IL-1 plays an important role in inflammation and immunological responses, binding to the IL-1 receptor and activating a wide variety of inflammatory mechanisms. IL-1 receptor is also regulated by a natural IL-1 receptor antagonist (IL-1RA) that binds to IL-1 receptor binding sites and competes with IL-1. Being a recombinant IL-1 receptor antagonist, anakinra binds to the receptor and, therefore, reduces the inflammatory response [4]. Its metabolism in the body is not fully understood. It is known that the main route of elimination is the kidney [5]. Although the non-renal clearance pathway has not been described, as a protein-based therapy it may undergo endogenous proteolysis [5]. Similarly, the mechanism by which anakinra causes liver injury is also unknown. Previous research has related polymorphisms in IL-1 receptor antagonist and IL-1β to antiretroviral hepatoxicity [6]. However, further studies are needed to better understand the direct link between anakinra and liver injury.
Anakinra associated hepatotoxicity is an uncommon side-effect previously observed in the adult rheumatic patient population, especially in individuals with Still’s disease, and several cases of asymptomatic hepatic enzyme elevation have been described [7].
The cases presented are representative of children with rheumatic disease who developed acute hepatitis undergoing anakinra. Clinical presentation was a diagnostic challenge, as diverse infectious and malignant aetiologies had to be excluded. Bone marrow biopsies were not generally suggestive of hemophagocytosis, with the diagnosis of MAS and SHS anchored in clinical and laboratorial data. No apparent triggers were identified in these patients. After exclusion of other aetiologies, anakinra-induced hepatic injury was assumed, resolving after drug suspension. Since they responded to other treatments, no patients were rechallenged with the drug after discontinuation.
Liver enzymes may be elevated during the first stages of sJIA, even in the absence of MAS, although the degree of elevation is generally mild [8, 9]. Moreover, hepatic dysfunction in KD is frequently manifested as transaminitis, despite great individual heterogeneity [10]. Frequently hepatic dysfunction represents the main organ involvement in MAS, presenting as an extreme elevation of liver enzymes and lactate dehydrogenase, besides the more traditional clinical finding of hepatosplenomegaly [11]. Disease-related hepatic dysfunction in these patients is generally accompanied by inflammatory marker elevations, with rapid response to treatment, making anakinra-related hepatotoxicity an exclusion diagnosis [2]. In this case series, all patients had transaminitis when their inflammatory response had improved, thus facilitating differential diagnosis.
Previous studies have reported anakinra associated hepatotoxicity in pediatric rheumatic diseases. Canna S. et al [12] described three cases of anakinra induced acute hepatitis in children treated with anakinra for refractory or severe disease. Only two patients developed suggestive symptoms of abdominal pain and jaundice, with a delay until diagnosis ranging from 44 to 250 days. Hyperbilirubinemia was an important laboratorial feature in two patients and cholestasis was uncommon, with significant AST elevations > 1000 UI/mL in all patients. All laboratorial abnormalities rapidly resolved with therapeutic suspension.
Phadke O. et al [13] described a case series of 3 patients with sJIA/MAS who underwent IL-1 A or IL-6 A treatment, with two patients developing biopsy proven hepatitis less than a month into follow-up of anakinra. There was a significant dissociation between clinical symptoms and inflammatory markers and elevation of liver enzymes, sustaining a drug induced mechanism, as in the cases hereby presented. All situations were reverted with pharmacological discontinuation.
Murray G.M. et al [14] reported a case of a 13-year-old boy with sJIA who was treated with pulsed intravenous MPDN and anakinra 3 mg/kg afterwards with prompt clinical improvement and laboratorial value normalization, with IL-1RA discontinuation after 10 days of treatment. Posteriorly, MAS led to reintroduction of anakinra, with severe elevation of hepatic enzymes 1 month later, with suspension of therapy leading to steadfast cessation of liver injury.
In a recent post authorization safety study using the Pharmachild registry including 306 patients with sJIA, Giancane G et al [15] described adverse events related with anakinra (monotherapy or in association with other glucocorticoids or DMARDs), with description of only 6 cases of increased liver enzymes and hepatitis.
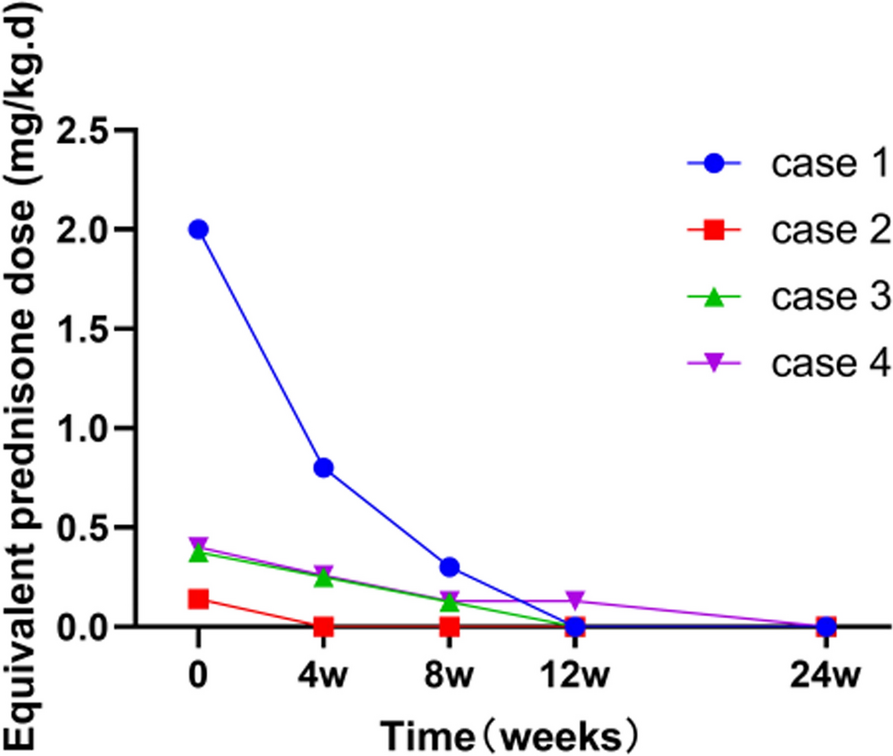
Figure 1 A, B and C show the evolution of liver enzymes after introduction of anakinra in the three cases presented here. The results show an earlier adverse liver injury compared to cases previously described in literature.
Only one patient had hepatic involvement by the rheumatic disease at diagnosis (Case 3), and only one patient had symptoms and objective findings compatible with acute hepatitis (Case 1). A ratio ALT:AST > 1 was observed in all patients, associated with mild to no degree of cholestasis, compatible with a hepatocellular injury pattern, frequently described in acute toxic hepatitis. There was not a clear relationship between dose and degree of liver enzyme elevation, pointing to the fact that anakinra associated hepatotoxicity follows an idiosyncratic pattern in pediatric patients.
Elevation of liver enzymes was observed in the first month of treatment for all patients, as with adult patients who were reported to have developed anakinra-associated hepatotoxicity [7], suggesting a similar pathophysiology for this adverse effect in both subsets of patients.
Liver dysfunction was not more serious in the individual with hepatic involvement by KD at presentation, nor recuperation was longer than in the other cases described. Cessation of anakinra led to rapid resolution of the adverse event in all cases, with an average time until complete resolution of laboratorial abnormalities of 20.3 (± 11.8) days. Data regarding anakinra hepatotoxicity in KD patients is lacking, with previous studies not revealing significant hepatotoxicity, or general side effects for that matter [16].
Liver biopsy may prove useful to ascertain the aetiology of acute liver dysfunction in young patients under anakinra with potential confounding factors, with previous case series describing nonspecific patterns of mixed inflammation without identifiable hemophagocytosis, vascular microthrombi, or cholestatic biliary injury in pediatric sJIA patients [13, 3]. None of the patients in this case series underwent liver biopsy due to causal association between anakinra introduction and hepatic enzyme elevation and swift normalisation of laboratorial values following drug withdrawal, after extensive differential diagnostic consideration and exclusion.







留言 (0)