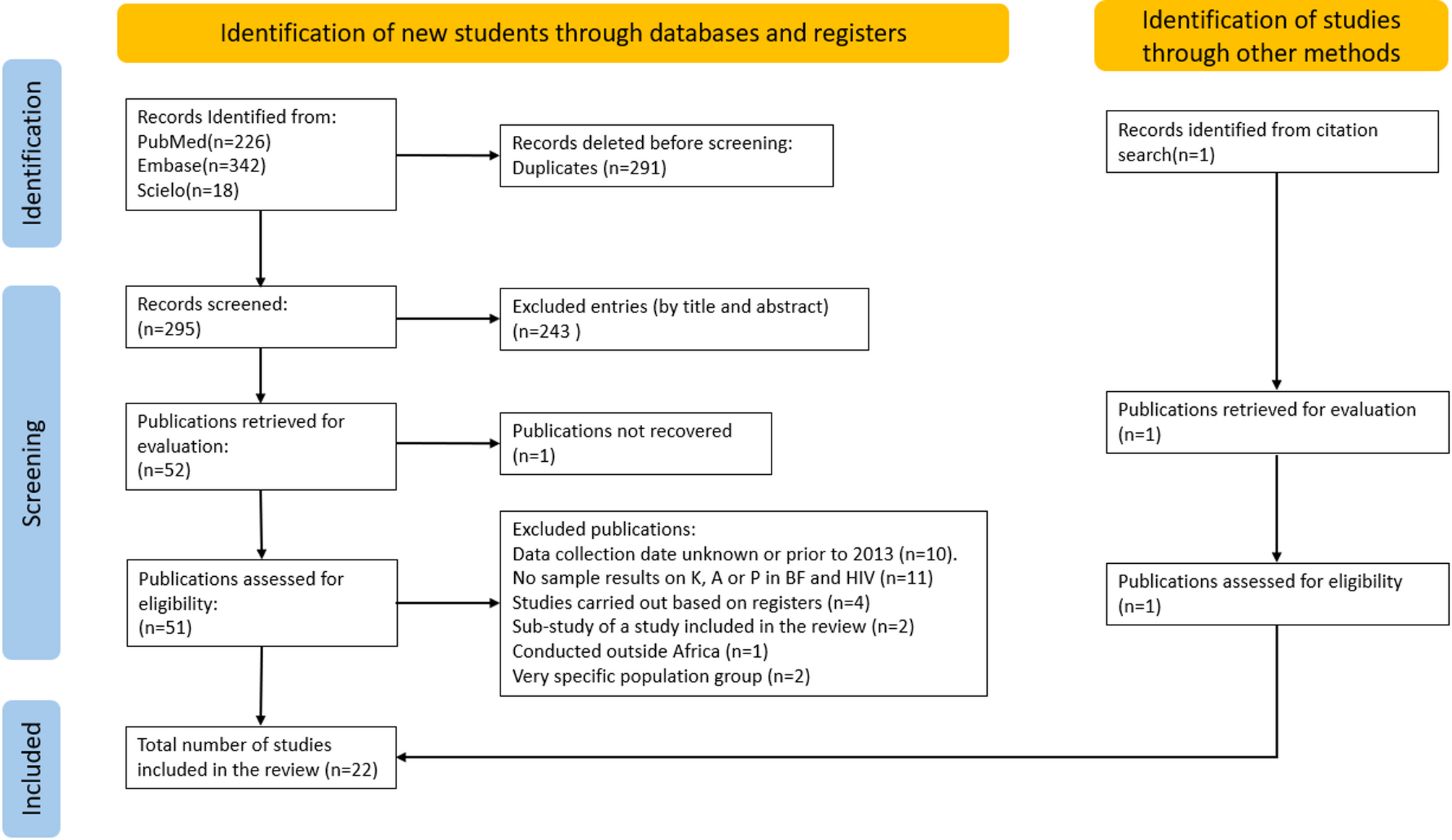
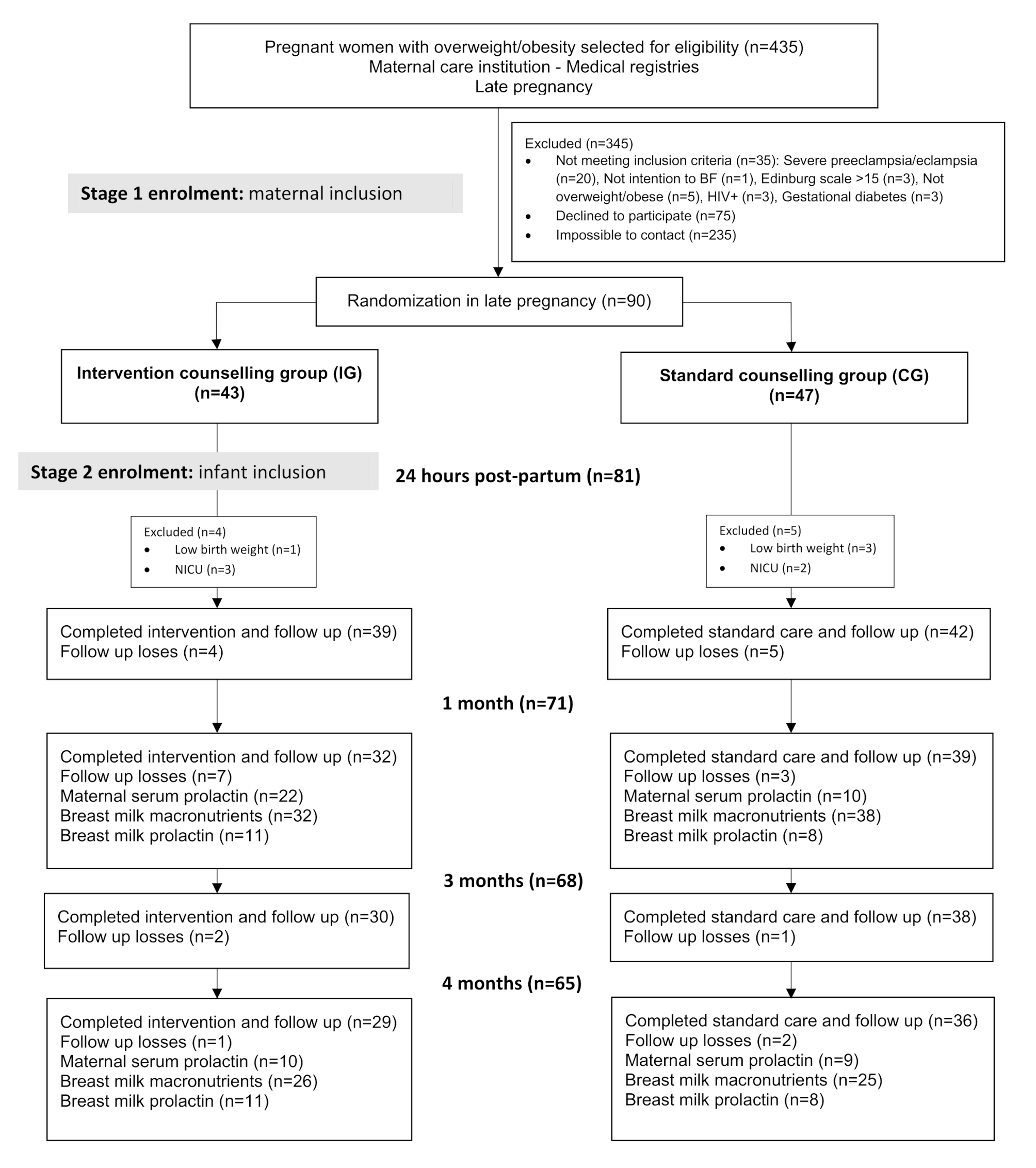
The research team employed a three-stage cluster random sampling technique to select participants for the study. Firstly, 13 nationally designated poverty-stricken counties in two prefectures within the Qinba Mountains area were chosen. Secondly, a list of villages was obtained for each county, and we randomly selected half of the total 876 rural villages from each of the 13 counties with assistance from local health commissions to form our initial village sample frame. We acquired an infant roster from the local health commissions and cross-validated it with primary healthcare providers responsible for infant management in each village. Considering the financial constraints and overall feasibility of the study, villages with a small sample size (< 3) or large sample size (> 15) were excluded, leaving 202 villages eligible for inclusion in the final sample frame. Based on our power calculation, the sample size was estimated to achieve a sampling standard error of 0.025 with a 95% confidence interval ranging from 0.10 to 0.20 for a binomial variable of 0.15, as determined from our pilot study. The final planned sample size was set at 430. Taking into account the findings from our pre-study, it was anticipated that each village would consist of approximately 3.5 households, with a 10% sample attrition rate. This led to a requirement for a minimum of 130 villages, and ultimately, 131 villages were randomly selected as the sample villages. Finally, in each of the 131 eligible villages, all caregiver-infant pairs that met the aforementioned criteria were included, resulting in a total of 495 eligible caregiver-infant pairs representing the Qinba Mountains area. However, for the purpose of analysis, 123 caregiver-infant pairs were excluded from the sample. Specifically, 115 family primary caregivers were absent during data collection and an additional 8 primary caregivers discontinued their participation after attempting to answer several questions. Consequently, a final sample size of 372 caregiver-infant pairs was considered for analysis (Fig. 1).
Fig. 1
Sampling procedure and study participants
Data collectionData were collected via face-to-face interviews conducted by trained survey enumerators between March and April 2019. Enumerators received comprehensive training on the administration of survey instruments for each main component of the study, followed by a pilot study involving twenty participants to ensure research reliability and validity. Prior to the interview, eligible participants were provided with a consent form containing detailed information regarding program objectives, procedures, potential risks and benefits, as well as a privacy statement. The mother was interviewed first, following which a brief questionnaire was administered to the primary family caregiver separately in order to minimize interruptions from other family members. The survey encompassed data collection on infant and family characteristics, demographic profiles of both mothers and primary caregivers, breastfeeding practices, as well as maternal and primary caregiver health and nutrition knowledge.
MeasurementsExclusive breastfeedingExclusive breastfeeding is the main outcome of interest. Infant feeding practices were based on the mother’s recall of the previous day (within the 24 h before the interview), including whether the infant was fed breastmilk, water, formula, fresh animal milk, juice, etc. In accordance with the definition provided by the WHO, we considered exclusive breastfeeding as feeding an infant with only breastmilk and no other liquids or solids, except oral rehydration solution and drops or syrups containing vitamins, minerals or medications [20].
Primary family caregiversA questionnaire was used to collect information on all family members living in the participant’s home for longer than three months. The primary family caregiver was defined as the individual among the family members who provided the most care to both the mother and infant during the antenatal and postnatal periods, as identified by the mothers in each household. For example, if the grandmother consistently assisted with tasks such as meal preparation, diaper changes, accompanying the mother to prenatal check-ups, and offering substantial support throughout this period, she was designated as the primary family caregiver. Conversely, if the father was frequently absent due to demanding work commitments or present at home but did not actively participate in assisting with maternal and infant care, he would not be considered as fulfilling the role of primary family caregiver. Given the sample size and sample distribution, three categories of primary family caregivers were used in this study: the infant’s father, the infant’s paternal grandparents, and the infant’s maternal grandparents.
Health and nutrition knowledgeThe mother’s knowledge of health and nutrition is the independent variable of interest, while the primary family caregiver’s knowledge in this area serves as another independent variable. Both parties employed a shared set of questionnaire items to evaluate their understanding, which was developed based on the “Guidelines for Breastfeeding in Infants Under 6 Months of Age” published by the Chinese Nutrition Society [23]. The assessment measured knowledge related to common issues within infants under six months old, including four items regarding exclusive breastfeeding, three items regarding nutrition (primarily anemia), and one item regarding general health. Questions were designed to be gender-neutral and applicable to both genders without modification. Each correct answer received one point while incorrect or unanswered questions scored zero points. Total scores ranged from 0 to 8 with higher scores indicating greater maternal nutritional and health-related knowledge. To minimize interruptions, mothers and primary caregivers responded individually.
To further investigate the association between caregivers’ health and nutrition knowledge and exclusive breastfeeding, we computed the mean level of health and nutrition knowledge as well as the disparity in such knowledge. The average level of health and nutrition knowledge among both mothers and primary family caregivers was determined by summing their respective levels of knowledge and dividing the total by two. Meanwhile, the gap in health and nutrition knowledge between mothers and primary family caregivers was calculated as the absolute difference between the mother’s level of knowledge and that of the primary caregiver.
Breastfeeding family supportBreastfeeding family support is one of the intermediate outcomes, which was measured using a scale designed by Zhu Xiu (2013) which contained nine items [24]. The original Cronbach’s alpha value of the scale was 0.886, indicating adequate reliability for internal consistency, and our study yielded a value of 0.891, suggesting its transferability to our study population. For each item, participants were asked to rate their level of agreement on a 5-point Likert-type scale ranging from strongly disagree to strongly agree. This scale can be divided into two dimensions: practical support which include two items (such as “my family often prepares food that is good for lactation”) and emotional support which include seven items (such as “I think my family wants me to exclusively breastfeed my child”). We calculated the mean score of each dimension and the higher score indicates stronger perceived family support. An average score of four or above represents high levels of breastfeeding family support.
Breastfeeding self-efficacyMaternal breastfeeding self-efficacy also serves as an intermediate variable. The study employed the revised version of the Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF), developed by Cindy-Lee Dennis in 2003 [25]. The average inter-item correlation coefficient was 0.55. The reliability of the breastfeeding self-efficacy scale was verified using Cronbach’s coefficient alpha (α = 0.94, whereas our study yielded a value of 0.62), indicating exceptional reliability and validity. This scale consists of 14 items and uses a 5-point Likert rating system, ranging from “not confident at all” to “very confident”. Higher scores indicate a higher level of maternal confidence in breastfeeding.
Conflict frequency Conflictfrequency is another intermediate outcome. The scale used to measure conflict frequency was adapted from the work of Peterman et al. (2015) and Shroff et al. (2011) [26,27,28]. The scale demonstrated acceptable internal consistency reliability, with a Cronbach’s alpha value of 0.652 in our study, as recommended by Nunnally and Bernstein (1994) [28], for evaluating maternal decision-making power. We investigated disagreements within the family regarding eight household decisions related to childcare and household consumption. Participants were asked to indicate whether they had experienced differences of opinion, with “yes” scored as 1 and “no” scored as 0. Higher scores indicate a greater frequency of conflict.
Basic participant informationInfant and family characteristics, including the infant’s gender, age in months, number of infant siblings, and family income, were collected from the mother. Additionally, demographic information about the mother was gathered, such as maternal age, education level (senior high school and above), and health and nutrition knowledge. Primary family caregiver characteristics encompassed the age of the primary caregiver, education level (junior high school and above), relationship to the infant, and health and nutrition knowledge.
Data analysisSTATA15.0 software was used for data cleaning and statistical analysis. Descriptive statistics were reported as frequencies (%) for categorical variables and mean (± SD) for continuous variables. Univariate and multivariate logistic regression analyses were conducted to examine the association between maternal and primary family caregiver knowledge of health and nutrition, in addition to various factors such as infant and family characteristics (infant age, number of siblings, family income), as well as maternal and primary family caregiver characteristics (age, education level), primary caregiver’s relationship to the infant, and exclusive breastfeeding status. Furthermore, potential mechanisms were explored using multivariate logistic regression models with consideration of county fixed effects. Odds ratios (ORs), corresponding 95% confidence intervals (CIs), and P-values were reported. Statistical significance was defined at a threshold of p < 0.05 for all tests.
Comments (0)