
記住我
The data used in this study were obtained from the Japan Environment and Children’s Study (JECS), an ongoing cohort study that began in January 2011 to identify the effect of environmental factors on children’s health.
In the JECS, pregnant women were enrolled at among 15 Regional Centers in Japan between January 2011 and March 2014. The inclusion criteria were: 1) having residence in the Study Area at the time of recruitment, 2) expected delivery after August 1, 2011, and 3) capable of comprehending the Japanese language and completing the self-administered structured questionnaire in Japanese. This study was registered in the UMIN Clinical Trials Registry (no. UMIN000030786). Details of the JECS project have been described previously [12,13,14]. The JECS protocol was reviewed and approved by the Ministry of the Environment’s Institutional Review Board on Epidemiological Studies (no. 100910001) as well as by the Ethics Committees of all participating institutions. The JECS was conducted in accordance with the Helsinki Declaration and other nationally valid regulations and guidelines. Written informed consent was obtained from all participants.
Most of the questionnaires during pregnancy were distributed to women attending prenatal examinations, with some sent by post. Completed questionnaires were submitted during subsequent prenatal visits or mailed. When possible, respondents giving incomplete answers were interviewed face-to-face or by telephone for missing details. The first trimester and second/third questionnaire response rates were 98.5% and 97.2%, respectively [12]. Regarding the medical record transcriptions of mothers in early pregnancy and children at birth, the response rates were both 100% [12]. After the neonatal period, surveying has continued every 6 months via self-administered questionnaires given by mothers or caregivers. If the questionnaire is not returned, reminders are sent by telephone, postcard, or text message as necessary by each Regional Center. As of September 25, 2022, the questionnaire response rates for 6-month-olds, 1-year-olds, and 3-year-olds are 94.1%, 91.4%, and 84.2%, respectively.
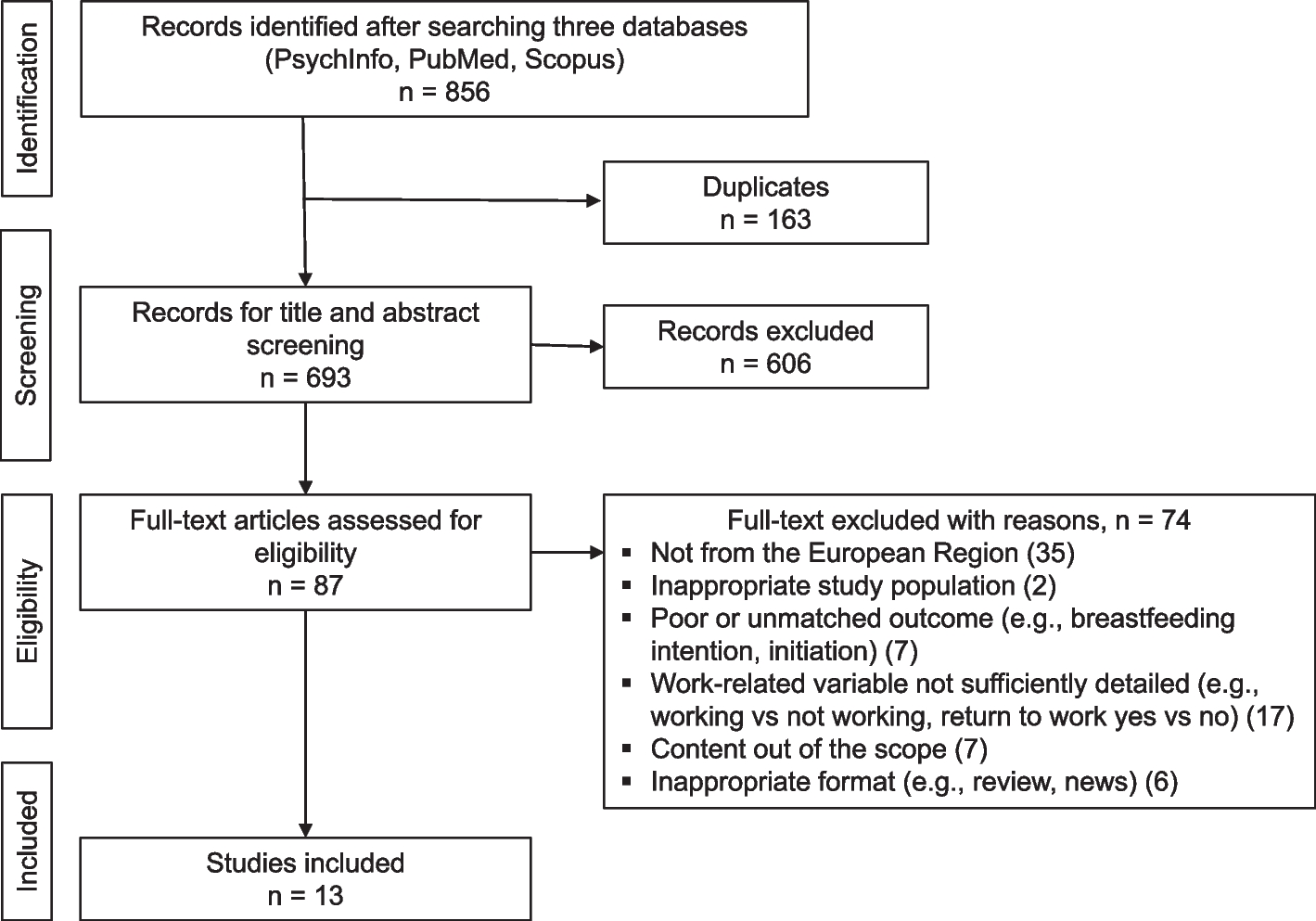
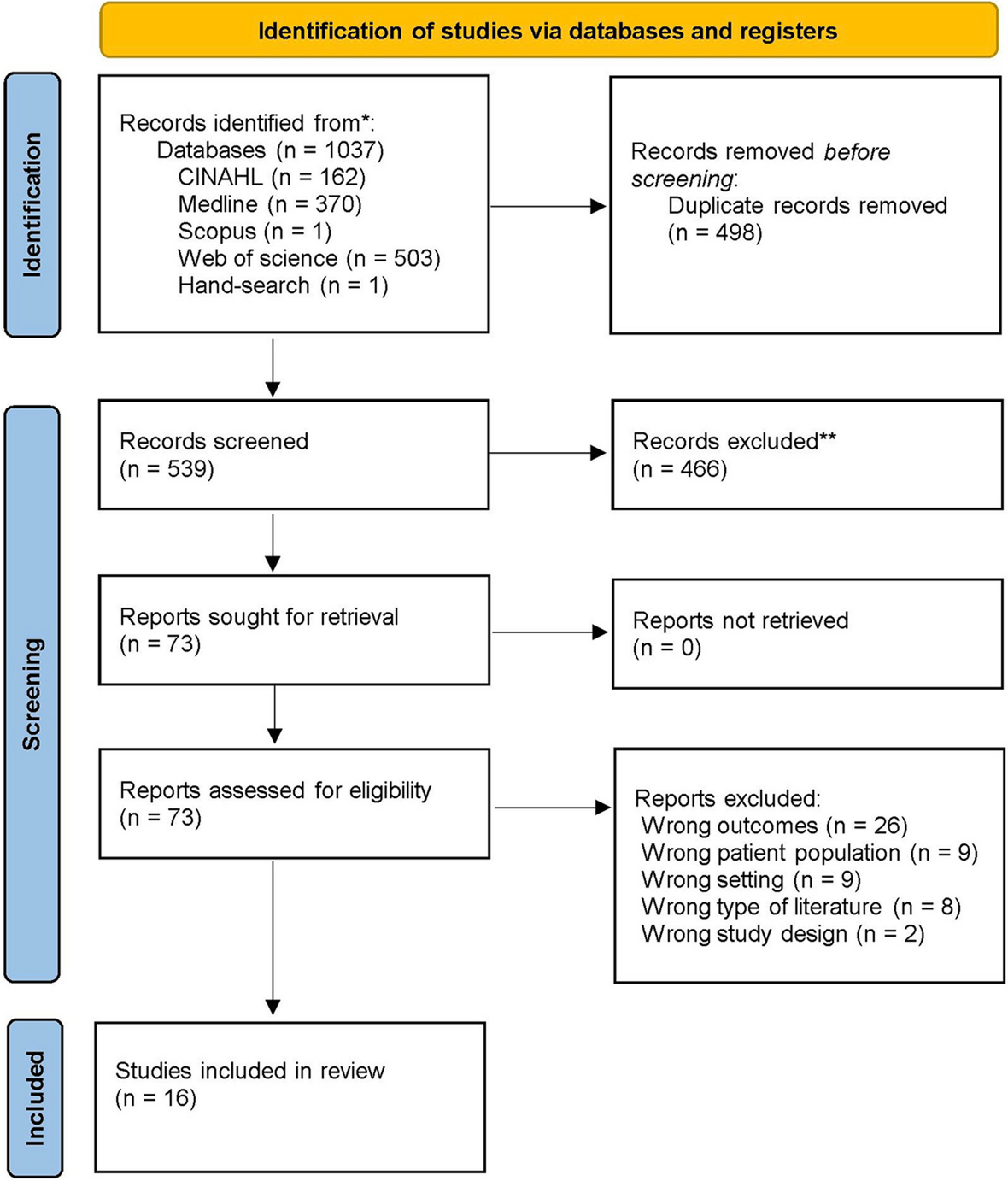
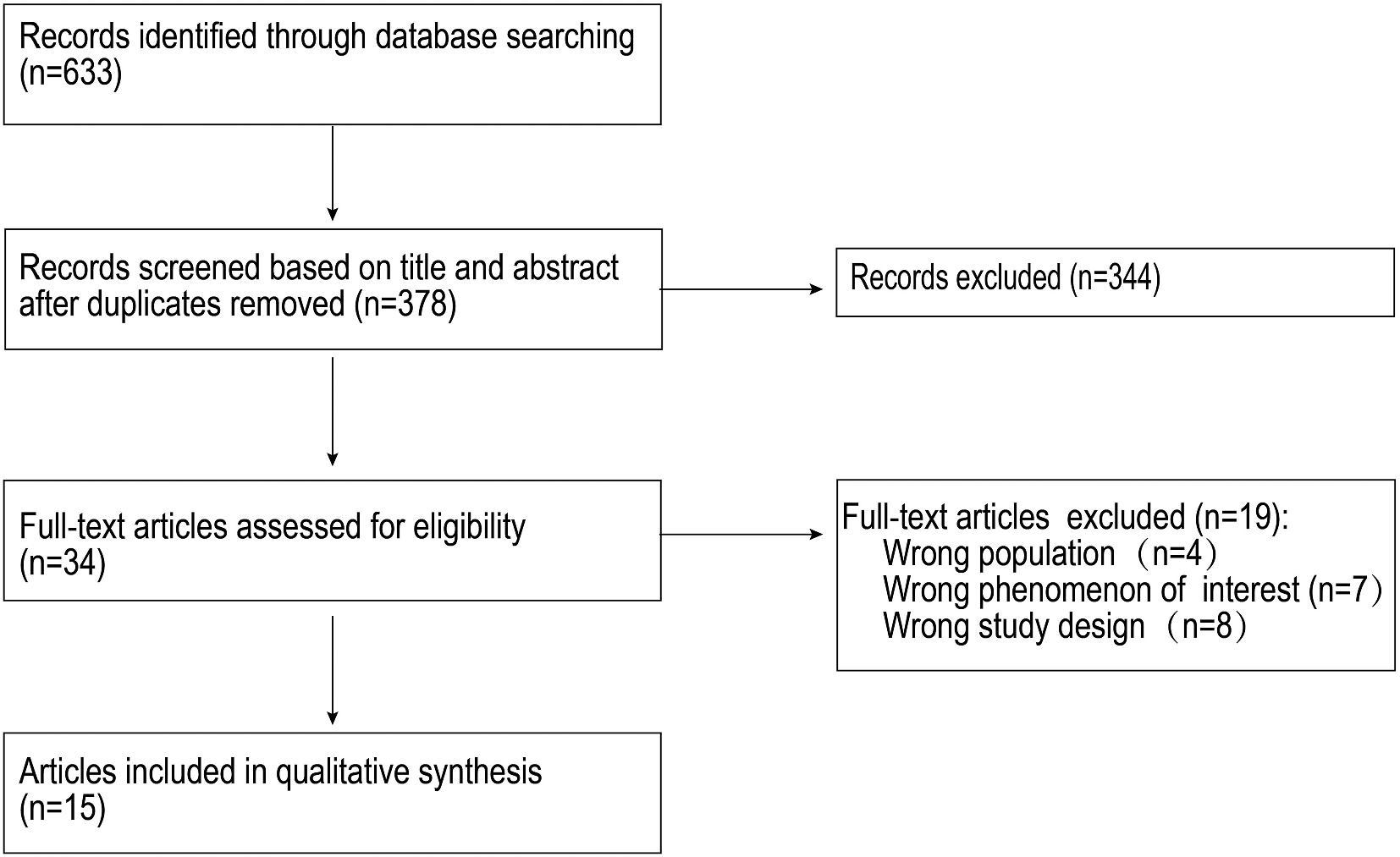
The present study was based on the “jecs-ta-20190930” dataset released in October 2019 containing information on 98,412 singleton live births. We excluded 14,246 participants with insufficient or missing data on feeding status up to 12 months of age and 13,705 with insufficient or missing data on the child’s constipation. Participants reporting known organic causes of constipation, including Hirschsprung’s disease, spina bifida, thyroid gland insufficiency, and 21 trisomy as diagnosed by physicians, were also excluded, leaving 70,078 mother-toddler pairs for the analysis (Fig. 1).
Fig. 1 Data collectionExposure
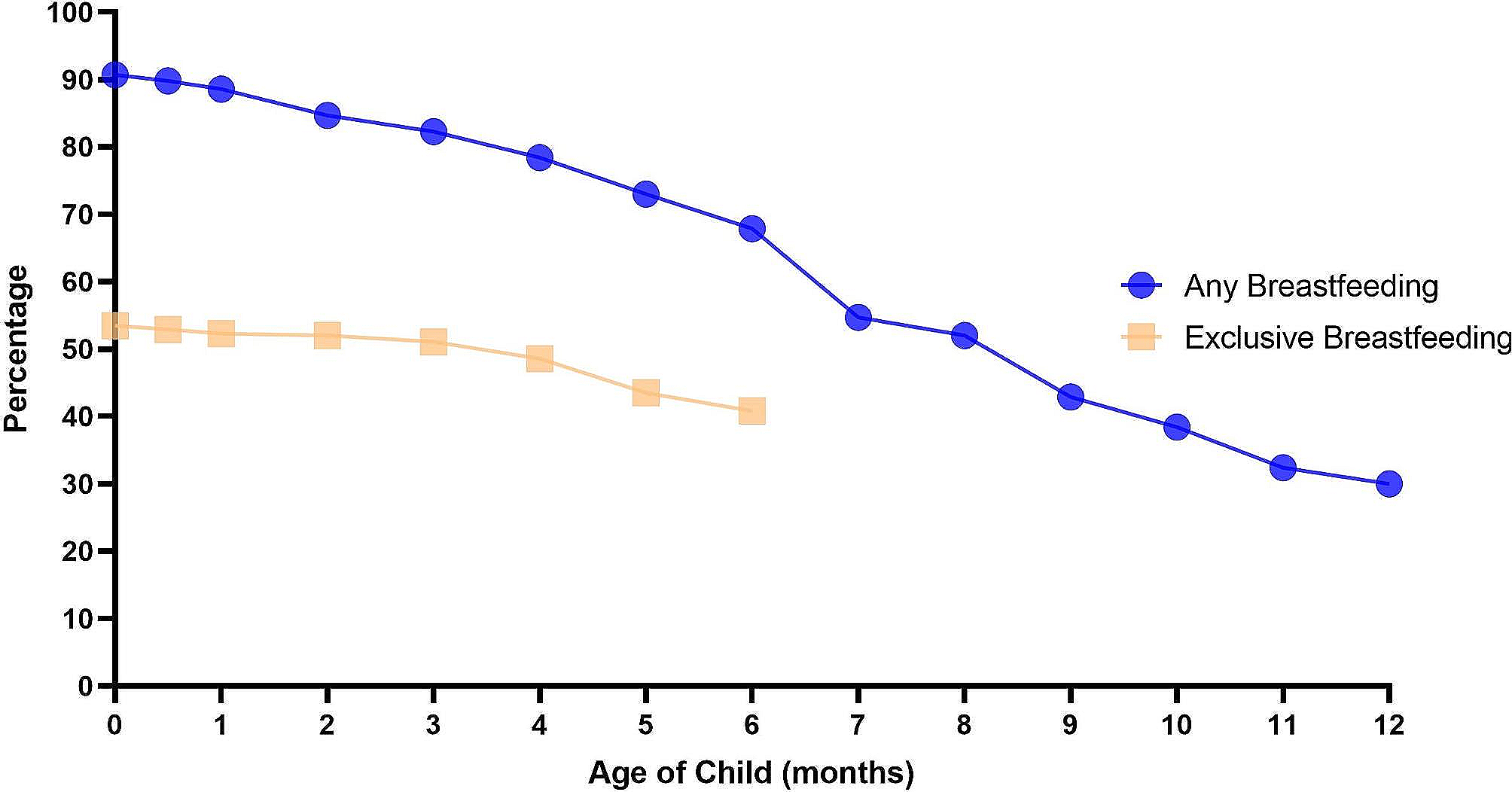
Data collectionExposureData on breastfeeding status during the first month of life were derived from medical record transcripts completed by physicians, midwives/nurses, and/or Research Co-ordinators and classified into 3 categories: breastfeeding exclusively (feeding with breast milk only), partial breastfeeding (feeding with any combination of breast milk and infant formula), or formula feeding only. Information on breastfeeding status until 6 months of age and the breastfeeding period until 12 months of age were obtained from self-reported questionnaires completed by mothers, whereby all applicable month numbers could be selected for the breastfeeding period and formula feeding period.
The breastfeeding duration up to 12 months of age was defined as the period up to the last month between 1 and 12 months in which mothers checked selections for any breastfeeding, regardless of whether or not infant formula was used in combination. Mothers who checked the breastfeeding selection for the first 6 months while leaving the formula feeding box unchecked were considered as breastfeeding exclusively. Mothers who checked the formula feeding selection for the first 6 months while leaving breastfeeding unchecked were considered as formula feeding only, with all others classified as partial breastfeeding. Partial breastfeeding referred to feeding with a combination of breast milk and infant formula, regardless of which milk was predominant. Breastfeeding status in this study referred to feeding methods related to milk, and did not take into account whether or not solid food was also provided.
OutcomesThe main outcome of interest was the presence of functional constipation in 3-year-old toddlers of mothers whose answers met the Rome III diagnostic criteria [15, 16]. Rome III is a standard set of diagnostic criteria for childhood functional gastrointestinal disorders and requires at least 2 of the following items lasting for a minimum of 1 month for a diagnosis of functional constipation: 1) two or fewer defecations per week, 2) at least 1 episode per week of incontinence after the acquisition of toileting skills, 3) history of excessive stool retention, 4) history of painful or hard bowel movements, 5) presence of a large fecal mass in the rectum, and 6) history of large-diameter stools that may obstruct the toilet. The Japanese version of Rome III was used in this study [17].
CovariatesThe covariates in our models were selected a priori based on previously published literature and biologic plausibility [4,5,6, 18,19,20,21]. We included the following covariates for mothers and their partners: maternal age at delivery (< 35 or ≥ 35 years), pre-pregnancy body mass index (BMI) (< 18.5, 18.5–24.9, 25.0–29.9, or ≥ 30.0 kg/m2), parity (primipara or multipara), cesarean birth (yes or no), maternal highest education age (< 16, 16 to < 19, or ≥ 19 years), marital status (married, single, divorced, or widowed), and annual household income (< 2 million, 2 million to < 4 million, 4 million to < 6 million, 6 million to < 8 million, or ≥ 8 million Japanese yen). As covariates for children, we included gender (male or female), gestational age (< 37, 37–41, or ≥ 42 weeks), birth weight (< 1,500, 1,500–2,499, 2,500–3,999, or ≥ 4,000 g), and started solid baby food by 6 months of age (yes or no). Pre-pregnancy body BMI to evaluate body weight status for mothers was calculated according to World Health Organization Standards as body weight (kg)/height (m)2.
Statistical analysisDistribution normality was confirmed by the Kolmogorov–Smirnov test. Data are expressed as the mean ± standard deviation or the median (interquartile range) depending on whether they are normally distributed or not, respectively. The outcome of interest was functional constipation defined as any toddler satisfying the Rome III diagnostic criteria as described by the mother. The exposure variables were breastfeeding period until 12 months of age (never [reference], up to 6 months, or ≥ 7 months), breastfeeding status at 1 month of age (breastfeeding exclusively [reference], partial breastfeeding, or formula feeding only), and breastfeeding exclusively at 6 months of age (breastfeeding exclusively [reference], partial breastfeeding, or formula feeding only). We adopted logistic regression models to calculate crude and adjusted odds ratios (ORs) and their 95% confidence intervals (CIs). The forced entry method was used to enter covariates into multivariable analysis models. Model 1 was adjusted for demographic and prenatal covariates, including maternal age at delivery, pre-pregnancy BMI, maternal highest level of education, annual household income, marital status, maternal gestational weight gain, and parity. Model 2 was adjusted for the covariates in model 1 in addition to covariates after birth, including cesarean section at delivery, gender, birth weight, and started solid baby food by 6 months of age. The JECS protocol prohibits sharing the ORs of covariates to prevent double publications because other JECS studies use covariates as outcomes in parallel. Missing data on covariates were excluded in the logistic regression models. Spearman’s rank correlation coefficient was used to check for multicollinearity of covariates. Hosmer–Lemeshow testing was employed to assess the goodness-of-fit of the models. All statistical analyses were performed using SPSS statistical software version 29 (SPSS Inc., Chicago, Illinois).
留言 (0)