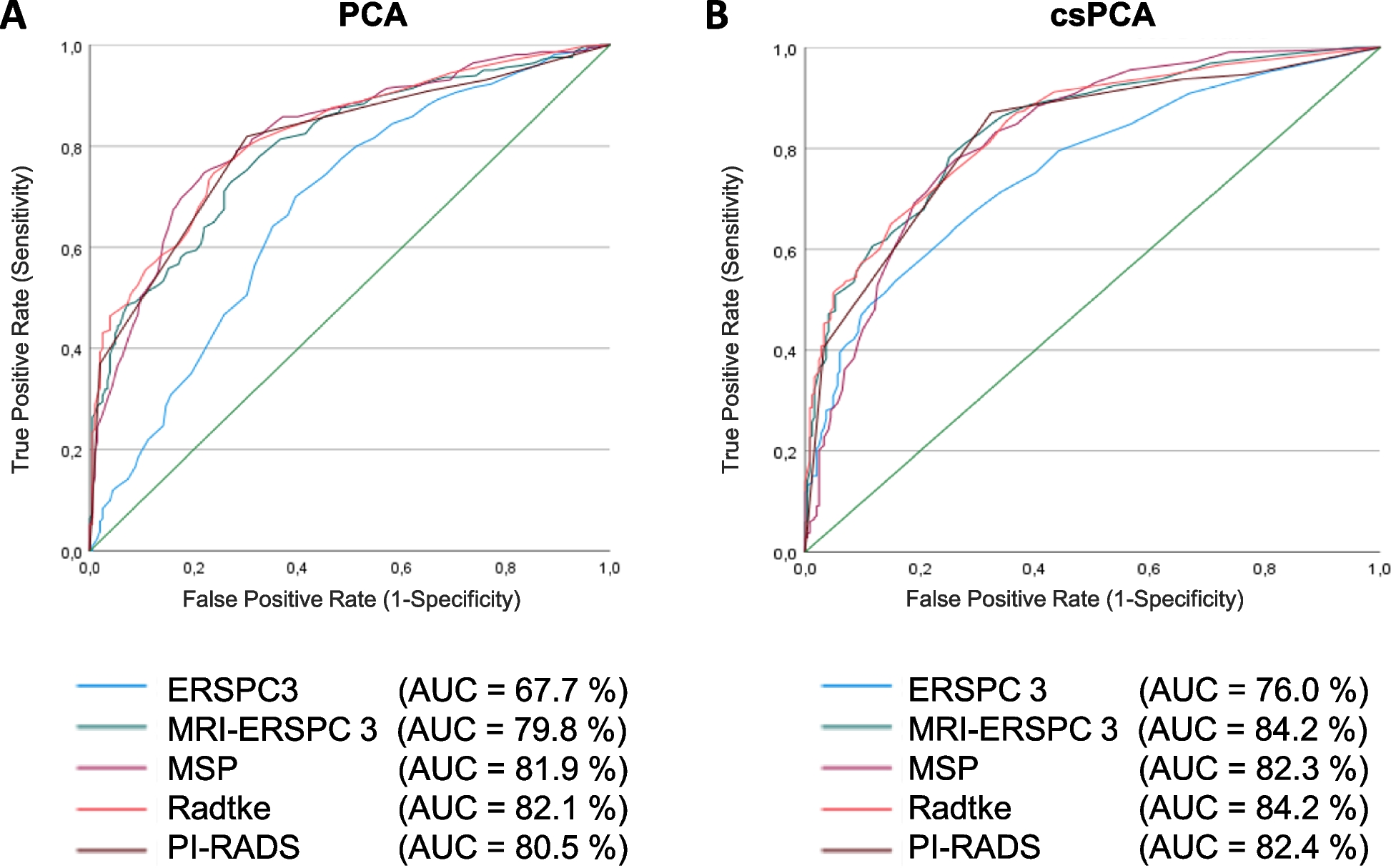
Our study revealed that women with IC/BPS exhibited a significantly elevated neutrophil-to-lymphocyte ratio (NLR) compared to healthy individuals, and this distinction remained significant when compared to patients with overactive bladder (OAB). Through ROC analysis, we established that NLR possesses substantial diagnostic utility in discriminating between IC/BPS and OAB, as well as in distinguishing IC/BPS patients from those without the condition. Additionally, we identified a positive and statistically significant correlation between NLR and the symptom scales ICPI and ICSI, suggesting the potential of NLR as a symptom marker in IC/BPS patients. These findings imply that NLR holds promise as a marker for assessing symptoms in individuals with interstitial cystitis and offers a non-invasive diagnostic approach for detecting IC/BPS.
In previous investigations, potential biomarkers for IC/BPS have encompassed NGF, chemokines, inflammatory mediators, and particular antiproliferative agents. Within the urethra, NGF emanates from the smooth muscle of the bladder and the urothelium [21]. Jacobs et al. [22], discerned heightened urinary NGF levels in individuals with neurogenic bladder and central bladder symptoms. Women grappling with bladder dysfunction, encompassing idiopathic sensory urgency, chronic cystitis, and IC/BPS, manifested increased bladder NGF immunoreactivity in comparison to their counterparts without distressing symptoms, which included women with stress urinary incontinence [23]. Nevertheless, it’s imperative to note that urinary NGF levels also surge in cases of urinary tract infections, bladder outlet obstruction, and urinary calculi [24]. The usage of NGF as a biomarker for IC/BPS is hindered by its lack of specificity, making it inadequate for distinguishing these conditions from IC/BPS. Furthermore, quantifying NGF necessitates a more intricate technique, ELISA.
Chemokines exert their effects by interacting with seven-transmembrane G protein-coupled receptors situated on glycosaminoglycans tethered to the endothelial cell layer [25]. These chemokines are not limited to inducing chemotaxis but also have the capacity to activate target cells within the bladder, thereby contributing to the inflammation-driven alterations seen in IC/BPS. In a cross-sectional study, the hypothesis that urinary levels of specific chemokines are elevated in IC/BPS patients was tested. The findings revealed that urinary levels of chemokines/cytokines were 10–100 times higher in patients with both Hunner-type interstitial cystitis (HIC) and non-Hunner-type interstitial cystitis (NHIC) in comparison to asymptomatic controls [26]. JIANG et al. [27] observed that serum Scr levels, NGF, and pro-inflammatory cytokines/chemokines, such as IL-1β, IL-6, TNF-α, and IL-8, were significantly higher in IC/BPS patients than in the control group. The heightened levels of these pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) and chemokines (IL-8) in the serum of IC/BPS patients not only suggest mast cell activation but also underline the significance of other inflammatory mediators in the pathogenesis of IC/BPS. Nevertheless, the application of inflammatory factors for diagnosing IC/BPS lacks specificity and is not suitable for widespread use.
A particular antiproliferative factor (AFP) has been identified in the urine of IC/BPS patients. AFP is the most extensively investigated biomarker and exhibits remarkable specificity and sensitivity [28]. Nevertheless, there is currently no evidence supporting the utilization of AFP for early detection of IC/BPS.
Neutrophils play a pivotal role in the innate immune response, carrying out essential functions like phagocytosis and releasing a multitude of cytokines and molecular mediators. The presence of lymphocytopenia is a hallmark of stress, while inflammation stems from processes like demargination, redistribution, and accelerated apoptosis. The neutrophil-to-lymphocyte ratio (NLR) serves as a valuable metric that reflects the equilibrium between the innate and adaptive immune responses. Consequently, NLR emerges as an exceptional indicator of both inflammation and stress, effectively capturing the intricate interplay between the two [29]. The underlying mechanism driving neutrophilia involves the activation of stem cell growth factor, which exerts its influence on neutrophil production [13]. In the early phases of an inflammatory response, the tumor necrosis factor family triggers apoptosis in lymphocytes, thus establishing lymphocytopenia as a diagnostic marker of infection [30]. Neutrophils possess the ability to release reactive oxygen species and an array of peptides, including antimicrobial peptides. These components contribute to the formation of neutrophil extracellular traps, which, unfortunately, exert adverse effects on the bladder [31]. In a comprehensive epidemiological study conducted by Lee et al. in 2018, a robust cohort comprising 12,160 healthy Korean citizens (6,268 men with a median age of 47 years and 5,892 women with a median age of 46 years) was meticulously examined. The researchers analyzed 12,160 blood samples that had undergone routine complete blood count assessments. The mean NLR value was (1.65 ± 0.79) [32]. Zahorec proposed NLR categorizations as follows: Latent, subclinical, or mild inflammatory/stress conditions: NLR range 2.3-3.0; Mild to moderate inflammation: NLR range 3–7; Moderate to severe inflammation, systemic infection, sepsis, and SIRS: NLR range 7–11; Severe inflammation, infection, severe sepsis and SIRS, and bacteremia: NLR range 11–17 [29]. In simpler terms, elevated NLR values are directly associated with conditions characterized by severe inflammation, stress, injury, trauma, major surgery, or cancer. These elevated NLR values indicate a worsening prognosis, signifying a higher likelihood of unfavorable outcomes in terms of illness or death.
NLR, as an objective measurement, can be readily derived from standard blood tests commonly conducted in clinical settings. Furthermore, in comparison to currently employed biomarkers, NLR presents itself as a cost-effective, easily obtainable, and readily calculable parameter. Therefore, introducing NLR into clinical practice is a feasible prospect. Our study suggests that NLR holds the potential to serve as a non-invasive diagnostic tool and a symptom indicator for interstitial cystitis, effectively distinguishing it from overactive bladder.
This study has a few limitations that warrant discussion. Firstly, the study’s cross-sectional nature restricts the establishment of causality between IC/BPS and NLR elevation, as the order of their occurrence cannot be ascertained. Future research adopting a prospective design and conducting multiple NLR measurements could yield more substantial evidence regarding NLR’s role in diagnosing IC/BPS. Secondly, it is conceivable that unmeasured covariates might have confounded the relationship between elevated NLR and IC/BPS. However, as the seemingly healthy individuals were selected from the general population, this potential confounding effect appears to have been mitigated. Thirdly, there is a possibility of bias, as various factors can influence the results of a routine blood test. Nevertheless, our random selection approach may have minimized some of the chance-related effects when screening the healthy control groups.
This study possesses several noteworthy advantages. Firstly, it stands as the inaugural examination of the correlation between NLR and IC/BPS. Secondly, our study utilized validated and widely accepted tools, namely the Interstitial Cystitis Symptom Index and Interstitial Cystitis Problem Index, to assess the IC status, enhancing the robustness and reliability of our findings.







留言 (0)