
記住我









Attachment theory proposes a theoretical model that aims to explain how the development of early interpersonal relationships forms cognitive patterns that qualify an individual's perception as being worthy of care (care-seeking) and the perception of others as being reliable in providing care (caregiving).2,3 Attachment style tends to be stable through life and affects how people think, feel, and behave in close relationships all over the life span, “from the cradle to the grave”3 (p. 129). Therefore, attachment security/insecurity is perceived as a diathesis, which determines how individuals relate to each other and manage threatening situations such as an illness.22
Previous studies have shown that attachment style has an indirect effect on pain management. Patients with chronic pain and insecure attachment report higher levels of pain-related stress, anxiety, depression and catastrophizing,4,18–20,28 and lower pain self-efficacy.19 They are more likely to use emotion-focused than problem-focused coping,21 report greater pain intensity and disability,17,28,30 describe themselves and their pain with more threatening terms, and feel less capable to cope with pain.18,21 Individuals with insecure attachment also report greater usage of health care.4 Patients who met the criteria for “chronic widespread pain” were 70% more likely to report insecure attachment than the group of patients with no pain.6
On the other hand, self-compassion is a concept that is gradually taking its place as a resilience factor in patients with chronic pain, associated with greater pain acceptance, lower levels of anxiety and depression,5 as well as with adaptive coping strategies (active coping, acceptance, and positive reframing) in patients with chronic pain. The concept of self-compassion refers to an individual's capacity to contain their feelings of suffering with a sense of warmth, connection, and care.24 This involves an ability to be kind to oneself and to confront one's difficulties with understanding and as part of the human experience, as well as to keep one's emotions and thoughts in balanced awareness without overidentifying with them (ie, mindfulness). Early experiences either support or hinder the development of soothing and threat systems and influence the formation of emotional self-regulation and the ability to be compassionate.11–13
Attachment patterns and self-compassion seem likely to influence not only the emotional experience but also the means through which a person will cope with the situation.
Thus, the purpose of our study is mainly to explore the interrelationships between these related variables in patients with chronic pain to improve intervention and help patients to adopt more functional strategies to cope with chronic pain. The study's novelty is rooted in the fact that there is no research articulating these 3 variables together, and very few that studies them separately, in patients with chronic pain.
Attachment quality and self-compassion are more stable variables of an individual's psychological functioning and are not exclusive to the chronic pain context, so similar results from studies conducted in the general population are expected.16,25,26,31 Specifically, our principal hypothesis is that secure attachment will be positively correlated with global self-compassion. Regarding the coping variable, we will explore how attachment quality and self-compassion are related to coping quality.
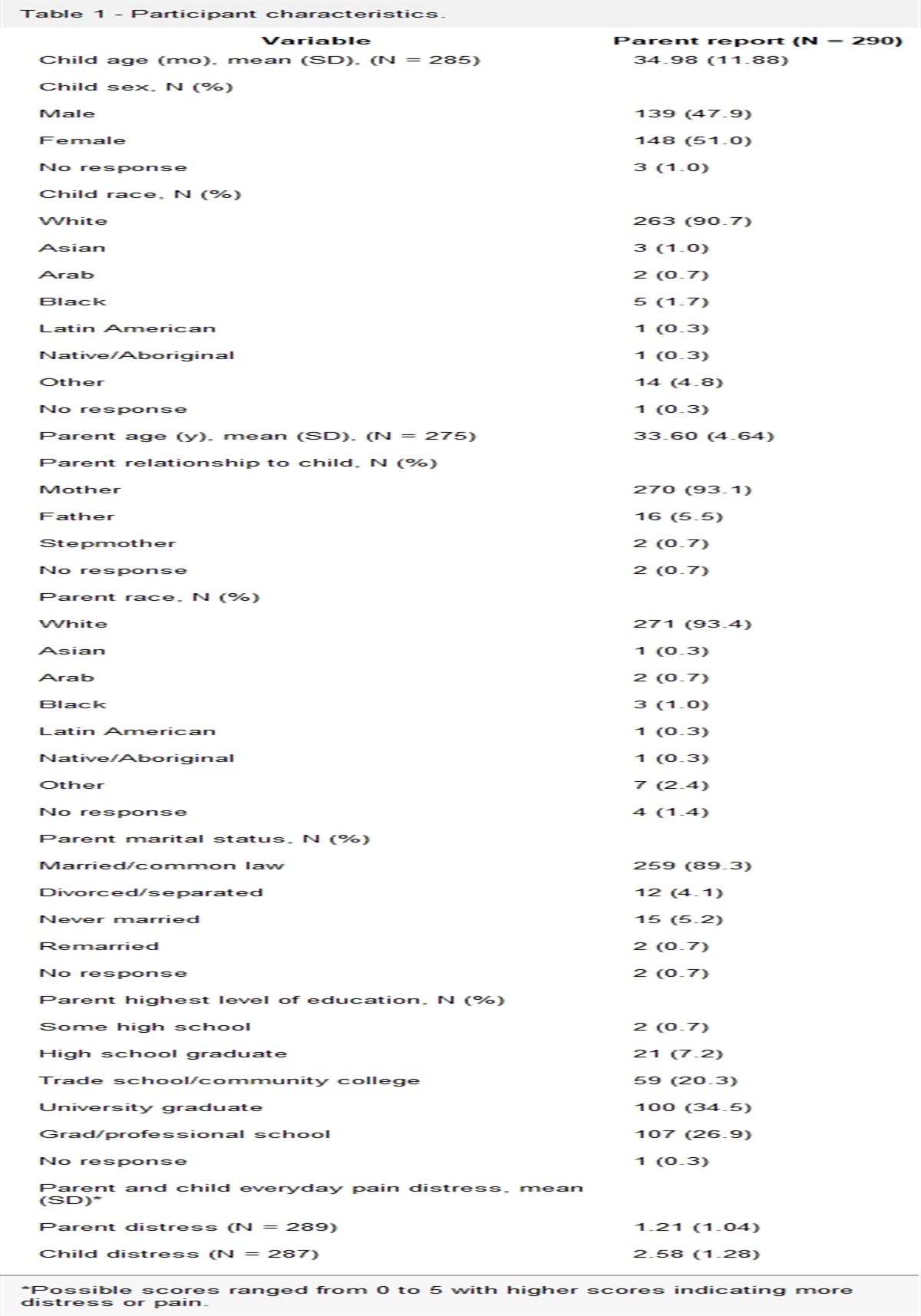
2. Methods 2.1. ParticipantsIn this study, 134 participants were eligible at the chronic pain centre of the hospital “Adolphe de Rothschild Foundation” in Paris, among them 97 women (72.4%) and 37 men (27.6%). The average age was 53.2 years (SD = 14.5). The majority were married (45.9%) or cohabiting (8.27%) with their partner. Forty-seven percent of them had a higher education diploma. Table 1 describes the sociodemographic characteristics of all eligible participants.
Table 1 - Sociodemographic characteristics. Variable N = 134 Overall, n (%) Sex WomenThis is a quantitative study that was performed using a sociodemographic questionnaire and 3 self-report questionnaires:
The Relationship Scale Questionnaire—Reviewed Coding (RSQ-CR) was developed by Bartholomew and Horowitz,2 and its coding of the French version was reviewed by Tereno et al.29 The RSQ-CR is an adult attachment self-administered scale that has as output variables a global security scale and 4 subscales that define 4 different attachment styles. Each of the 30 items is scored on a range of a 5-point Likert scale (RSQ-CR scoring details in supplementary materials, available at https://links.lww.com/PR9/A199).
The RSQ-RC has a satisfactory internal consistency in its scales, and Cronbach's α was 0.69 to 0.82. For the factor “detached” (α = 0.69), “secure” (α = 0.73), “preoccupied” (α = 0.76), and “disorganised” (α = 0.79), the internal consistency was globally good, and for the factor “global security index” (α = 0.82), the internal consistency was very good.29
The Self-Compassion Scale (SCS)15,24 is a self-compassion questionnaire for adults that includes of 26 items, coded in a 5-point Likert scale and grouped into 6 subscales that measure 3 main components: self-compassion vs self-judgment, common humanity vs isolation, and mindfulness vs overidentification (SCR scoring in supplementary materials, available at https://links.lww.com/PR9/A199).
The French version of SCS has a satisfactory internal consistency in its scales, and Cronbach's α was 0.74 to 0.88. For the factors “common humanity” (α = 0.74), “overidentification” (α = 0.77), and “isolation” (α = 0.79), the internal consistency was good. For the factors “self-judgment” (α = 0.85), “mindfulness” (α = 0.81), and “self-care” (α = 0.89), the internal consistency was very good. Internal reliability for the total score of the French version of the SCS was excellent (α = 0.94).15
The Brief COPE (state version)23 is a 28-item self-administered questionnaire of the coping state, which takes into account the specific way in which people cope with a given stressful situation. It is composed of 14 subscales (2 items each) assessing the following distinct coping dimensions: (1) active coping, (2) planning, (3) seeking instrumental social support, (4) seeking emotional social support, (5) expressing feelings, (6) behavioural disengagement, (7) distraction, (8) blaming, (9) positive reinterpretation, (10) humour, (11) denial, (12) acceptance, (13) religion, and (14) substance use. Participants rate each item on a four-point Likert scale: “I have not been doing this at all,” “a little bit,” “a medium amount,” and “I have been doing this a lot,” score 1 to 4 for each item, and no reverse scoring.
The French version of Brief COPE state version has good psychometric qualities. The confirmatory factor analysis showed satisfactory results. The χ2 obtained was equal to 391, P < 0.05. The GFI was 0.87, the AGFI was equal to 0.80, and the RMR less than 0.06.23
Muller and Spitz23 make a distinction between functional coping strategies and dysfunctional coping strategies: Functional strategies aim to adjust the person to the situation and to preserve a certain quality of life (planning, active coping, positive reframing, and acceptance); some strategies are functionally variable (instrumental support, emotional support, venting, religion, humour, and distraction), and their functional variability depends on the circumstances and the particular use by each. Dysfunctional strategies do not promote a person's adjustment to a given situation, nor their well-being in the face of this situation (self-blame, denial, substance use, and behavioural disengagement).
2.3. Procedures 2.3.1. Recruitment proceduresEach patient with chronic pain (defined as pain persisting longer than 3 months) who made a new request for treatment at the chronic pain centre of the hospital “Adolphe de Rothschild Foundation” in Paris during the study's inclusion period (December 2018–December 2020) was consecutively offered to participate in the research. Inclusion criteria were being an adult (older than 18 years), French-speaking or bilingual, and affiliated or a beneficiary of a Social Security plan. Patients already treated in another pain centre in the past, patients being followed for cancer, breastfeeding women, patients being followed for Parkinson disease, and patients with a previous psychiatric diagnosis. Patients benefiting from a legal protection measure were excluded from the research, according to the guidelines of the French Ethics Committee. All patients who agreed to participate have completed informed and written consent.
The study adhered to the tenets of the Declaration of Helsinki. A French Ethics Committee (Comité de Protection des Personnes Est IV) approved this study on October 9, 2018 (IDRCB: 2018-A01167-48). This clinical study was registered at clinicaltrials.gov under the number NCT: NCT03845816.
2.3.2. Administrative proceduresFor the comfort of the participants, an appointment with the psychologist–researcher of the chronic pain centre was proposed to them on the same day of one of their 2 first appointments. At the end of this first assessment, an additional, but optional, appointment was proposed for the restitution of the results of the questionnaires and for a possible therapeutic orientation.
2.3.3. Statistical proceduresData were statistically analysed using R (version 4.0.3). Descriptive statistics are reported as mean and SD for continuous variables and as frequency and percentages for categorical variables. t test, or Wilcoxon test, when appropriate, was used to compare continuous variables (self-compassion scores, coping strategies scores, and attachment quality scores) between groups (secure vs insecure attachment; women vs men). Nonparametric test was used if assumptions were not met. χ2 test, or Fisher exact test when appropriate, was used to compare qualitative parameters (sex and attachment type). Correlations of self-compassion scores, coping strategies scores, and attachment quality scores were realised using Pearson method or Spearman method when appropriate. As an exploratory analysis, multivariate linear regression was conducted to assess the association of attachment type on global self-compassion score adjusted to sex. Because it is an exploratory study, no correction of multiple testing was realized. A mediation analysis was realised to found if total self-compassion mediated between attachment type and coping strategies. A P-value <0.05 was considered as statistically significant.
3. Results 3.1. Sample description at inclusionRegarding their pain status, described in Table S1, available at https://links.lww.com/PR9/A199, participants presented most frequently, peripheral neuropathic pain (15%), low back pain (15%), headaches (9.8%), and central neuropathic pain (8.3%).
3.2. Attachment qualityIn our sample, the mean of secure score was 4.30 (SD = 0.61), which is higher than the secure threshold point of 3.67. Regarding attachment quality, described in Table 2, of all the participants, 45.5% (n = 60) had a secure attachment style, and 54.5% (n = 72) had an insecure attachment style.
Table 2 - Attachment quality. Attachment pattern (N = 134) Mean (SD) n (%) P Secure 4.30 (0.61) 72 (54.5) P < 0.001* Insecure 2.73 (0.63) 60 (45.5) Secure women 4.28 (0.55) 44 (73.3) Secure men 4.22 (0.66) 16 (26.7) Insecure women 2.48 (0.53) 51 (70.8) n.s.† Insecure men 2.54 (0.59) 21 (29.2)*Fisher exact test.
†χ2 test.
As seen in Table 3, subjects in our sample had a mean of self-compassion of 2.92 (SD = 0.64), which corresponds to a moderate level of self-compassion (moderated level from 2.5 to 3.5 to the SCS scale). All other subscale scores were moderate for our population. The overidentification, self-judgement, and isolation subscales indicate less self-compassion, and they are reversed for the total score calculation. Men reported a significantly (P = 0.02) higher mean of global self-compassion score (mean = 3.13; SD = 0.61) when compared with women (mean = 2.84; SD = 0.63). Self-kindness scores were also significantly (P = 0.008.) higher in men (mean = 3.17; SD = 0.97) compared with women (Mean = 2.66; SD = 0.94).
Table 3 - Self-compassion. Self-compassion (N = 134) Total*Reverse score.
†Student t test.
‡Wilcoxon test.
Table 4 shows mean values and SDs of the use of coping strategies. Two Wilcoxon tests were performed with 2 different variables: sex and attachment quality (secure or insecure). Women in our sample (mean = 4.49; SD = 1.74) reported significantly lower (P = 0.05) acceptance coping compared with men (mean = 5.59; SD = 1.94). Securely attached individuals reported a significantly higher (P = 0.02) mean of active coping score (mean = 5.22; SD = 1.44) compared with insecurely attached individuals (mean = 4.60; 1.59).
Table 4 - Coping strategies. Coping strategies (N = 134) Mean (SD) Women (N = 97)t test showed that securely attached participants (mean = 3.14; SD = 0.61) reported a significantly higher (P < 0.001) global self-compassion score compared with the insecurely attached individuals (mean = 2.73; SD = 0.61). The securely attached subjects also reported significantly higher levels (P = 0.01) of self-kindness (mean = 3.01; SD = 1.01), compared with the insecurely attached ones (mean = 2.62; SD = 0.90). Scores on the isolation items were also significantly higher (P = 0.002) for the securely attached patients (mean = 3.29; SD = 1.13), compared with insecure attachment ones (mean = 2.69, SD = 0.96) (Fig. 1, Table S2, available at https://links.lww.com/PR9/A199).
 Figure 1.:
Figure 1.: Attachment and self-compassion—comparisons between secure and insecure groups on attachment and self-compassion variables using the Student test or Wilcoxon test.
At an alpha risk set at 0.05, in multivariate analysis, being a woman decreases the total self-compassion score (−0.30 [−0.53 to −0.07], P 0.01) compared with being a man, and having a secure attachment increases the total self-compassion score (0.41 [0.20–0.61], P < 0.001) compared with having an insecure attachment.
Correlation analysis (Fig. 2, Table S3, available at https://links.lww.com/PR9/A199) showed that the global security scale was significantly and positively correlated with global self-compassion (r = 0.41, P < 0.05), self-kindness (r = 0.26, P < 0.05), self-judgment (r = 0.29, P < 0.05), isolation (r = 0.35, P < 0.05), mindfulness (r = 0.23, P < 0.05), and overidentification ones (r = 0.38, P < 0.05).
 Figure 2.:
Figure 2.: Correlations between attachment quality and self-compassion.
Insecure detached attachment scale was significantly and negatively correlated with self-judgment (r = −0.27, P < 0.05), with isolation (r = −0.31, P < 0.05), and with total self-compassion scores (r = −0.30, P < 0.05). Insecure disorganised attachment score was significantly and negatively correlated with self-judgement (r = −0.24, P < 0.05) and isolation score (r = −0.05, P < 0.05).
3.6. Attachment quality and coping strategiesTable 5 presents the correlations between attachment styles and coping strategies implemented by patients with chronic pain. The global security score was correlated significantly and positively with instrumental support (r = −0.19, P < 0.05) but negatively with behavioural disengagement coping (r = 0.35, P < 0.05). Preoccupied attachment was significantly and positively correlated with instrumental support coping (r = 0.19, P < 0.05) and with emotional support coping (r = −0.2, P < 0.05). Secure attachment score was significantly and positively correlated with the active coping (r = 0.29, P < 0.05), planning coping (r = 0.28, P < 0.05), instrumental support coping (r = 0.30, P < 0.05), and significantly and negatively correlated with behavioural disengagement coping (r = −0.46, P < 0.05). Preoccupied attachment was significantly and negatively correlated with emotional support coping (r = −0.29, P < 0.05).
Table 5 - Spearman rank correlation between attachment quality and coping strategies. Secure Detached Disorganized Preoccupied Global security Active coping 0.29* 0.03 0.03 0.03 −0.16 Planning 0.28* 0.00 0.03 −0.01 0.01 Use of instrumental support 0.34* 0.13 −0.11 −0.18 0.19* Use of emotional support 0.30* 0.11 −0.16 −0.29* 0.13 Venting 0.23 0.08 −0.11 0.01 0.12 Positive reframing 0.21 −0.06 −0.08 −0.17 0.17 Acceptance 0.09 −0.01 0.14 −0.13 0.08 Denial 0.03 −0.05 0.10 0.09 −0.02 Self-blame 0.01 0.05 −0.01 −0.01 −0.17 Humour 0.03 −0.09 0.12 −0.01 0.07 Religion 0.00 0.07 0.10 0.14 −0.17 Self-distraction 0.19 0.08 0.00 −0.12 0.13 Substance use 0.03 0.00 0.26* 0.15 −0.12 Behavioural disengagement −0.46* 0.09 0.12 −0.08 −0.2*Table 6 presents the correlations between coping strategies and self-compassion. Active coping was positively and significantly correlated with overall self-compassion score (r = 0.48, P < 0.05), as well as self-kindness (r = 0.29, P < 0.05), common humanity (r = 0.29, P < 0.05), isolation (r = 0.39, P < 0.05), mindfulness (r = 0.45, P < 0.05), and overidentification (r = 0.39, P < 0.05).
Table 6 - Spearman rank correlation between self-compassion and coping strategies. Self-kindness Self-judgment* Common humanity Isolation Mindfulness* Overidentification* Self-compassion Active coping 0.29† 0.04 0.29† 0.39† 0.45† 0.39† 0.48† Planning 0.07 −0.14 0.15 0.12 0.33† 0.11 0.15 Use of instrumental support 0.06 −0.06 0.1 0.11 0.12 0.11 0.11 Use of emotional support −0.01 −0.17 0.01 −0.08 0.06 −0.16 −0.09 Venting 0.06 −0.18† 0.00 0.02 0.05 −0.07 −0.03 Positive reframing 0.35 0.00 0.31† 0.24
留言 (0)