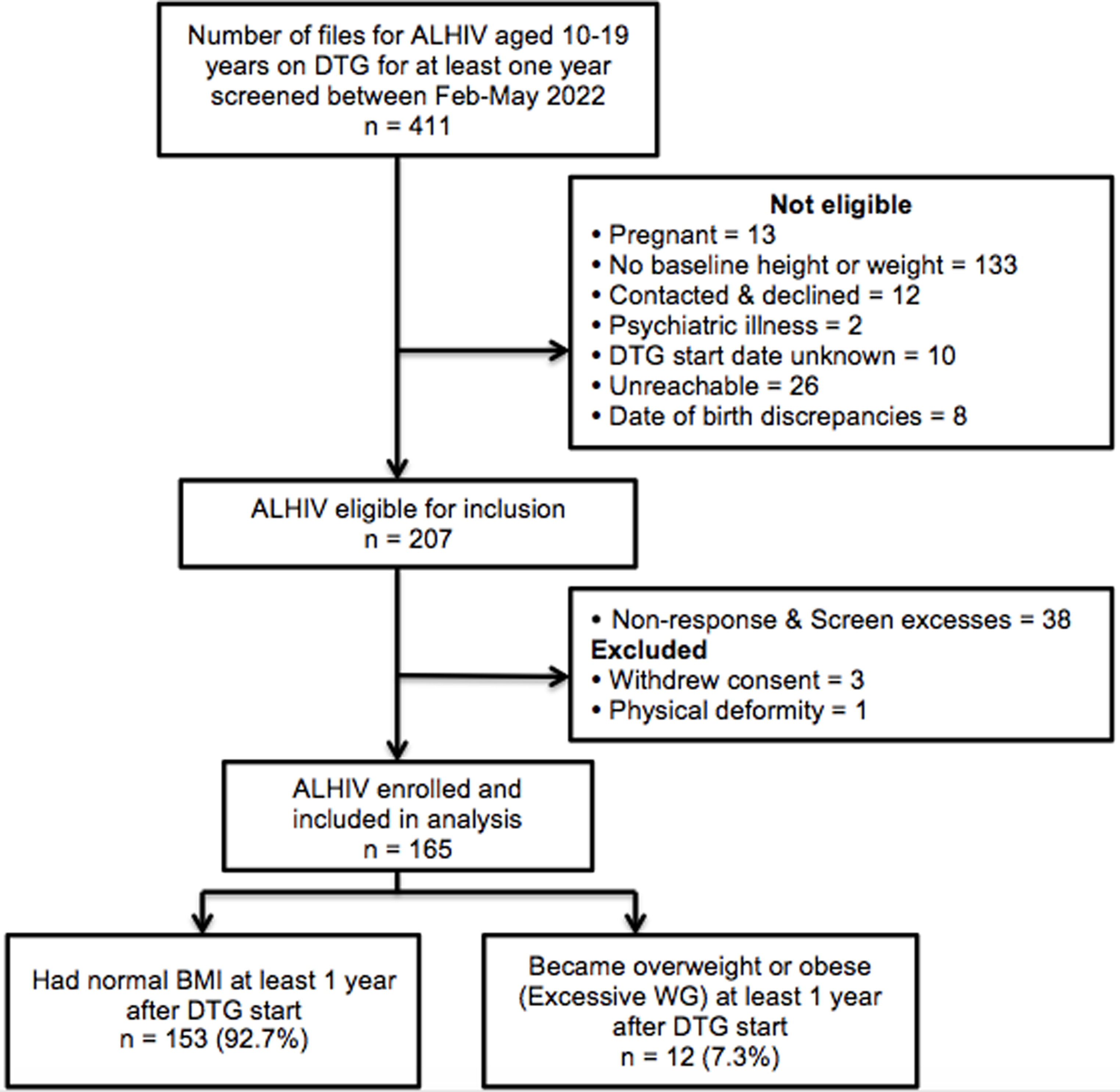
During the study, interviews were conducted with 38 WWID aged from 18 to 53 years old (with a median and mean age of 35 years). The group was stratified into four regions of the study: Kryvyi Rih city, Kyiv city, Ivano-Frankivsk, and Odesa regions.
The impact of War on well-being and living conditions
The majority of respondents (34) permanently lived in the research regions. Four respondents were forced to change their place of residence due to the loss of housing or the danger of martial law. Only 10 women lived alone; the remaining 28 shared housing with their parents, other close people, and/or male partners.
Deterioration of financial situation
All respondents noted changes in their usual lifestyle and well-being levels after the onset of the war. In January 2022, just before the war, the average personal income was 5,008 Ukrainian hryvnias (US$139), but by July 2022, it had decreased to 2,884 Ukrainian hryvnias per month (US$80). Most of them had lost their jobs even before the war, primarily due to drug use and health problems. Some had been financially dependent on their male partners for a long time. However, most of their husbands also lost their regular income due to the closure of enterprises in the winter and spring of 2022.
Women living in families with retired parents had a better financial situation, as the pension payments continued during the war. A significant proportion of the respondents received small social benefits, such as low-income or IDPs support, due to their own disabled status or a child’s disability. They also received irregular humanitarian aid from local authorities or volunteers. Temporary part-time jobs, such as seasonal vegetable sales, house cleaning, home sewing, and hairdressing services, served as additional sources of income. For several respondents, the only source of income was providing sexual services or participating in the drug trade.
Complication of life situation
In general, during the full-scale invasion, the living conditions of all interviewees became significantly more challenging due to a decrease in income, inflation (increased prices of transportation products), the risk of shelling and stress, increased drug costs, and a deterioration of living conditions. However, the significance of individual well-being factors varied in each case. Of particular importance to WWID during the war was the quality of relationships with family members, partners, and other loved ones. If the women had loved ones, then their connections support helped them endure the hardships of wartime.
A rocket hit our house, but from the other side, luckily. The windows were blown out. We didn’t replace them because we don’t have the money. We’re on ‘street methadone’, and we can barely afford to eat. I live with my boyfriend. He hardly walks. Lately, he understands me. – Kyiv, 36.
I have only one grandma left. I have friends, but when you have nothing, when your pockets are empty, then you’re not needed by anyone. My dear grandma helps me now, because things have become very tough. So, I’m very dependent on her now. – Odesa, 28.
Changes in drug use during wartime
The vast majority of respondents (35) had started injecting drugs before the full-scale war. Interviewees reported that changes in drug consumption mainly occurred in the first weeks of the war. An increase in the dose or frequency of drug use was primarily driven by heightened levels of anxiety, while a decrease was attributed to the difficulty of accessing drugs due to police and territorial defense control, as well as increased substances cost.
It used to be easier before. But now, even couriers are afraid to create drug stashes. It’s hard to transport them and hard to acquire – there are checkpoints everywhere. They punish severely for it. I don’t see a way out of all this. The prices have gone up. When the war started, it was around two thousand [hryvnias]. Before the war, it was six or seven hundred. – Odesa, 30.
Respondents noted the overwhelming extent of negative impact of drugs on their lives, namely on their physical and psychological state, relationships with significant people, and life prospects. However, among them there are individual participants who emphasize the positive consequences of drug use due to the reduction of stress, the opportunity to escape from uncertainty and fear during war.
War is a shock. War is fear. War is tragedy. And to survive this, to somehow come to your senses, I guess drugs are salvation, because when I use drugs, I forget about what’s happening in life right now. – Kyiv, 29.
Facilitators of engaging WWID in HIV testing, initiation of treatment, and retention on ARTSocial support
The presence of close relationships, support from relatives, encouragement from friends, or examples of loved ones, as well as support and accompaniment from social workers, were facilitators of accessing the entire cascade of HIV services. For a significant proportion of women, the first HIV testing took place alongside with friends, on the recommendation of volunteers and social workers at HIV/AIDS prevention sites, or during a medical examination (related to a specific somatic disease, a gynecological examination, or in places of imprisonment). If women had permanent connections with relatives, the facilitators for the initial test were often the example and encouragement of relatives (sisters, brothers) who lived with HIV. An important incentive for women to get tested for the first time was the recommendation of their male partners, who were HIV-positive or seriously ill.
The first person who conveyed this message to me was my husband as he neared the end of his life: ‘Get tested, unless it’s too late’. – Kyiv, 40.
Comparing the facilitators of starting ART in subgroups of women who learned about HIV infection before the war and did not start or started taking ART during the war, we found that the respondents of the second subgroup had stronger support from their loved ones and (or) motivation to care for their loved ones (child, parents, roommates). The support of trusted social workers was a significant motivator for them to start ART.
I discussed my need to get treatment with my husband. If I do not take ART, no one will be there to bring up my child. – Odesa, 28.
Relationships with the immediate environment, especially with partners, also facilitated the retention of WWID in therapy and their adherence to it. Taking care of loved ones and, at the same time, relying on their support in the challenging situation of war, women gained more motivation for treatment. In some cases, the breakdown of relationships led to a decrease in vitality and a devaluation of the need to take care for one’s life and continue treatment. The fear of discovering one’s HIV status due to taking ART may have also contributed to treatment discontinuation.
Taking ART is not for fear of oneself. My niece, my mom, they ask, ‘Please take it, what will we do without you?’. – Kryvyi Rih, 41.
One should never cease taking ART. However, I had a dispute with my husband, so I don’t care now. If I do not return home, I will not resume therapy. I don’t want anything at all now because I used to live for the sake of my family, and now I have no family. – Odesa, 35.
Support from social workers in HIV service NGOs was especially relevant for women who had lost family ties and were living in the worst conditions with limited material wealth. Participants of OST programs had more frequent contacts with social workers. Participation in OST programs was generally associated with increased awareness of HIV and contributed to the formation of intentions to start treatment.
I want to be on this program [OST] now. They called me from this organization. I feel like I have support. And if it helps me, then I will definitely go and get treatment. – Kryvyi Rih, 32.
However, as a whole, the attitudes of WWID toward OST were not unanimous. Approximately half of the respondents who received services at OST sites were committed to treatment and observed positive changes in their lives. They also reported the accessibility of HIV services. IDPs committed to OST enrolled in the program in their new place of residence, where they had more opportunities to access HIV services.
State of health and the threat of its loss
The risk of HIV infection and the timely initiation of HIV treatment were not equally relevant facilitators for receiving HIV services among different WWID subgroups. Other priorities took precedence in the lives of many during the war. Most of those who had not been tested for HIV previously or had a negative HIV status did not plan to be tested or were ambivalent about testing. As their drug use experience increased, some respondents became more aware of the risks associated with their lifestyle. Some mentioned they would consider testing only in the event of an immediate risk of HIV infection, such as unprotected sex or the risk of parenteral infection.
I didn’t think it was necessary to get tested before. I thought I was healthy, in general. Although now I believe that it’s necessary to get tested every year, well, in my case. – Ivano-Frankivsk, 33.
If you accidentally get pricked with a needle – it often happens to us, sometimes they throw them in the mailboxes. There are syringes without caps there. That’s the kind of situation when you could really catch something. – Kyiv, 26.
Poor health or the determination of viral load facilitated the initiation of therapy. However, as a result of improvements in immune system indicators and overall well-being, coupled with the influence of additional demotivating factors, some individuals discontinued treatment.
I saw that my test results were bad, and it probably contributed to starting ART. Then I noticed that my cell count hasn’t gone up or down in a couple of years, and I thought if I stop taking it, nothing bad will happen. I just didn’t want to keep ruining my body. Also, with drug use, there wasn’t any time; it just got too busy and all. – Kyiv, 41.
The interviews with WWID did not reveal key and universal individual facilitators for HIV detection, ART initiation, and retention in care during the war. In each case, a variety of circumstances and specific personal factors facilitated HIV testing, enrollment, and retention in HIV treatment. The most consistent personal facilitators for HIV services and commitment to ART were demonstrated by women who possessed a combination of several factors, including strong connections with relatives, responsibility for loved ones, family support, willingness to collaborate with specialists, a higher level of education, and a relatively prosperous financial situation. Among the social and organizational facilitators we studied, during wartime, the support and assistance of social workers from HIV services NGOs proved to be the most significant for WWID.
Barriers to seeking HIV testing services, treatment initiation and retention on ARTFear of HIV and social restrictions
Among the barriers to HIV testing, WWID most frequently cited the fear of learning their positive status, as it marks the beginning of living in constant anxiety about the future and facing the genuine threat of death. They believed that a positive HIV status would result in restrictions on sexual contacts, the disruption of relationships with loved ones, stigmatization, and a loss of life prospects. Respondents often avoided testing out of fear of a breach of confidentiality during the process and refrained from seeking treatment due to concerns that relatives might cease all communication upon learning about their illness. Given the heightened importance of permanent family and friend bonds during the war, the risk of losing them due to the revelation of a positive HIV status became an especially pertinent concern for some of the WWID.
This [positive HIV status] hits your self-esteem hard and you get demotivated. You don’t have that energy anymore. Everything seems futile in life. – Kyiv, 32.
If I tell everyone that I’m going to receive pills, that I have HIV, those few of my acquaintances who still have contacts with me will scatter. The girl in whose apartment I live will kick me out. – Kryvyi Rih, 32.
Drug use
This barrier, characteristic of both wartime and peacetime, becomes even more significant during times of danger such as war. Respondents noted that since the onset of the war, people have been turning to drugs more frequently as a way to cope with anxiety, causing them to care less about their own health and forego HIV testing. Many reports indicated that the war shifted priorities, making drugs more necessary but less accessible. Consequently, individuals focused primarily on finding drugs and often lacked the time to adhere to ART regimens regularly.
I think during the war, people started using more [drugs], and they do not care about their health or whether they have HIV or not. – Kyiv, 18.
It just slips your mind. You set different priorities. My way of life was such that I did not care if I take [ARТ] or not. Because it’s war, and I have a headache about where to get drugs, and here, I had to go for therapy too. – Kyiv, 41.
War-related stress
Among the barriers to initiating treatment, respondents also pointed to the onset of the war. However, in only a few cases could they specify the actual consequences of the war that hindered their ability to seek treatment, such as a lack of transport or money for travel. More frequently, women referred to circumstances they had heard from others (“they say the medical center was bombed”) or exaggerated the city’s difficult situation (“everyone is in bomb shelters, so they can’t access their medication”). Some respondents perceived the war as a threat, making it seem futile to prioritize their own health in the face of the broader crisis.
When the war started, I felt helpless, and I didn’t join the program, I didn’t start therapy. A person won’t even be able to safely go outside to get pills. – Kyiv, 36.
Nearly all respondents who had started ART before the war and discontinued it after February 24, 2022, cited the war as the primary reason for their treatment interruption. ART discontinuation mainly occurred in the early days of the war. Due to psychological stress or rumors about difficulties in obtaining medication, they did not renew their drug supply and subsequently did not seek healthcare facilities. Two respondents discontinued ART after changing their place of residence. In reality, this discontinuation was not due to limited access to the therapy but rather because of changes in their personal lives, such as deteriorating family relationships leading to apathy and indifference towards their health or the intention to conceal their HIV status from a new partner with whom they started living after relocation).
Distrust of medical professionals
WWID who learned about their positive HIV status before the war but did not initiate ART reported various circumstances that hindered them from starting treatment. If they learned of their HIV infection by chance during specific medical examinations (for the treatment of chronic diseases or preparation for the termination of a pregnancy), they did not always receive proper pre-test and post-test counseling. While they were advised to undergo retesting and begin ART, their distrust in the testing results or their shock upon learning their HIV positive status often deterred them from seeking further assistance from service organizations. Under martial law, the initial mistrust of medical workers increased even more. Respondents believed that their issues were of secondary importance to doctors, who were overwhelmed due to the large number of wounded patients and were unlikely to prioritize individuals with drug addiction. Women who had lost contact with their relatives felt entirely helpless in cases of deteriorating health or illness during the war. They were certain that medical care was not available to them and, as a result, saw no point in taking care of themselves.
During the war, it’s very difficult; there’s no time for ‘drug addicts’ and their problems now. I think any doctor would say I chose this path myself. There are a lot of wounded people now, and they have something to deal with. – Kyiv, 35.
Here’s the war, even if I feel really bad, I won’t call an ambulance. They won’t take me anyway. I’m not needed by anyone, so why bother. – Kryvyi Rih, 32.
Mistrust of health workers was also a barrier to consistent ART use. WWID most frequently mentioned treatment side effects (such as sleep disturbances, nausea, diarrhea, and dizziness) as hindrances to regular ART intake and adherence to treatment. Usually, treatment discontinuation occurred when WWID did not seek advice from doctors or did not follow their recommendations.
Quality of communication with medical professionals
The majority of WWID had a positively assessment of the quality of work and the availability of HIV prevention services. Women who had not previously been tested for HIV reported a lack of information about the health effects of HIV and where to get tested. However, one respondent emphasized that PWID are often disinterested in receiving this information and may neglect it. Additionally, during testing, they are frequently in a state of intoxication or abstinence, and the news of infection can be shocking, making them less able to fully comprehend the information received.
Complex barriers to accessing HIV services included medical personnel’s insufficient attention to the psychological state of women during testing, a lack of persistence in conveying information about the importance of testing and initiating ART upon receiving a positive HIV status, and a deficiency in sensitivity among medical workers regarding the individual needs of WWID.
Probably, there are enough brochures, leaflets, and booklets. But who has read them? I did not pay attention to it; I was never interested. – Kyiv, 53.
I was in a shock. I remember virtually nothing of what he was saying; I could not believe it can happen. – Kyiv, 29.
Some respondents erroneously believed that the testing procedure and subsequent examinations preceding ART were paid, although this is not true. In wartime conditions, aimed a significant deterioration in their financial situation, this misconception made it impossible for them to access services. In reality, the barrier to testing in this case was a gap in informing WWID and a lack of messages tailored to the characteristics of the target audience.
In order to get tested and find out, you have to pay 350 hryvnias. It’s tough for people now, you understand? And to find 350 hryvnias, you have to think about it, whether to buy food with them or go check your health. – Odesa, 28.
Violation of the operating hours of medical institutions
WWID, particularly those residing in remote rural areas, frequently encountered challenges related to registration and other bureaucratic procedures before commencing ART. These challenges became more pronounced during the war.
To start this therapy, one needs to get enrolled first. The red tape obstruction makes this process extremely slow. – Ivano-Frankivsk, 34.
At the onset of the war, changes occurred in work schedules, and there were alternations in medical staff teams at certain ART sites. These challenges resulted in overcrowding of patients who had wait for extended periods to see doctors and obtain their prescribed medications. Some respondents found it burdensome to make regular visits to health facilities and maintain contact with doctors, particularly air raid alarms and when public transportation was disrupted.
The queues for this therapy are insane. I would like to start taking ART again even now, for these services to me more accessible somehow, or even delivered by mail or in some other way. – Kyiv, 41.
Some WWID expressed concerns about potential interruptions in the supply of ART drugs during the war. They recommended increasing the quantity of drugs dispensed and organizing delivery to patients. Respondents also highlighted the need of support from social workers during registration process and suggested improving communications between various institutions providing HIV services.
Residing in rural areas
The danger of shelling and disruptions in transport communications during the war significantly affected the accessibility of HIV services, as it became challenging and sometimes impossible to reach medical institutions. This barrier was especially pertinent for women living in rural areas. Simultaneously, they had less access to information about HIV and comparatively fewer facilitators for testing and initiating of treatment than urban residents. They lacked social support, as HIV service NGOs workers, even before the war, primarily operated in cities, with only occasional visits to villages. Residents of remote rural areas also expressed dissatisfaction with the limited availability of OST programs and the lack of information about these programs. WWID who had lost contact with their relatives, faced worse financial situations, and had lower motivation to care for their health were more common in rural areas. Additionally, compared to city residents, WWID living in the countryside during the war were more likely to report fears of stigmatization from fellow villagers and feelings of guilt and shame as barriers to initiating therapy and maintaining adherence.
I didn’t make it [to the ART site]. I heard about it only once, somewhere. The workers from the NGO haven’t registered us. Can you imagine what would happen if they found out? It’s a small village. – Odesa, 40.









留言 (0)