
Remember me




The nipple is a small protuberance in the center of the areola at the summit of the breast, through which the lactiferous ducts open to the skin surface, enabling the drainage and suction of milk during breastfeeding in mammals. Given its unique tissue constituents, a wide variety of cutaneous and mammary lesions may occur at this site ranging from inflammatory processes to benign and malignant tumors. This review provides an update on the clinical, pathologic, and immunophenotypic features of nipple lesions of the breast, with a discussion of the most common and/or challenging differential diagnosis. The molecular alterations underpinning nipple adenoma are included, but molecular data on other nipple neoplasms is almost inexistent.
EMBRYOLOGY OF THE MAMMARY GLANDThe mammary gland is an epidermal appendage derived from apocrine sweat glands.1 During embryogenesis, the ventral ectoderm thickens along “milk lines” that stretch between the front and rear limb buds bilaterally. Depending on the mammalian species, mammary buds form where the nipples will later develop, while the rest of the milk line disappears. In humans, each mammary line regresses completely except for a single site on both sides of the chest. The mammary gland develops from the residual mammary bud through a process of invagination, cavitation, and duct branching. Canonical Wnt signaling is essential for mammary gland morphogenesis.2 Occasionally, supernumerary nipple(s) and ectopic breast tissue develop along the milk line if the latter did not regress completely. In females, further growth and development of the mammary lobules occur during puberty and in pregnancy, culminating with the secretion of milk post-partum, enabling breastfeeding, which is the main function of the mammary gland. Males also develop nipples and rudimentary mammary glands consisting only of a few ducts in fibrous stroma and usually devoid of any terminal-duct lobular units. While most inflammatory and function-related alterations of the nipple typically occur in females, neoplastic processes can affect any sex and may also arise in remnants of the milk line.
ANATOMY OF THE NIPPLEThe nipple is the cutaneous protuberance through which the lactiferous ducts that drain the underlying mammary gland open onto the skin (Fig. 1). Elegant studies using serial sectioning and tridimensional digital reconstruction of nipples with no pathologic abnormalities obtained from risk-reducing mastectomy specimens found a median of 23 nipple ducts closely aligned in a central bundle that narrows to a waist just beneath the skin, roughly along a line that separates the nipple from the retroareolar breast tissue. Below this line, the lactiferous ducts expand slightly into the lactiferous sinuses. At the summit of the nipple, the nipple ducts drain through inconspicuous orifices. Tridimensional reconstruction of the tip of 1 nipple demonstrated 15 orifices draining 29 ducts.3 The nipple is in the middle of the areola, a ring of thin and pigmented skin, and together they are often referred to as nipple-areola complex (NAC). The NAC is devoid of hair follicles, with sparse pilosebaceous units usually present around the areola. The NAC is rich in sebaceous glands. The skin of the areola often shows small bumps (1 to 2 mm) (Morgagni tubercles) that represent the openings of the ducts of prominent sebaceous glands (Montgomery glands). The sebaceous glands of the nipple become more prominent in pregnancy and during breastfeeding since they help lubricate the areola during lactation. No eccrine glands are found in the nipple. In ~10 to 12% of cases, the epidermis at the summit of the nipple contains scattered bland glandular cells, known as Toker cells (see the section on Paget disease for a detailed discussion of Toker cells). The stratified squamous epithelium of the NAC extends into the terminal portion of the nipple ducts for 1 to 2 mm4 (Fig. 2). More extensive squamous metaplasia may cause accumulation of keratin within the ducts and duct plugging. The dermis of the NAC is rich in smooth muscle fibers and has sensory nerve endings. The deep aspect of the nipple harbors a rich lymphatic network (Sappey’s plexus).5
 FIGURE 1:
FIGURE 1: Anatomy of the nipple-areolar complex (submacroscopic, hematoxylin and eosin).
 FIGURE 2:
FIGURE 2: Transition of the stratified squamous epithelium to the glandular epithelium of a nipple duct (×40, hematoxylin and eosin).
SQUAMOUS METAPLASIA OF THE LACTIFEROUS DUCT (SMOLD) OverviewSMOLD is an uncommon breast disease. Other terms used for this disease, especially for advanced manifestations, include Zuska’s disease (after Dr Joseph J. Zuska, who first described this condition in 1951), recurrent subareolar abscess, and periductal mastitis.4,6–12 SMOLD may affect women and men from a wide age range. Smoking, especially cigarette smoking, is the primary risk factor. The byproducts of smoking are thought to promote keratinizing squamous metaplasia of the lactiferous ducts leading to dilatation of the ducts and keratin plugging, followed by duct rupture with extravasation of keratin into the periductal stroma, which promotes acute and chronic periductal inflammation with abscess formation.13 Decreased levels of beta-carotene occurring in smokers have also been suggested to promote squamous metaplasia of the ducts.14 SMOLD is also a possible complication of nipple inversion or piercing, thus suggesting that also mechanical factors could have a pathogenetic role.15
Clinical FeaturesSMOLD usually affects females but may rarely occur also in men.16 It presents as a red, painful nodule of the NAC. Purulent nipple discharge is common. In some cases, the abscess drains through a fistula in the areola. Typically, the patient is a chronic smoker and may report prior similar episodes.17–19 Clinically, the differential diagnosis may include intraductal papilloma or an abscess associated with breastfeeding or breast malignancy.19–22 SMOLD usually appears as a mammographic retroareolar asymmetric density and an ill-defined hypoechoic lesion with increased vascularity.19
In most cases, antibiotic therapy alone is inadequate to cure SMOLD, and only surgical excision may eradicate this condition together with smoking cessation;15 the latter may also reduce the recurrence of the disease.19 Although rare case reports have suggested that squamous cell carcinoma may develop in the context of SMOLD/Zuska’s disease, the possibility of delayed diagnosis of the carcinoma cannot entirely be ruled out.
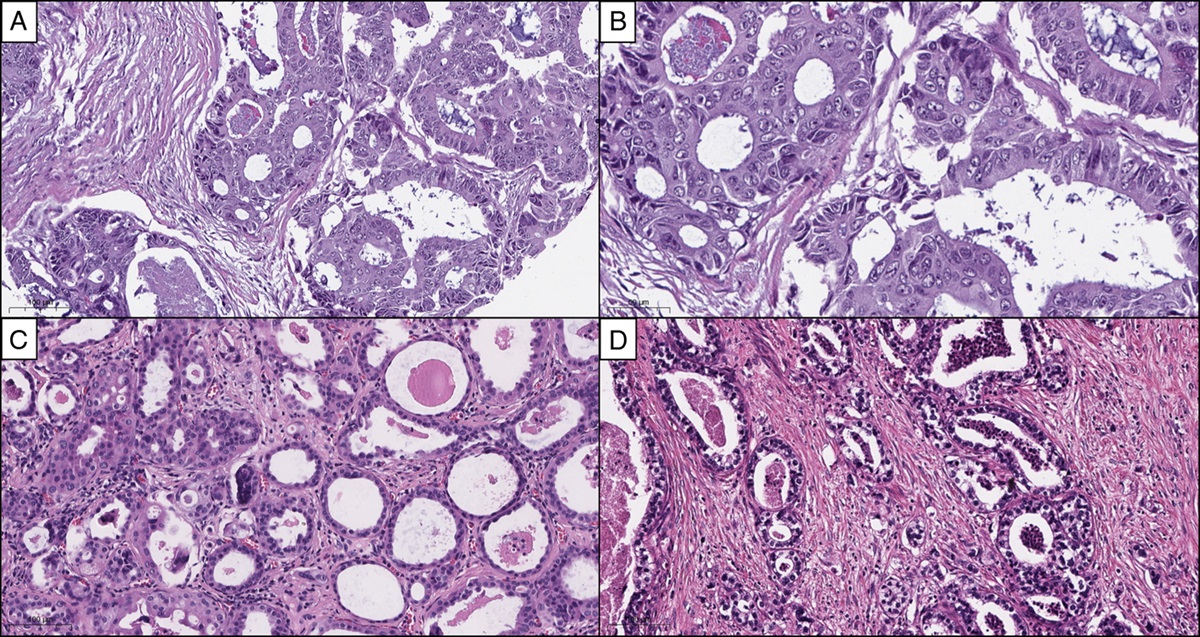
HistopathologyThe specimen shows a mixed inflammatory infiltrate composed of lymphocytes, plasma cells, and neutrophils with scattered giant cells admixed with keratin debris. Immunohistochemical staining for high-molecular-weight cytokeratins (CK5/6, CK14) highlights keratin debris in the inflammatory infiltrate and within the giant cells. In the appropriate clinical setting, these findings strongly support the diagnosis of SMOLD. Squamous metaplasia may be difficult to identify in small, unoriented incisional specimens but usually is evident in resection specimens (Fig. 3A-D). Toker cell hyperplasia in the epidermis overlying SMOLD has recently been described. The authors suggested that inflammation may trigger the proliferation of Toker cells,23 but this hypothesis requires further validation.
 FIGURE 3:
FIGURE 3: SMOLD, squamous metaplasia identified in a small biopsy (A, ×20; B, ×100; hematoxylin and eosin), surrounded by a marked inflammatory infiltrate composed of lymphocytes, plasma cells, neutrophils, and giant cells (C,× 200; hematoxylin and eosin) with keratin debris (D, ×100, CK5/6 immunostaining).
Differential DiagnosisThe differential diagnosis of SMOLD includes epidermal inclusion cyst and duct ectasia. While an epidermal inclusion cyst typically occurs in the dermis, SMOLD develops just below the nipple and in continuity with lactiferous ducts. Duct ectasia is not associated with squamous metaplasia, and no keratin debris is present in the inflammatory reaction.
DUCT ECTASIA OverviewDuct ectasia (also previously known as plasma cell mastitis or comedomastitis)24 is secondary to the weakening and disruption of the elastic lamina around the lactiferous ducts, which leads to stasis and accumulation of intraductal secretion, with subsequent rupture of the duct wall. Leakage of the inspissated secretion into the stroma induces the inflammatory response and periductal fibrosis.
Clinical FeaturesDuct ectasia usually occurs in multiparous peri-postmenopausal women24 and does not affect males. Rare examples have been reported in children, but the pathogenesis is not established.25 It presents as a palpable subareolar mass, often associated with thick nipple discharge, which is only rarely bloody. Nipple retraction and skin tethering may mimic a malignant process. Since multiple ducts may be affected, duct ectasia may appear clinically and grossly as a firm, ill-defined area. Ultrasound may show duct dilatation, abscess collection, or mixed cystic and solid mass.
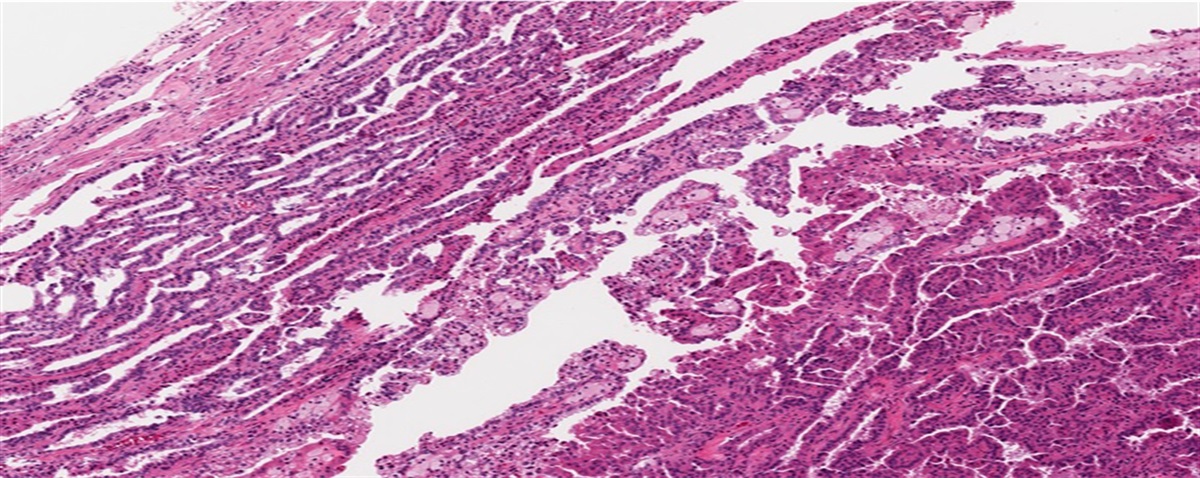
HistopathologyThe lactiferous ducts are ectatic, filled with abundant amorphous granular secretion, and surrounded by a mixed inflammatory infiltrate composed of lymphocytes, plasma cells, and neutrophils. Foamy histiocytes are commonly found in the cystic lumen and within the wall of the affected ducts. Multinucleated giant cells are also present, but well-developed granulomas are not a feature. Periductal fibrosis may be marked and lead to occlusion of the ducts in late-stage lesions, so-called mastitis obliterans (Fig. 4A-C). In some cases, partial recanalization of the ducts by small peripheral epithelium-lined conduits may occur (Garland sign).
 FIGURE 4:
FIGURE 4: Duct ectasia, a lactiferous duct filled with foamy histiocytes (A, ×200, hematoxylin and eosin), surrounded by a mixed inflammatory infiltrate composed of lymphocytes, plasma cells and neutrophils (B, ×40, hematoxylin and eosin), and marked periductal fibrosis in late-stage lesions (C, ×40, hematoxylin and eosin).
Differential DiagnosisThe differential diagnosis includes SMOLD and/or a breast abscess. Acute and chronic inflammation associated with keratin debris is the dominant feature of SMOLD. Purulent inflammation characterizes a breast abscess, which may occur primarily during lactation or secondary to SMOLD.
Duct ectasia is a specific clinical and histologic entity, and this term should not be used improperly to diagnose dilated ducts outside the specific clinical context, for example, if dilated ducts containing foamy histiocytes are identified in a mammary resection specimen obtained post-neoadjuvant chemotherapy.
NIPPLE ADENOMA OverviewNipple adenoma is a benign glandular proliferation of the superficial lactiferous ducts within the nipple. Many different names have been used in the past for this entity, including florid papillomatosis of the nipple, erosive adenomatosis of the nipple, nipple duct adenoma, subareolar papillomatosis, superficial papillary adenomatosis and papillary adenoma of the nipple;26–32 nipple adenoma is the term favored in the latest classification of the tumors of the breast33. Nipple adenoma is rare and can occur in both sexes and over a wide age range, including children, but is most common in middle-aged women. In the largest series published to date, the patient mean age ranged from 38 to 56 years (Table 1).
TABLE 1 - Nipple Adenoma: Clinicopathologic Features References Cases Sex Mean age years (range) Symptoms duration Signs & symptoms Mean size mm (range) Morphologic patterns Jones DB26 5 F 56.2 (28–70) 1 m–4 y 4 erosionNA indicates nipple adenoma.
Nipple adenoma usually is unilateral. Most cases present with nipple erosion and serous or bloody exudate, closely mimicking Paget disease. The exudate is often described as “nipple discharge,” raising the differential diagnosis of an underlying intraductal papilloma or carcinoma. In a contemporary series40 69% of patients with clinical information were symptomatic, and the most common symptom was bloody nipple discharge (24% of patients). In another series, 83% of patients39 had nipple erosion and discharge. Fewer than 10% of patients reported nipple pain or itching.39,40 Thickening of the epidermis, erythema, and ulceration associated with a nipple adenoma may also suggest a benign cutaneous lesion such as eczema or psoriasis, or an infectious process,41 prompting initial treatment with topical antibiotics and/or steroids without resolution of the lesion. Given these presenting symptoms, most nipple adenomas are detected when the tumor has a relatively small size and consists of a superficial palpable nodule. The tumor size is usually less than 1 cm (range 0.5 to 1.5) (Table 1). Reports of large nipple adenomas that protruded from the nipple may have been prolapsed intraductal papillomas. Nonetheless, the reported duration of symptoms ranges from 1 to 2 months to many years. In 1 series, the mean duration of symptoms was 10 months, and 3 patients reported having symptoms for 15, 10, and 10 years, respectively.35 In a contemporary series, the duration of symptoms also ranged from 3 months to 10 years, with a mean of 2.5 years.39 Imaging studies usually are inconclusive. Mammography may identify a superficial nipple mass. By ultrasound examination, nipple adenoma may appear as a hypoechoic, irregular mass, an intraductal lesion or duct dilatation, abnormal texture of the nipple, or even as a nonspecific hypervascularity.40 In most cases, a skin punch biopsy or a small incisional biopsy of the lesion is obtained for initial evaluation. If Paget disease is suspected clinically and only a shave biopsy of the eroded skin is obtained, the specimen may be too superficial and inadequate to diagnose nipple adenoma.
HistopathologyMicroscopically nipple adenoma consists of a nodular proliferation of small glands and ductules associated with a lactiferous duct. It is well-circumscribed but not encapsulated42 (Fig. 5). The glandular epithelium frequently extends to the surface of the nipple and replaces the squamous epithelium, with resulting erosion of the nipple surface, inflammation, and serous to bloody exudate (Fig. 6A-B). The glandular epithelium is often hyperplastic and micropapillary or arranged in papillae. Focal necrosis and mitoses may be present, but in the absence of cytologic or architectural atypia, they are not indicative of malignancy (Fig. 7A-B). Moreover, the myoepithelium is uniformly preserved.43 Investigators have described different morphologic patterns of nipple adenoma, but the different patterns often coexist in the same case. Rosen and Caicco described 4 major morphologic patterns35 (Fig. 8A-E):
Adenosis pattern: a nodular proliferation of small ducts resembling adenosis with or without stromal sclerosis. Apocrine metaplasia is common in this pattern. The differential diagnosis includes well-differentiated invasive ductal carcinoma and adenosis. Papillomatosis pattern: this pattern is characterized by large ducts with papillary growth. The glandular epithelium often extends to the surface of the nipple, causing erosion and ulceration. The glands and ducts often show usual ductal hyperplasia that can be florid, with focal central necrosis. The differential diagnosis in these cases often includes ductal carcinoma in situ. Sclerosing papillomatosis pattern: this pattern is characterized by papillary growth in large ducts that are distorted by stromal fibrosis with abundant collagen deposition, elastosis and/or myxoid changes. Keratin cysts may be present within duct orifices. This pattern may mimic invasive carcinoma. Mixed pattern: a combination of any of the patterns described above. FIGURE 5:
FIGURE 5: Nipple adenoma, a well-circumscribed proliferation of small glands and ductules (×20, hematoxylin and eosin).
 FIGURE 6:
FIGURE 6: Nipple adenoma, the glandular epithelium replaces the epidermis with erosion of the nipple surface (A, ×100, hematoxylin and eosin; B, ×100, ADH-5 immunostaining).
 FIGURE 7:
FIGURE 7: Nipple adenoma, florid usual ductal hyperplasia with focal necrosis (A, ×200, hematoxylin and eosin) and epithelial mitoses (B, ×200, hematoxylin and eosin) may be present.
 FIGURE 8:
FIGURE 8: Nipple adenoma, adenosis pattern (A, ×200, hematoxylin and eosin) with apocrine metaplasia (B, 100x, hematoxylin and eosin), papillomatosis pattern (C, ×100, hematoxylin and eosin), sclerosing papillomatosis pattern (D, ×100, hematoxylin and eosin) with superficial keratin cysts (E, ×40, hematoxylin and eosin).
In a contemporary series, however, different morphologic patterns could not be easily subclassified, and more importantly, the different patterns had no clinical correlation.40
Nipple Adenoma and Other LesionsToker cell hyperplasia may be present in the epidermis overlying nipple adenoma.44 Rarely nipple adenoma is associated with carcinoma. The occurrence of DCIS in a nipple adenoma is exceedingly rare, but DCIS may be present in an adjacent duct (Fig. 9A-B). In contrast, invasive carcinoma occasionally may arise in association with nipple adenoma, including low-grade adenosquamous carcinoma (LG-ASC), and invasive carcinoma of no special type (invasive NST). Gobbi et al reported 3 cases of carcinoma associated with nipple adenomas as having “features of both spindle cell metaplastic tumor and syringomatous adenoma.”44 These might have been examples of LG-ASC or carcinomas with low-grade metaplastic spindle cells and squamous components, not fulfilling the strict diagnostic criteria of fibromatosis-like metaplastic carcinoma (FL-MC).
 FIGURE 9:
FIGURE 9: Nipple adenoma and DCIS involving adjacent but separate ducts (A, ×40; B, ×100; hematoxylin and eosin).
Differential DiagnosisThe differential diagnosis includes “benign breast”, syringomatous tumor of the nipple (SyT), syringocystadenoma papilliferum, tubular adenoma, intraductal papilloma, Paget disease and invasive carcinomas, including invasive NST, and special subtypes, such as LG-ASC, and possibly FL-MC.
In small and/or superficial biopsy material, the identification of benign mammary glandular elements in the superficial dermis, immediately below the epidermis, is diagnostic of nipple adenoma and should not be reported simply as “benign breast”, a statement that albeit technically correct, does not account for the lesion sampled.
Nipple adenoma with predominantly papillary architecture may resemble syringocystadenoma papilliferum, a rare benign apocrine neoplasm composed of 2 layers of cells (luminal and basal layers) arranged in papillae and cystic spaces that connects focally to the epidermis/hair follicles and is often associated with a dense plasmacytic infiltrate. Syringocystadenoma papilliferum occurs most frequently in the scalp and face, and only rare examples are described in the nipple, including 1 in a 23-year-old male.45,46 Squamous metaplasia and keratin cysts are more common in syringocystadenoma papilliferum than in nipple adenoma, in which keratin cysts are exceedingly rare and usually restricted to the superficial portion of the lesion. Central papilloma may mimic a nipple adenoma, and some case reports of extremely large nipple adenomas are suggestive of pedunculated intraductal papillomas protruding from the nipple duct orifice. Central intraductal papillomas arise within the lactiferous ducts and are not in continuity with the overlying epidermis (Fig. 10). Morphologically, central papilloma consists of fibrovascular cores covered by epithelium and a continuous layer of myoepithelium. The proliferation of the epithelium of papilloma is common, ranging from usual ductal hyperplasia to atypical ductal hyperplasia and ductal carcinoma in situ.47 In contrast to invasive carcinoma, nipple adenoma usually has a nodular and circumscribed outline and lacks peripheral infiltration. Immunohistochemical stains for myoepithelial markers can be used to resolve this differential diagnosis.
 FIGURE 10:
FIGURE 10: Intraductal papilloma in a lactiferous duct (×20, hematoxylin and eosin).
Paget disease with superficial erosion is a close mimic of erosive nipple adenoma but consists of neoplastic glandular cells (see the section on Paget disease). The glands of invasive NST are devoid of myoepithelium and infiltrate the adjacent tissue, whereas the glands and tubules of nipple adenoma have a nodular arrangement and are surrounded by a continuous myoepithelial layer. SyT and LG-ASC are also in the differential diagnosis (see sections below).
Molecular AlterationsInformation about the molecular alterations of nipple adenoma is very limited. In 1 study, activating PIK3CA mutations were identified in 12/24 cases and consisted of PIK3CA H1047R in 11 cases.38PIK3CA H1047R coexisted with KRAS Q61H in 1 case. Troxell et al previously identified the same combination of genetic alterations in an atypical papilloma and in an invasive papillary carcinoma.48 Furthermore, these molecular findings and the tumor morphology (classified as “adenosis-like” and illustrated in 1 of the figures) raise the possible differential diagnosis of adenomyoepithelioma. Another 2 nipple adenomas harbored BRAF V600E mutations.38 These results are intriguing and highlight the need for additional information on the genetic alterations underpinning nipple adenoma.
ManagementComplete excision of nipple adenoma is curative and is generally regarded as necessary to prevent a possible recurrence, although the latter is exceedingly uncommon. Complete excision is also intended to rule out the rare possibility of an associated in situ or invasive carcinoma35,36 (see the section on invasive carcinoma). Even if the risk of recurrence or subsequent carcinoma is extremely low, clinical follow-up is advised.
SYRINGOMATOUS TUMOR OF THE NIPPLESyT of the nipple was first described in 1983 by Dr Paul P. Rosen as syringomatous adenoma of the nipple,49 but the WHO expert consensus group recommends classifying this neoplasm as a tumor due to its locally infiltrative nature.33 Although microscopically SyT resembles cutaneous syringoma, a tumor of the eccrine glands, it arises from progenitor cells in the lactiferous ducts and is unrelated to cutaneous syringoma.50 In addition, the nipple is devoid of eccrine glands.
Clinically SyT presents as a firm nodule in the dermis of the nipple, in the nipple itself and/or subareolar region. It is often associated with nipple discharge, tenderness, or itching. The tumor diameter varies in size from 5 to 4 cm, but some of the larger tumors may have been examples of LG-ASC. The clinical differential diagnosis usually includes nipple adenoma and carcinoma, while Paget disease is rarely a consideration. Due to its location in the superficial aspect of the nipple, SyT is usually undetected by mammography and/or ultrasound. It may appear as a mass-like enhancement at magnetic resonance imaging.33,51
HistopathologyMicroscopically, SyT is characterized by cells with glandular and squamous morphology arranged in glands, tubules, or typically, in elongated, comma-shaped nests.49 Nuclear atypia is absent. If any atypia is present, the differential diagnosis of LG-ASC needs to be excluded. Mitoses are uncommon, and apoptotic figures are not observed. SyT is a benign yet infiltrative neoplasm and invades the wall of the nipple ducts. Rarely may it extend into the smooth muscle fascicles of the areola or around nerves or in the most superficial aspect of the retroareolar breast tissue. Despite its infiltrative growth, SyT is not associated with stromal desmoplasia (Fig. 11). SyT is negative for Estrogen receptor (ER), progesterone receptor (PgR) and has extremely low Ki67 index. The most challenging differential diagnosis of SyT is with LG-ASC.
 FIGURE 11:
FIGURE 11: Syringomatous tumor, tubules and comma-shaped nests of glandular and squamous cells invade the nipple-areolar complex without stromal desmoplasia (A,×20, hematoxylin and eosin); no overt nuclear atypia and mitotic figures are present (B, ×100, hematoxylin and eosin). Courtesy of Dr Dilip Giri, Department of Pathology and Laboratory Medicine, Memorial Sloan Kettering Cancer Center, New York City, NY.
LOW-GRADE ADENOSQUAMOUS CARCINOMA (LG-ASC)LG-ASC is a rare subtype of metaplastic mammary carcinoma. It is most common in perimenopausal or postmenopausal women but can occur at any age. Men are rarely affected. LG-ASC may occur anywhere in the breast but often arises in the nipple and/or retroareolar tissue. Usually, it presents as a palpable mass but may be an incidental finding at mammographic screening. Nipple discharge can be a presenting symptom. The average tumor size is about 2.0 cm (range 0.5 to 5.0). LG-ASC often arises in association with sclerosing lesions (such as a radial scar or complex sclerosing lesion) or myoepithelial-rich tumors, such as papilloma and adenomyeopithelioma, and has been reported to arise in association with nipple adenoma.52
LG-ASC consists of infiltrating tubules, glands, squamous nests, and cysts. The neoplastic epithelium has low to intermediate-grade nuclear atypia, apoptosis, and scattered mitoses. The epithelial elements are embedded in desmoplastic stroma composed of plump spindle cells with lamellar distribution. Small lymphocytes are scattered throughout the tumor and often form tightly nodular aggregates at the tumor periphery. LG-ASC usually is negative for ER, PgR, and human epidermal growth factor receptor 2 (HER2) and is not HER2/ERBB2 amplified. Immunohistochemical studies have documented that the ducts and glands of LG-ASC consist of an inner luminal epithelial layer and a peripheral basal/myoepithelial layer, although the latter may be complete, incomplete, or focally absent. The “consistently inconsistent” distribution of the myoepithelium can be highlighted with immunohistochemical stains for myoepithelial markers. In particular, we find p63 staining to have unique diagnostic utility, as it highlights the squamous epithelial nests and also the basal/myoepithelial cells around the neoplastic glands/tubules as a complete or incomplete layer or even absent. Intriguingly, tumor nests show a lamellar pattern of positivity for actin and calponin, which probably is secondary to the staining of myofibroblasts in the peritumoral stroma.53 Morphologically, LG-ASC is very reminiscent of SyT but differs from it because of the nuclear atypia, mitotic activity, stromal desmoplasia, and associated inflammatory infiltrate (Fig. 12). The relationship between these 2 entities is debated. Using immunofluorescence to highlight the distribution of luminal and basal cytokeratins and squamous and myoepithelial markers in LG-ASC and SyT, Boecker et al demonstrated substantial overlap between these tumors and concluded that both may derive from the same progenitor cells in the nipple ducts.54
 FIGURE 12:
FIGURE 12: Low-grade adenosquamous carcinoma may arise in association with nipple adenoma (A, black circle, ×20, hematoxylin and eosin); tubules and comma-shaped nests of glandular and squamous cells display atypia and invade the nipple-areolar complex with associated stromal desmoplasia (B, ×200, hematoxylin and eosin).
Treatment and follow-upSyT is usually completely excised and does not require adjuvant treatment. Recurrence has been reported.
In contrast, LG-ASC has been traditionally managed as an invasive carcinoma, which involves mastectomy or wide excision with adjuvant radiotherapy. Given that LG-ASC is triple-negative carcinoma, adjuvant chemotherapy has also been administered. However, contemporary studies with long-term follow-up found that local recurrence of this tumor is very rare, axillary lymph node involvement is exceedingly uncommon, and none of the patients with LG-ASC developed distant metastases. Although the treatment of the patients in the recent series was not uniform, these findings consider the possibility that LG-ASC may be a locally aggressive neoplasm but raise questions about its malignant potential.55,56
PAGET DISEASE OF THE BREAST Clinical FeaturesIn 1874 Sir James Paget, a British surgeon and pathologist, observed that in some female patients, an erosion/ulcer of the nipple associated with purulent exudate and pain or itching had preceded the development of an ipsilateral “scirrhous” tumor of the breast in the following 1 to 2 years. Paget disease of the breast, also known as mammary Paget disease (MPD), is indeed most common in women but can also occur in men.57 Nowadays, MPD accounts for 1% to 4% of all breast cancers.58 Analysis of 1973–2002 SEER data showed that the age-adjusted incidence rate of MPD in selected states in the United States peaked in 1985 (1.5 per 100,000-woman years) and has decreased yearly thereafter, with a 45% decrease between 1988 and 2002, likely secondary to the implementation of breast cancer screening.59 MPD can occur at any age but is more common in older patients.60 It can arise in the setting of ipsilateral invasive carcinoma or DCIS or occur in the absence of either. Of 1704 women with MPD registered in the 1988–2002 SEER database, 50.4% had ipsilateral invasive carcinoma, 36.3% had ipsilateral DCIS, and 13.3% had MPD alone. In the 1988–2002 time-period, the mean age of patients with MPD was 62.6 years (95% CI, 61.9–63.3 y), but patients with only MPD were significantly older (mean 66.2 y, 95% CI, 64.4–68.0 y) than patients with MPD and DCIS (mean 63.8 y, 95% CI, 62.6–64.9 y) or MPD and invasive carcinoma (mean 60.8 y, 95% CI, 59.7–61.8 y).59 Similarly, in a retrospective analysis of 114 patients with MPD treated at a major European Center, the median age was 54 years, and MPD was associated with ipsilateral invasive carcinoma or DCIS in the majority of cases.61
Clinically MPD presents as a crusty, red, itchy plaque on the nipple with or without the involvement of the areola, commonly accompanied by a bloody exudate, often improperly described as “nipple discharge” (Fig. 13). The diameter of the lesion can range from 3 mm to 15 cm.62 The size of MPD may correlate with the duration of symptoms, which can reach a few years in the absence of an underlying carcinoma. Sometimes the nipple may appear inverted. MPD usually is unilateral, but bilateral lesions have been reported.63 Occasionally, MPD may present as a large, irregularly pigmented lesion and mimic melanoma.64 Imaging studies rarely detect MPD not associated with ipsilateral invasive carcinoma or DCIS. On mammography, MPD may appear as skin thickening and/or nipple retraction; however, it can be undetectable in about 50% of cases.65 In a series of 34 women with biopsy-proven diagnoses of MPD who underwent a mastectomy, 32 (94%) had an ipsilateral carcinoma (7 invasive, 25 DCIS). Preoperatively, all 34 patients had a mammogram, and 13 had an MRI exam. Mammography had identified only 11 carcinomas, while MRI detected 7. In particular, MRI detected mammographically-occult disease in 4 of 8 patients. Accordingly, the current NCCN guidelines suggest MRI examination in the setting of MPD with negative mammography and ultrasound studies.66 In the setting of clinical suspicion of MPD with no imaging evidence of underlying disease, it is recommended to obtain a full-thickness skin biopsy of the involved nipple-areolar lesion, whereas if mammographic, ultrasound, or MRI examination detects a suspicious area in the breast, core biopsy of breast lesion and full-thickness skin biopsy of the involved NAC should be obtained to rule out multifocal disease, which would require a mastectomy.
 FIGURE 13:
FIGURE 13: Mammary Paget disease presenting as a large erosion of the nipple.
PathogenesisTwo pathogenetic theories are proposed for MPD. According to the Epidermotropic theory, DCIS cells migrate along the ducts towards the nipple orifices and colonize the epidermis of the nipple and areola.67 In particular, HER2/neu overexpressing malignant epithelial cells may be attracted into the epidermis by heregulin-alpha, a chemotactic factor released by keratinocytes.68 This hypothesis may explain the observation that MPD cells overexpress the HER2/neu protein in the majority of cases. Another theory involves the malignant transformation of stem cells or glandular cells in the epidermis, which is often invoked to explain MPD occurring without an underlying carcinoma. According to this hypothesis, Paget cells may originate from Toker cells, described below.69
HistopathologyMPD is an intraepidermal neoplastic process. The tumor cells are more evident in the basal layer of the epidermis, where they tend to be more numerous and form larger clusters, but smaller clusters or single cells are present throughout the thickness of the epidermis (so-called “pagetoid spread”). The neoplastic cells are substantially larger than the adjacent keratinocytes and have relatively abundant pale or eosinophilic cytoplasm. The nuclei are enlarged, hyperchromatic, with vesicular chromatin and prominent nucleoli (Fig. 14). Mitoses are often present, and some may be atypical. The epidermis involved by MPD may be acanthotic with hyper-parakeratosis, eroded, or ulcerated. Unusual morphologic features of MPD include:
Comments (0)