Design, sample, and procedure
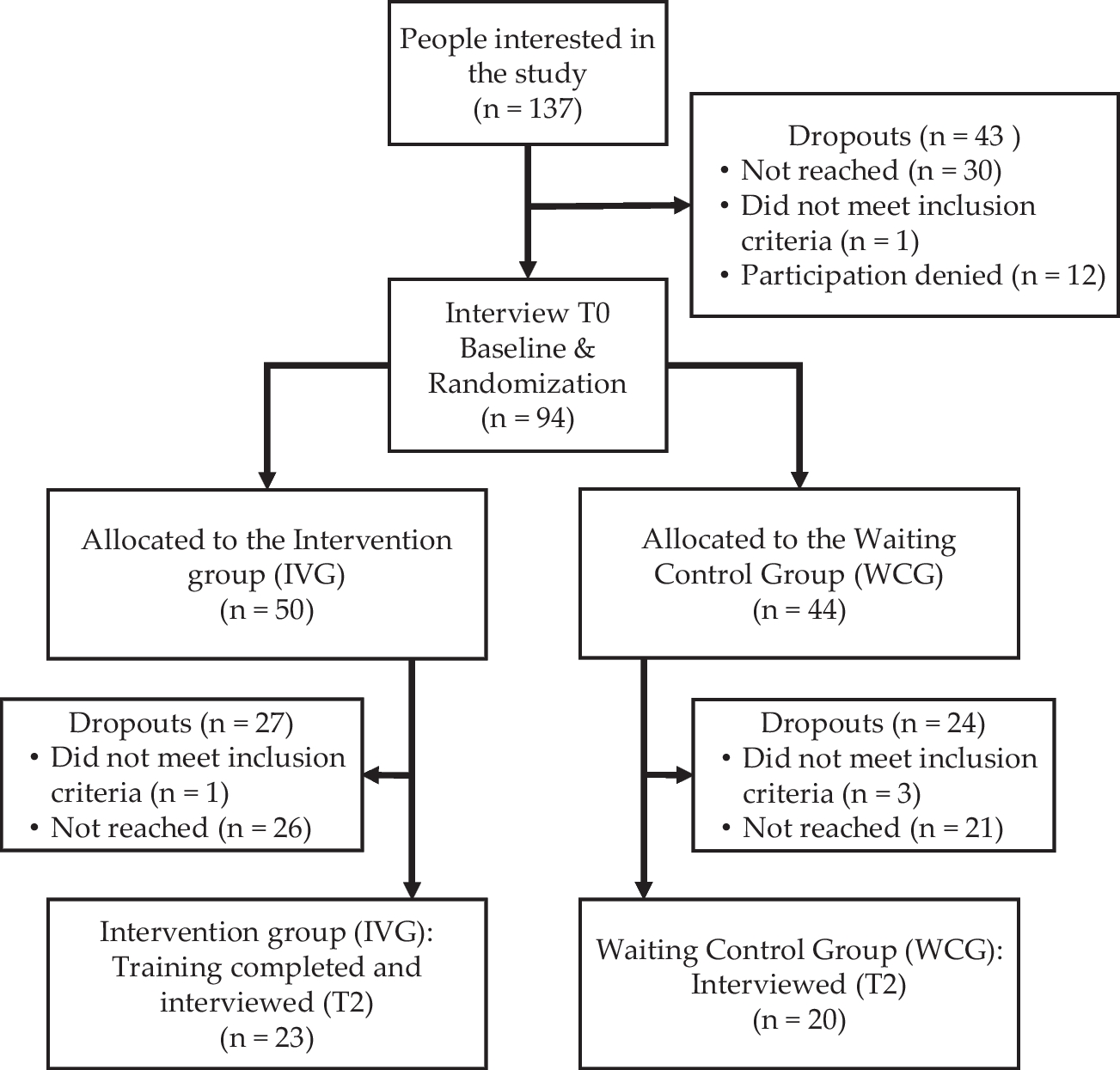
This cross-sectional study is a secondary data analysis from a larger study. The data from this study were drawn from the ADJUST study on risk factors, stressors, and mental health during the COVID-19 pandemic (Lotzin et al. 2020). N = 2245 German participants from the general population were included. Inclusion criteria were (1) being at least 18 years old, (2) ability to understand the German language, (3) written informed consent to participate in the study. Data collection took place from June until September 2020 in Germany using an online survey. The study was actively promoted using different recruitment strategies (e.g., promotion via social media platforms, organizations, leisure and interest groups).
MeasuresDepressive symptoms
Depressive symptoms were measured using the Patient Health Questionnaire (PHQ-9; Kroenke et al. 2001). Participants rated on nine 4-point scaled items (0 = ‘not at all’ to 3 = ‘nearly every day’) how often they have experienced depressive symptoms (e.g., loss of interest, fatigue, negative thoughts) during the last two weeks. Items can be summarized to a total score, cut-off categories indicate mild (5 to 9), moderate (10 to 14), moderately severe (15 to 19) or severe (≥20) depression. A cut-off score of 10 indicates probable depression (Manea et al. 2012). The PHQ-9 is a well-established instrument to screen for depression. Previous studies found high reliability, as well as criterion and construct validity for the PHQ-9 (Levis et al. 2019; Sun et al. 2020).
Living alone
To determine whether people lived alone or not, the participants were asked ‘Do you currently live together with other people?’ (0 = ‘no’, 1= ‘yes’). For the following analyses, answers were coded in reverse (0 = ‘yes’, 1 = ‘no’).
Social support
We assessed two aspects of social support, emotional and instrumental support. The Brief COPE (Coping Orientation to Problems Experienced; Carver 1997) assesses the subscales emotional and instrumental social support on 4-point-Likert scales (0 = ‘I have not been doing this at all’ to 3 = ‘I’ve been doing this a lot’) with two items each, which can be summarized in a total score. The Brief COPE is an established instrument and has been validated in various clinical and non-clinical populations (e.g., Muller and Spitz 2003).
Control variables
To control for confounding variables, we included those that have been found to correlate with depressive symptoms (e.g., Fitzpatrick et al. 2020). We controlled for age, gender (1 = ‘male’, 2 = ‘female’, 3 = ‘other’), highest education on a 6-point scaled item (1 = ‘Less than 6 years of schooling’ to 6 = ‘Doctorate’; for the analyses, categories 1 and 2, as well as categories 5 and 6 were recoded to one category), and monthly household income, also rated on a 6-point scaled item (1 = ‘Less than €500’ to 6 = ‘€5000 or more’; for the analyses, categories 3 and 4, as well as categories 5 and 6 were recoded to one category).
Statistical analyses
Before conducting the main analysis, we tested the dimensional structure of the included constructs with confirmatory factor analysis (CFA) to identify the appropriate measurement model. We then used structural equation modelling (SEM) for the main analysis. To determine the best fitting measurement model of assessing emotional and instrumental support, the following fit-indices were used: Chi-Square (χ2; p > .05), Comparative-Fit-Index (CFI; ≥ .95), Tucker-Lewis Index (TLI; ≥ .95), Root Mean Square Error of Approximation (RMSEA; ≤ .06), and Standardized Root Mean Residual (SRMR; < .008) based on the criteria of Hu and Bentler (1999).
Three different CFA models were fitted and compared: In measurement model 1 (Online Resource 1), social support was estimated as a first-order, one-factor model, where all four items loaded directly onto the latent factor social support. In measurement model 2 (Online Resource 2), social support was estimated as a two-factor, second-order model that consisted of a factor called emotional support and a factor called instrumental support, that loaded onto a second-order factor called social support. In measurement model 3 (Online Resource 3), social support was estimated as a two-factor model comprised of emotional support and instrumental support. The best fitting measurement model was then selected for hypotheses testing.
By means of a path model, the directional relationships between the factors were estimated. To test the first hypothesis (H1), which postulates a direct relationship between living alone and depressive symptoms, the latent variable depressive symptoms was regressed on the manifest variable living alone. To test whether the relationship between living alone and depressive symptoms is moderated by social support (H2), a moderation model additionally including the latent moderator variables emotional and instrumental support was estimated. The maximum likelihood (ML) parameter estimation was used for the measurement and structural models. All analyses were conducted with MPlus (Version 8.8) for macOS.


留言 (0)