
記住我
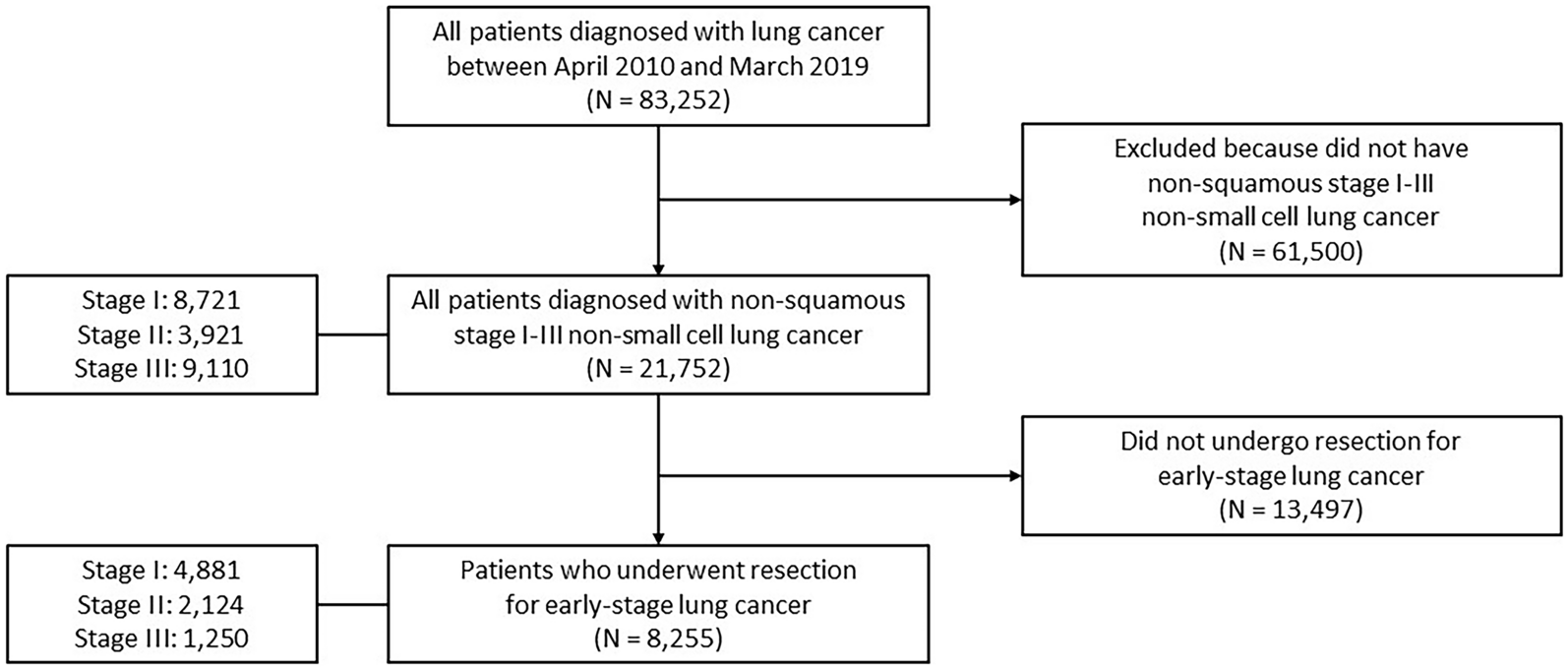


The initial literature search using search syntax identified 140 articles. Of these, 74 remained after deleting 66 duplicates. Upon title and abstract screening, 38 articles were omitted as they did not meet the inclusion criteria. After full-text analysis of the remaining 36 articles, 20 papers were excluded due to the non-availability of full text (n = 2), only published abstract (n = 1), previous cancer-directed treatment (n = 6), no survival data available for analysis (n = 5) and no data available for a primary surgical subset (n = 6). A total of 16 studies [5, 7,8,9, 31,32,33,34,35,36,37,38,39,40,41,42] were included in the qualitative synthesis. Finally, seven studies [7, 8, 31, 33, 37, 39, 41] were included for meta-analysis as T4a and T4b data were available for comparison. The data were extracted from the published Kaplan–Meier graphs of the respective articles using Webplotdigitizer.
The Rationale for Study InclusionLiao et al. [31] (2012) provided distinct datasets for infranotch T4b and T4a categories within their findings. Pillai et al. [8] have categorised T4b tumours into three distinct classes (I: lower masticatory space or infranotch; II: intermediate masticatory space or low supra-notch; and III: high-masticatory space or high supranotch) based on the extent of infiltration into the ITF, aligning with the classification outlined by Trivedi et al. [43]. In our meta-analysis, we have selectively incorporated the subset of T4b patients falling under class I from this study. Similarly, Pillai et al. and Mair et al. [33] have exclusively examined patients with low ITF and excluded those involving supranotch ITF as per the classification elucidated by Liao et al. [5] (2007). Thiagarajan et al. [37] recently conducted a comparative investigation of upfront surgery versus neo-adjuvant chemotherapy for both T4a and T4b oral cancers. Within their upfront surgery group, they have encompassed patients that underwent curative-intent surgery. Our analysis has confined our focus to the cohort of upfront surgical cases encompassing T4a and a subset of T4b. Kumar et al. [39], in their study, have included patients that underwent curative-intent surgery for T4b. Their scrutiny of T4b outcomes has been predicated on the involvement of components within the masticator space, including the masseter muscle, medial pterygoid muscle, ramus of mandible, lateral pterygoid muscle and the lower pterygoid plate. Remarkably, the components scrutinised by Kumar et al. [39] closely correspond to the constituents of low ITF, as delineated in the subcategorisation framework proposed by Liao et al. [5] (2007).
Further, Patel et al. [7] have incorporated data from the NCDB database, while Kang et al. [41] have integrated information from the Taiwanese Cancer Registry. An important note is that Patel et al. [7] study exhibits disparities in the numerical values depicted within their Forest plot. In this analysis, we have confined our consideration to values concordant with the data described within the results section and consistent with their abstract. Both Kang et al. [41] and Patel et al. [7] have encompassed patients who underwent curative-intent surgical interventions for T4a and T4b. However, neither of these studies provided distinct data for patients falling within the supranotch and infranotch T4b categories.
Quality of Included StudiesThe main characteristics of the included studies are summarised in Table 1. The qualitative data synthesis yielded 1229 surgically treated T4b patients from 16 articles, and 820 patients from 7 studies were included in the final meta-analysis. Seven studies reported the comparative surgical outcomes for T4a and T4b patients; 10,561 patients of surgically treated T4a patients were included for comparative meta-analysis. Eligible studies were either a prospective (n = 1) [8] or retrospective (n = 15) [5, 7, 9, 31,32,33,34,35,36,37,38,39,40,41,42] cohort study design, and none were randomised controlled trials. Two studies were based on the cancer registry, namely the Taiwan cancer registry (TCR) and the US National Cancer Database (NCDB). The Newcastle–Ottawa score ranged from 6 to 8 (Table 1). Based on the risk of bias assessment tool, the included studies had the highest risk of patient selection and confounding variables (Supplementary Fig. 1).
Two Year Overall Survival (T4b versus T4a)Two year OS data were extracted from 11 studies [7, 31,32,33,34,35, 37, 38, 40,41,42] for T4b disease. The 2 year OS data were extracted from five studies [7, 31, 33, 37, 41] for T4a and T4b. The pooled 2 year OS was 61.2% for T4b patients from 11 studies [7, 31,32,33,34,35, 37, 38, 40,41,42]. The pooled 2 year OS was 59.7% for T4b (n = 660) and 64.6% for T4a (n = 10,371) patients from five studies in the meta-analysis [7, 31, 33, 37, 41]. The pooled data had significant heterogeneity (Table 2). The logOR was 0.21 (−0.25, 0.67; DL, REM, CI = 95%) favouring T4a and the overall effect estimates for T4a and T4b were not statistically significant for 2 year OS (Z = 0.9, p = 0.36, CI = 95%) (Fig. 2). Normal Q–Q plot shows bimodal distribution. The publication bias (funnel plot asymmetry) was insignificant (Table 2) (Supplementary Figs. 2, 3, 4).
Table 2 Overview of meta-analysis statisticsFig. 2
Forest plot (A, B) and L'Abbé plot (C, D) for overall survival (OS); 2 year OS (A, C) and B 5 year OS (B, D)
Two Year Overall Survival (subset IN–T4b versus T4a)Two year OS data were extracted from three studies [31, 33, 37] for T4a and IN–T4b patients for the meta-analysis. The pooled 2 year OS was 59.3% for IN–T4b (n = 149) and 65.3% for T4a (n = 653) patients from three studies in the meta-analysis [31, 33, 37]. The pooled data had significant heterogeneity (Supplementary Table).The logOR was 0.28 (−0.47, 1.03; DL, REM, CI = 95%) favouring T4a and the overall effect estimates for T4a and T4b were not statistically significant for 2 year OS (Z = 0.73, p = 0.46, CI = 95%). Normal Q–Q plot shows bimodal distribution. The publication bias (funnel plot asymmetry) was significant (Supplementary Figs. 5–9).
Five Year Overall Survival (T4b versus T4a)Five year OS data were extracted from nine studies for T4b disease [5, 9, 31, 33, 35, 38, 39, 41, 42]. Five year OS data were extracted from four studies [31, 33, 39, 41] for T4a and T4b patients for the meta-analysis. The pooled 5 year OS was 46.1% for T4b patients from nine studies [5, 9, 31, 33, 35, 38, 39, 41, 42]. The pooled 5 year OS was 53.2% for T4b (n = 508) and 50.9% for T4a (n = 4393) patients from four studies [31, 33, 39, 41] in the meta-analysis. The pooled data had significant heterogeneity (Table 2). The logOR was 0.09 (−0.20, 0.38; DL, REM, CI = 95%) favouring T4a and the overall effect estimates for T4a and T4b were not statistically significant for 5 year OS (Z = 0.61, p = 0.54, CI = 95%) (Fig. 2). Normal Q–Q plot shows bimodal distribution. The publication bias (funnel plot asymmetry) was not significant (Table 2) (Supplementary Figs. 10–12).
Five Year Overall Survival (subset IN–T4b versus T4a)Five year OS data were extracted from three studies [31,
留言 (0)