In this study we find that compensation claims are rare after shoulder arthroscopy. Only 216 claims out of 69,097 shoulder arthroscopies were filed, accounting for 0.3% of all operations. This is lower compared to other elective orthopedic procedures such as hip- and knee arthroplasty (1.9% and 0.9% respectively) [6, 7]. However, these procedures are open surgeries with high expectations and wider complications which may partially explain the difference found in our material. In a retrospective study from Finland, 8 901 compensation claims after various surgical procedures were analyzed [11]. Similar to our findings, they reported an overall claim rate of 6 per 1000 procedures (0.6%) but denoted that “different surgical procedures exhibit varying claims”. Similar to other studies, we found an acceptance rate of compensation claims at nearly 40% [4, 5, 7, 11].
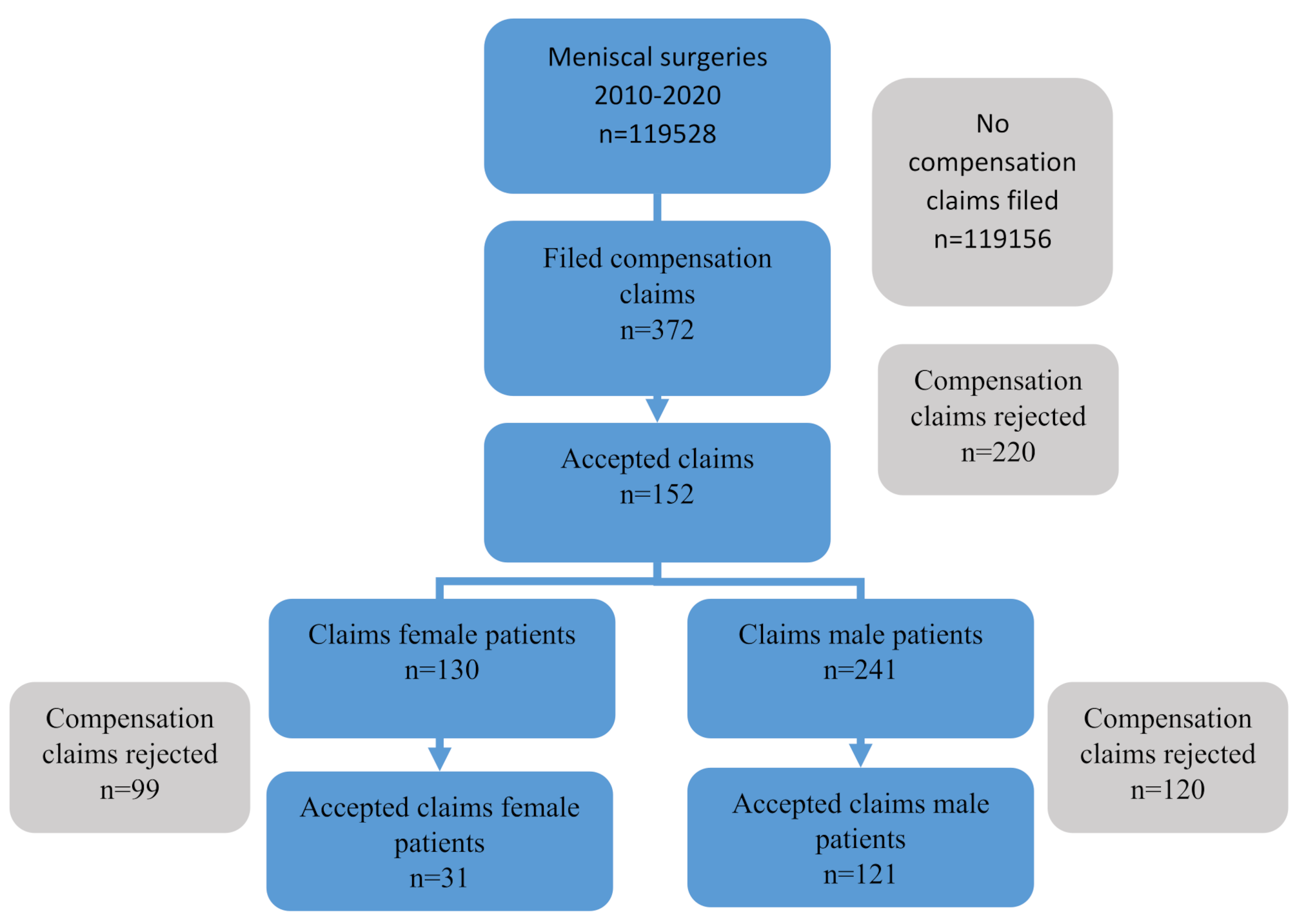
Our data demonstrates that more men than women file a complaint. This is somewhat different to previous findings, where women more often file a compensation claim [6, 7]. Some diagnosis and procedures are more common for men, while others are more common for women. This slightly different gender imbalance may explain why more men than women filed a compensation claim after shoulder arthroscopy compared to hip replacement surgery.
The main reason for an accepted compensation claim was infection (37.8%). This is consistent with previous studies on compensation claims following orthopedic surgery [5,6,7]. According to regulatory laws governing the Norwegian System of Patient Injury Compensation system, patient claims due to infection are accepted as long as the patient does not have an underlying disorder predisposing for infection. These claims are still evaluated for patient injury, but acceptance is granted independently of this investigation if no predisposing factors are identified.
No indication for surgery was the second most common reason for accepted compensation claims (15.9%). This demonstrates the importance of accuracy in diagnosis and indication for surgery and is a reminder that non-operative treatment often is a valid solution. There is an increased focus on low-value care, referring to the use of health care service for which harms or costs outshine the therapeutic benefits [12, 13]. The Choosing wisely campaign, originating from the United States, have become an international strategy to reduce wasteful healthcare [14]. In arthroscopic shoulder surgery, several studies have demonstrated that less equals more [15, 16]. Schrøder et al. showed that neither labral repair nor biceps tenodesis for superior labrum anterior posterior lesion of the shoulder is superior to sham surgery [15]. Our study indicates that experts at the Norwegian System of Patient Injury Compensation have caught on to the change in indication for some arthroscopic procedures, and that publications such as this one may help direct attention to low value care in orthopaedics.
The Norwegian System of Patient Injury Compensation experts concluded that ten patients had suffered a patient injury due to “wrong surgical technique”. This included insufficient bone removal in shoulder impingement procedures, loose/misplaced anchors after rotator cuff surgery and insufficient surgical capsulotomy before frozen shoulder mobilization. No common denominator was found among these patients, but is should be mentioned that only one Norwegian System of Patient Injury Compensation expert assesses a compensation claim making the assessment susceptible to subjectivity. It is important to point out that the Norwegian System of Patient Injury Compensation experts had the luxury of hindsight when reviewing the claims. A clearer guideline for the experts or multiple reviewers is desirable.
Pain was a common reason for filing a complaint, as 95 patients (43%) filed a complaint due to postoperative pain. However, pain is not a common cause for accepted claims as only 9 of 95 patients (9.5%) received compensation due to persistent postoperative pain. This finding is consistent with other studies [5, 8].
One patient suffered a cerebral stroke after an elective subacromial decompression. Acceptance was granted due to both faulty indication of the surgery and the consequences for the patient which were described as disproportional to the potential benefits of the surgery.
One patient was operated in the wrong shoulder. This occurred in 2013. Although various safe surgery checklist was implemented in Norway from 2012 to reduce and prevent treatment errors [17], this unfortunate accident demonstrates the importance of vigilance in all health care aspects.
A total of 7 patients had their compensation claims accepted due to inadequate diagnostics. This is a reminder of the importance of taking the time and performing the necessary tests required to arrive at the correct diagnosis before committing to a treatment strategy, especially if this involves surgery. The time interval from diagnosis to surgical treatment was considered too long for 5 patients (6.1%). The reparability of a rotator cuff rupture decreases in time. Within months, fatty infiltration and atrophy limit the mobility of the rotator cuff causing an eventual irreversible retraction of the tendon [18]. Particularly in the presence of a traumatic rupture, time is of the essence.
In a study involving malpractice claims against shoulder surgeons, Lynch et al. identified only 45 malpractice claims over a 28-year period [8]. This study included arthroscopic and open surgery and reported that rotator cuff repairs had the greatest total number of litigations, whereas manipulation under anaesthesia had the highest probability to be litigated. This is somewhat different to our findings. We found NBA11 (shoulder arthroscopy) to be the most likely procedure to lead to a patient injury and an accepted claim (p < 0,05). This procedure code is often used as a primary code in more complex arthroscopies (i.e. shoulder stabilization, capsulotomies) as well as minor surgeries (i.e. diagnostic procedures, removal of corpora libra). The surgical diversity differs more within this group than in the other groups. This might at least in part explain why this group has more acceptances than the other groups.
A puzzling finding in our study is that there is a complex relationship between hospital geography and accepted compensation claims following shoulder arthroscopy. We found a significant increased odds ratio for an accepted claim per procedure in both the Northern and the South-Eastern regional Health Trusts compared to the other regional Health Trusts and the private institutions. The Northern regional Health Trust is the smallest regional Health Trust in Norway both in terms of catchment population and the number of shoulder arthroscopies, while the South-Eastern regional Health Trust is the largest and performed most arthroscopies. It is not unexpected that the regional Health Trust with the fewest surgeries had a higher risk for accepted compensation claims, as this is consistent with previous findings that lower volume is proportional to accepted compensation claims [5, 7]. The fact that we found an increased risk of accepted compensation claim also in the highest volume regional Health Trust is somewhat surprising. However, two of Norway’s most high-profile shoulder centres that treat complex and difficult shoulder injuries are located in this region, which may explain this finding.
There are some limitations to our study. We lacked clinical information on sex and age from NPR, and the diagnosis codes are broad and cover many different procedures, which makes it difficult to find subgroups of interventions that might have a particularly high risk of patient injury. We have only included surgical treatment options for common shoulder disorders and excluded non-surgically treated patients. Our data is from a single country, with a compensation claim system that differs from other countries, which may affect the generalizability of our study. However, identifying areas of improvement in health care should be of global interest. It is likely that patient injuries have occurred during the study period that was not reported to the Norwegian System of Patient Injury Compensation. The threshold for filing a complaint is highly individual. It is likely that a study on compensation claims is underestimating the prevalence of patient injury since not all patient injuries are reported to the Norwegian System of Patient Injury Compensation.






Comments (0)