Although the onset of SS is mainly in middle-age, epidemiological studies have shown that the disease can occur at any age and has been diagnosed in patients aged 2 [18] to 97 years [19]. The data available so far indicates that SS is a very rare disease in children [20]. The number of studies and reported cases of pediatric-onset SS are very limited compared to that of adult-onset SS. The 54 patients included in this cohort were around 10 years of age at the time of diagnosis, which was generally consistent with the findings of other pediatric cohort studies, and in terms of gender composition, our cohort had more girls and the female to male ratio in our cohort was 49:5 (9.8:1), when compared to the ratio of around 6:1 reported in other cohorts [5,6,7,8, 14,15,16,17].
In addition to dryness symptoms, patients with SS can have extensive extraglandular multiorgan and multisystem involvement, and in some cases, the organ damage can precede the dryness symptoms. Skin involvement is more common and includes purpura-like rash, erythema nodosum, and Raynaud’s phenomenon [21]. In our cohort, the skin involvement was also common being present in 46.3%. Involvement of the skeletal muscular system may be present with joint swelling and pain, arthritis, myalgia [21]. In our cohort, the skeletal muscular system involvement was 11.1%. Renal involvement mainly involves the distal renal tubules, and renal tubular acidosis is more common in pediatric SS patients [21]. In our cohort, renal tubular acidosis was 9.3%. In the hematological system, anemia, leukopenia, thrombocytopenia, and hyperimmunoglobulinemia is one of the features of SS [19]. In our cohort, cytopenias was 29.6%, and hyperimmunoglobulinemia was 63.0%. The incidence of lymphoma is significantly higher in patients with SS compared to the normal population. But lymphoma was not found in our cohort. The respiratory tract is most dominated by interstitial lung disease [21]. Involvement of exocrine glands in the mucosal layer of the digestive tract may result in atrophic gastritis, gastroesophageal reflux, dyspepsia [21]. Neurological involvement is less frequent and mostly manifests as impairment of peripheral nerve functions, and it can also coexist with neuromyelitis optica spectrum disorders [21]. In our cohort, the neurological involvement was 5.6%.
In this cohort, the pediatric dry symptoms were uncommon, and few patients presented with parotid enlargement, but more patients visited the hospital with extra-glandular symptoms manifesting mostly as fever, joint symptoms, lymph node lesions, and rare conditions such as renal tubular acidosis and pulmonary hypertension. This could be due to the fact that the build-up of exocrine gland dysfunction takes time, and it did not progress to visible symptoms in pediatric patients due to their young age. In contrast to our findings, Ramos-Casals et al. [7] reported a higher proportion of dryness symptoms in their cohort (n = 158), with 79.7% reporting dry mouth and 70.3% reporting dry eyes, and this may be related to the different inclusion criteria of cases in the cohorts. Inclusion in their cohort was based on the 2002 AECG and/or 2016 ACR/ EULAR classification criteria, where the premise of dry eye and dry mouth symptoms were the basis for inclusion, and hence, the difference in the incidence of subjective symptoms of dry mouth and dry eyes was more pronounced and may be due to case selection bias [7]. However, in Asian cohort studies, symptoms of dryness were generally lower [15,16,17], suggesting that there may also be racial differences. This could similarly explain the large variation in the proportion of subjective symptoms of dry mouth and dry eyes (16%–52.2%) reported in several other pediatric cohorts [5,6,7, 14,15,16,17]
Cimaz R [5] and Stiller M [6] reported recurrent parotid swelling was the most common clinical feature being present in 57.5% and 47.8%, respectively. But in our cohort, it was only 3.7%. The reason for the difference is not clear, it may be related to the different ethnic composition of the cohort.
The examination of the exocrine glands consists mainly of the salivary gland and lacrimal gland examinations [22]. Salivary secretion function can be evaluated by measuring salivary flow rate, including post-stimulation flow rate (e.g., chewing gum test, Saxon test) or resting/non-stimulation flow rate. Parotid gland imaging or 99mTcO4-nuclein imaging are also commonly used for detection. Salivary gland biopsy, which has low acceptance in pediatric patients, can visualize glandular involvement, and focal infiltration of lymphoid cells can be seen around the glandular ducts in patients with SS. Salivary gland ultrasonography and magnetic resonance imaging are also used [8]. In our center, nuclide imaging is often used to evaluate the secretory and excretory functions of the salivary gland and ultrasonography is utilized to observe the parenchymal damage of the gland. In this cohort, the positive rate was 70.4% for nuclide imaging and 55.6% for ultrasonography. Although the clinical manifestations of glandular enlargement were few, the ratio of glandular function and parenchymal damage was actually high, which suggested that there was mostly objective evidence in the pediatric salivary gland examination, but the external manifestations were absent. The means commonly used for lacrimal gland examination include Schirmer’s test, tear break-up time, and corneal and conjunctival staining score. The Schirmer I test, a method that does not use surface anesthesia, is used to determine the secretory function of the primary lacrimal gland and is generally well tolerated by children. The positive rate for Schirmer I test was not high in patients in our cohort, which is consistent with the low incidence of subjective dry eye symptoms of patients, and our results indicated that in pediatric SS, the involvement of salivary glands was greater than that of lacrimal glands.
In terms of laboratory investigations, the positive rate of Anti-Ro/SSA antibodies in our cohort (94.4%) was slightly higher than what others reported (73.6%–82.7%), and the positive rates of other indicators such as Anti-La/SSB antibodies, ANA, RF, and IgG were not significantly different [5,6,7,8, 14,15,16,17], and the variation in these indicators was consistent with the features of SS. The presence of autoantibodies is of considerable value in the diagnosis of SS, and studies have shown that serologic evidence is present approximately 18–20 years before the diagnosis is confirmed [23], therefore, it is also highly suggestive in the diagnosis of pediatric SS.
Pediatric SS is undeniably a systemic disease (90% of cases have systemic activity at the time of diagnosis, defined as ESSDAI score ≥ 1). Age at diagnosis is a critical deciding factor for systemic disease expression in primary SS, and an international cohort study showed that the highest ESSDAI score was in the 18–35 years group [19]. The ESSDAI score of our cohort was 4.91 ± 2.71, which is slightly lower than that reported by other cohorts [5,6,7,8, 14,15,16,17]. The top five sites in this cohort were serologic changes, systemic symptoms, glandular lesions, skin lesions, and lymph node lesions; The top five areas reported by Ramos-Casals et al. [7] (n = 158) were serologic changes, glandular lesions, hematologic lesions, lymph node lesions, and arthropathy; the top five areas reported by Legger et al. [14] (n = 23) were glandular lesions, serological changes, systemic symptoms, arthropathy, and lymph node lesions; those reported by Kobayashi et al. [15] (n = 25) were serological changes, systemic symptoms, glandular lesions, arthropathy, and skin lesions; and those reported by Cimaz et al. [5] (n = 40) were glandular lesions, arthropathy, systemic symptoms, renal lesions, and lymph node lesions, and those reported by Gong Y et al. [16] (n = 39) were serologic changes, skin lesions, systemic symptoms, hematologic lesions, and lymph node lesions, and there was no significant difference in the domains that were frequently involved [5,6,7,8, 14,15,16].
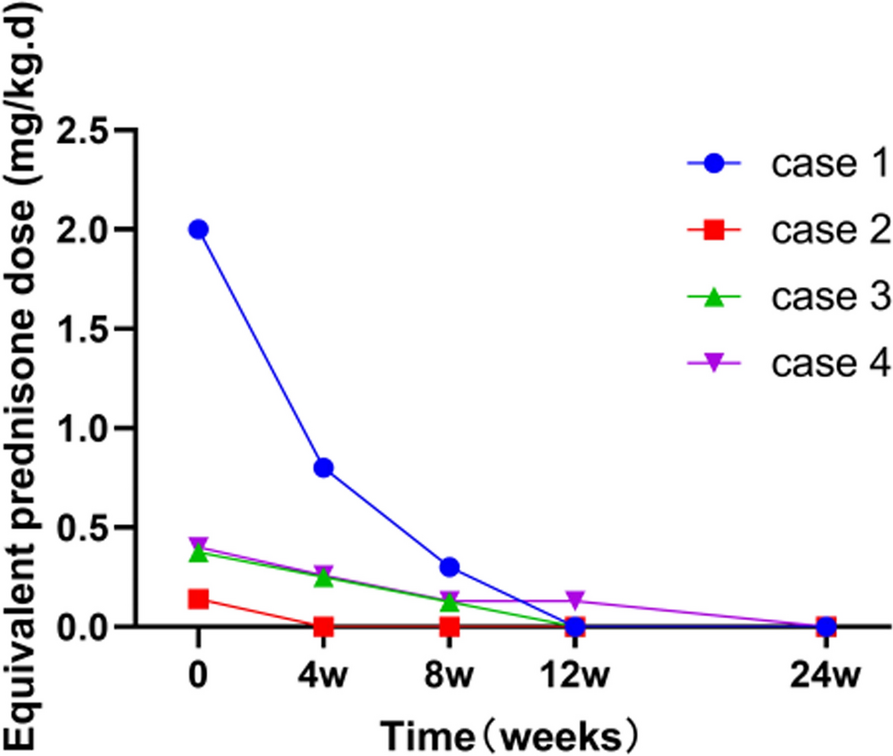
There is no specific treatment for SS that can reverse impaired glandular function and cure the disease, and patients are usually treated symptomatically to improve their quality of life. The vast majority of patients in our cohort had been treated with glucocorticoid and hydroxychloroquine, which were mainly administered to treat the extra-glandular symptoms, control the patient’s systemic inflammatory response, and protect the gland from further damage. Immunosuppressive agents were used in a low proportion, while MMF was commonly used. The treatment was also basically consistent with the reports of pediatric SS [8].
Starting with the Bloch criteria in 1965 [24], there are more than a dozen diagnostic and classification criteria for SS to date, but all are based on data from adult cohorts and have not been validated in pediatric cohorts. In adult SS, the 2002 AECG and/or 2016 ACR/ EULAR classification criteria are often used, but in pediatric SS, the compliance of these two criteria in clinical use is not high [8, 25]. 1999 proposed juvenile pSS criteria [26] have not been widely verified, and no formal diagnosis and classification criteria for children’s SS have been proposed yet. Our pSS patients showed only 8.8%, 14.7% and 52.9% met AECG criteria and ACR/EULAR criteria and proposed juvenile pSS criteria, respectively. New classification criteria was proposed in Japan in 2015 with the aim to identify pediatric SS cases at an early stage [27]. The criteria were designed to have separate scores for serology (S-score) and glandular involvement (G-score), and the score items took into account the special features of children, such as the difficulty of performing labial gland biopsy in pediatric patients, which was assigned fewer points, and further emphasized the importance of autoantibodies for the diagnosis of SS, and dryness symptoms were only one of the manifestations that needed clinical attention. The classification categories include definite SS, probable SS, possible SS, needs follow-up, and possibly non-SS [11]. An official diagnostic guideline for these criteria was published in 2018 [11] and the same set of criteria is used for primary SS and secondary SS. This study did not adopt the current international standards [9, 10], but based on the opinion of Chinese pediatric rheumatology experts, focusing on substantive evidence of exocrine glands involvement rather than sicca symptoms, combined with serological characteristics, aimed at identifying the clinical characteristics of this group disease in early stage for early diagnosis and treatment. Our pediatric cohort showed good compliance with the Japanese guideline, with 9.3% identified as Definite SS, 61.8% as Probable SS, and 26.5% as Possible SS. Taking into account the above discussion on the sicca symptoms, the incidence in Asian cohort is more similar (Table 4) [15,16,17], suggesting that the reason why the Japanese guideline is more applicable to our cohort may also be related to race.
The characteristics of SS such as photosensitive rash, arthritis, positive autoantibodies may also be observed in the other autoimmune diseases (including rheumatic arthritis and systemic lupus erythematosus (SLE). 8.3% -19.0% of SLE patients accompanied with SS, even some cases develop SLE several years after being diagnosed with SS [28,29,30]. Researches on adults found that, SLE with SS appears to constitute a subgroup of patients with distinct clinical, serologic, pathologic, and immunogenetic features, in whom SS is expressed as an overlapping entity and is largely similar to primary SS [30]. From this cohort study, we also found that there was no significant difference in clinical manifestations between primary and secondary SS, and sicca symptoms in children were uncommon, which made the diagnosie of SS face great challenge in distinguishing primary and secondary. Fever is atypical symptom, and in the absence of infections and tumors, which only indicates systemic inflammation and has no specificity for diagnosis. In addition, in our subgroup analysis, there were no significant differences between primary and secondary SS with regard to epidemiological features, clinical manifestations, auxiliary investigations, disease activity scores, and treatment, except for individual aspects, which suggested that these patients had a common pathogenesis that may be related to the similar autoantibody spectrum. However, from another perspective, since primary and secondary SS have such similarities in many clinical aspects, it is not so urgent to distinguish them early. Only closely follow-up, observation, and treatment are needed.
As is common among rheumatic diseases, the lack of an objective standard for diagnosis of SS in children requires the use of expert opinion as our gold standard for inclusion. This also leads to the evaluation of children being performed in a non-standardized fashion. Children with mild dryness may not seek medical attention resulting in a lower perceived prevalence of dryness and possibly the disease. And this was a retrospective clinical study, and the limitation is that the small sample size may have led to some bias in our findings. A larger sample size is needed in the future for more in-depth enquiry.
In conclusion, based on the analysis of clinical cases of pediatric SS in this study, we found that the incidence of the subjective symptom dry mouth and dry eyes was low and that children were more likely to develop various clinical manifestations of multisystem involvement. The findings of this study are similar to other pediatric study cohorts in terms of epidemiology, auxiliary investigation results, disease activity scores, and treatment. The Japanese Diagnostic Guidelines for Pediatric Sjögren’s Syndrome (2018) may be more suitable for the diagnosis of pediatric Sjögren’s syndrome in china.







留言 (0)