
記住我









The prevalence of chronic wounds is conservatively estimated at 4% of the adult population in developed countries.17,32 The incidence of chronic pain in individuals with a lived experience of chronic wounds is estimated to be as high as 85%, with pain reported to be one of the most distressing aspects of the chronic wound experience.4,14,19,20,27 Chronic pain is defined by the International Association for the Study of Pain as “An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.”31 Chronic pain affects many aspects of the individual's life and often exists concomitantly with conditions such as anxiety, depression, and cognitive impairment.6,18,24
Currently available therapeutics for the management of chronic pain are typically given as systemic preparations and include a wide variety of drug classes. Examples of commonly used analgesics include nonsteroidal anti-inflammatories (NSAIDS), opioid medications, and atypical analgesics including antiepileptics such as gabapentin, which is commonly used for neuropathic pain conditions.34,35 There exists several topical-based preparations for the prevention, management, and treatment of chronic pain and wound-associated pain, including local anaesthetics, anti-inflammatory foam dressings, and topical opioid medication.1,5,25,30 The therapeutic potential of topical cannabis-based medicines for the management of wound-associated pain and wound healing has been highlighted in several recent case reports.7,21,22
A previous Cochrane review of topical agents or dressings for pain limited to those with venous leg ulcers only identified 2 randomised controlled trials (RCTs) meeting their criteria.5 One study showed significantly more participants in the ibuprofen group achieving >50% total maximum pain relief score between day 1 and day 5 compared with the control group, whereas the second study showed no statistically significant difference in the proportion of participants experiencing slight to complete pain relief on the first evening of treatment. The following systematic review aims to establish a robust understanding of the level of efficacy of topical interventions available for the management of wound-associated pain in individuals with a lived experience of chronic wounds.
2. MethodsA full protocol for this review has been submitted for publication.16 Ovid Embase, Ovid MEDLINE, EBSCOhost, CINAHL, the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Web of Science, and Scopus were searched from inception to present with no limits on language alongside OpenGrey and Eudra CT for gray literature and registered clinical trials, respectively [All sources were searched between June 25, 2021, and July 1, 2021]. The most recent article was added on the 15th of November 2022.28 Searches were developed iteratively with PRESS Guideline Evidence-Based Checklist23 in mind. This was a stepped process, with terms being developed to capture 3 distinct concepts: different types of chronic wound, pain experienced because of chronic wounds, and interventions used to alleviate the wound-related pain.
2.1. PopulationThis review is limited to individuals older than 18 years who have chronic wounds including venous, arterial, mixed arterial venous, diabetic ulcer, or pressure ulcer. Studies which included individuals with surgical, acute, burn, or otherwise atypical wounds were excluded. Where more than one wound aetiology was reported, the article was included if a subset of the participants met the above criteria alongside the data being presented based on accordant aetiology.
2.2. Type of studyOnly RCTs were included in this review. Allocation method was open provided it fitted the criteria of an RCT (eg, clustered). Quasirandomised studies, reviews, and case studies were excluded.
2.3. ComparatorsStudies which compared any one intervention compared with another, or studies with any one intervention compared with a placebo were included.
2.4. Primary outcomesStudies required having pain as a primary outcome measure to be included. The primary outcomes were as follows:
(1) The proportion of participants with any reduction or improvement in pain intensity. (2) Any assessments of pain intensity measured on a continuous scale (eg, numerical rating or visual analogue scales). 2.5. Secondary outcome measuresBased on a process of public patient involvement from the Alliance for Research and Innovation in Wounds and with reference to the recommendations by IMMPACT,9 the following secondary outcomes were included:
(1) The proportion of participants with ≥30% reduction in pain intensity (equivalent to a moderate improvement defined by IMMPACT).9 (2) Reported changes in disability or physical functionality. (3) Reported changes in emotional functionality or impact on mental health (eg, anxiety, depression, mood, etc). (4) Reported changes to quality-of-life score, measured using any quality-of-life assessment tool. (5) Adverse events. For this review, adverse events will include reported measures of harm, withdrawal because of adverse events or serious adverse events, patient-reported adverse events, and specific adverse events—especially central nervous system (CNS) and cardiovascular. We will describe how adverse events were addressed, how they were reported, and over what time the harm was experienced as per the PRISMA harms checklist.36 (6) Rescued analgesia requirements (eg, time to rescue). (7) Patient-reported changes to sleep quality and duration. (8) Analgesic effect onset and duration. (9) Reported changes in cognitive functioning. 2.6. ProcedureAfter the conclusion of searches, deduplication was performed using EndNote and subsequently transferred to Rayyan (rayyan.qcri.org) for the second phase of deduplication and screening. Disagreements were resolved by discussion between 2 authors with referral to a third author when required. At least 2 members of the study team screened all titles and abstracts (randomly allocated). Full text of any studies or reports identified as potentially relevant was retrieved. All studies excluded from the review at this stage were listed as excluded, with reasons (PRISMA flowchart Fig. 1).
 Figure 1.:
Figure 1.: PRISMA flow diagram.
To create a more homogenous understanding of the screening process, team members who were involved with screening performed a pilot calibration exercise on a random sample of 100 references until 90% agreement was reached. Similarly, 2 review authors independently extracted data from included studies. Again, at least 2 review authors screened full-text studies for inclusion or exclusion. Any discrepancies were resolved by discussion until consensus was reached or through consultation with a third review author, when necessary.
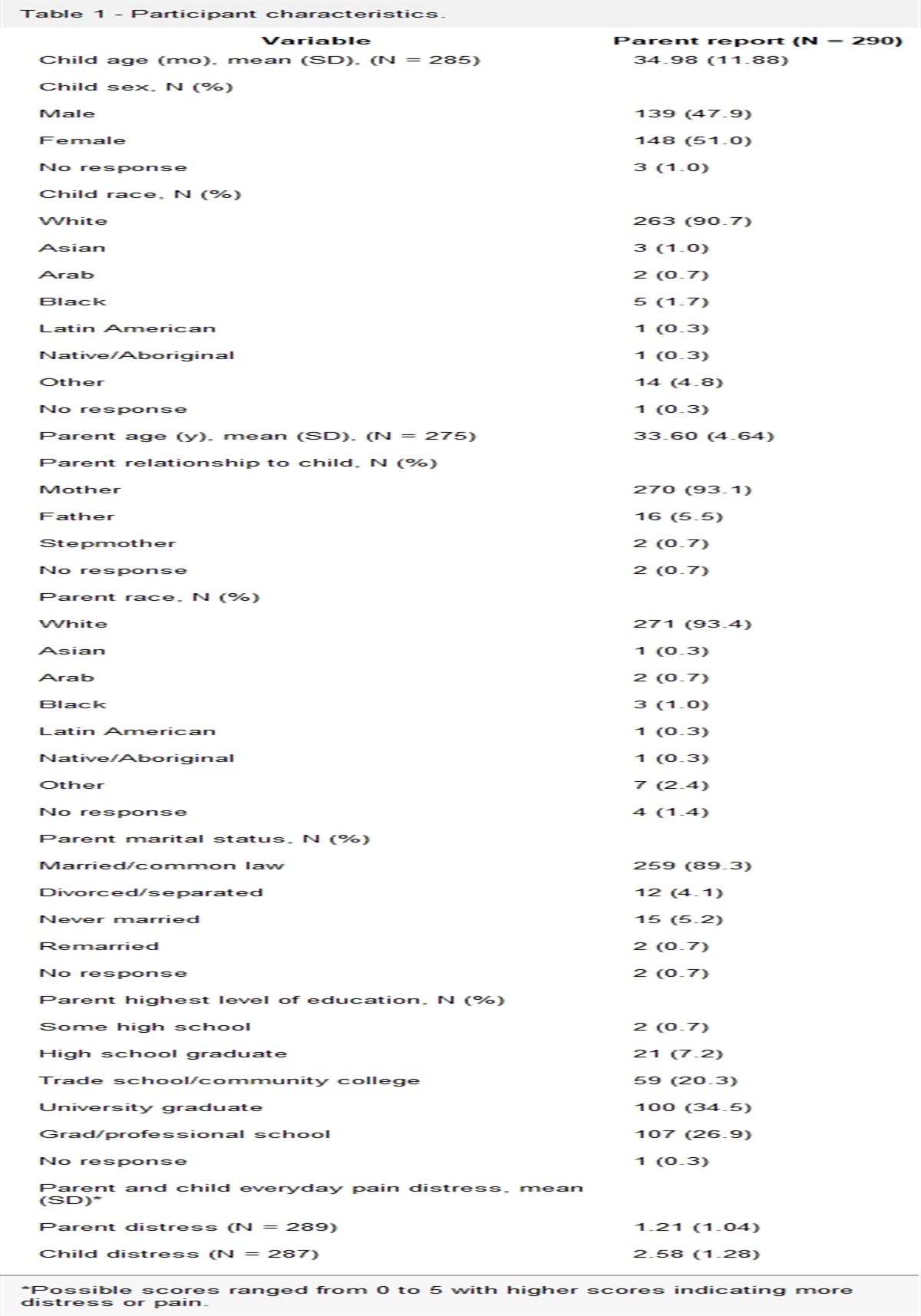
3. ResultsSearches retrieved 10,327 titles and abstracts (7,760 after deduplication). Eighteen studies were selected for full-text review, of which 9 (n = 1323 participants) examining the following were retained: ibuprofen (n = 4), morphine (n = 2), BWD + PHMB [polihexanide-containing biocellulose wound dressing] (n = 1), and EMLA (n = 2) (Table 1 for further details). The results of these searches are presented in the PRISMA flowchart Figure 1. Of the 9 included trials, 3 were multicentre/multinational, with the remainder in Canada, Switzerland, Australia, Sweden, and the United States. Combined statistical or meta-analysis was not possible because of differences in frequency and dosage of interventions and differences in timing and methods used to assess (combined) outcomes, and thus, a narrative review is reported here.
Table 1 - Summary of results table. Sibbald et al.,33 2007 Gottrup et al.,13 2008 Domenech et al.,8 2008 Fogh et al.,12 2012 Flock,11 2003 Bastami et al.,2 2012 Eberlein et al.,10 2012 Purcell et al.,28 2017 Purcell et al.,29 2017 No. of participants 24 122 853 120 13 21 50 60 60 Wound aetiology Chronic painful exudation leg ulcer Painful chronic VLU >8 wk Painful wounds with moderate-to-severe levels of exudate Painful, moderately to highly exuding, chronic VLU >8 wk Inpatients with painful stage II or III pressure ulcers with surrounding erythema Painful leg ulcer Wounds of various aetiologies and minimal bacterial load Chronic lower leg ulcer of at least 6-wk duration Chronic lower leg ulcer of at least 6-wk durationNRS, numeric rating scale; VAS, visual analogue scale.
Studies ranged in size from 13 to 853 participants with a mean of 147 and a median of 55. Studies involved predominantly female patients (52%–88%). The overall mean age was 71.9 years with a median of 70.3.
Four of the studies8,12,13,33 were partially or fully funded by Coloplast A/S. All author groups, funded by Coloplast, declared no conflict of interest except for Fogh et al.12 who included employees of Coloplast in their authorship list. The Research Council of Southeast Sweden funded one study.2 A clinical research grant from Lohmann & Rauscher GmbH & Co. funded one study.10 Three authors list conflicts of interests as members of the speaker's bureau and as consultants for the organisation.10 Two studies were funded by the New South Wales Health Nursing and Midwifery Innovation Scholarship, the Australian Wound Management Research Foundation, and the Central Coast Health Research Advisory Committee CHARM Research Grant.28,29 The remaining study lists no means of funding or conflicts of interest.11
3.2. Characteristics of excluded studiesStudies which were examined at the full-text stage and were subsequently excluded are presented here for clarity around their potential perceived relevance (Table 2).
Table 2 - Characteristics of excluded studies. Authors Title Journal Exclusion reason Agrifoglio et al. (2000) EMLA anesthetic cream for sharp debridement of venous leg ulcers: A double-masked, placebo-controlled study Phlebology, 15(2), 81–83 Pain not primary outcome Alvarez et al. (2012) An RCT to compare a bio-cellulose wound dressing with a non-adherent dressing in VLUs Journal of Wound Care, 21(9), 448–453. Pain not primary outcome Arapoglou et al. (2011) Analgesic efficacy of an ibuprofen-releasing foam dressing compared with local best practice for painful exuding wounds Journal of Wound Care, 20(7), 319–325. Subgroup analysis Chatterjee et al. (2019) Randomized controlled trial of topical mupirocin versus mupirocin with sucralfate combination in chronic skin ulcers Indian Journal of Pharmacology, 51(5), 316 Pain not primary outcome Dimikakos et al. (2011) An ibuprofen-releasing foam dressing provided clinically relevant pain relief for exuding, painful, chronic, and traumatic wounds of different aetiology EWMA Journal. 2011; Vol. 11:2 Suppl Subgroup analysis Hansson et al. (1993) Repeated treatment with lidocaine prilocaine cream (emla(r)) as a topical anesthetic for the cleansing of venous leg ulcers—a controlled-study Acta Dermato-Venereologica, 73(3), 231–233 Procedural pain was assessed and not ongoing wound pain. Jorgensen et al. (2005) The silver-releasing foam dressing, Contreet Foam, promotes faster healing of critically colonised venous leg ulcers: a randomised, controlled trial International Wound Journal, 2(1), 64–73 Pain not primary outcome Purcell et al. (2018) Eutectic mixture of local anesthetics (EMLA) as a primary dressing on painful chronic leg ulcers: a pilot randomized controlled trial Pilot and Feasibility Studies, 4(1), 1–13. Pain not primary outcome Romanelli et al. (2009) Ibuprofen slow-release foam dressing reduces wound pain in painful exuding wounds preliminary findings from an international real-life study Journal of Dermatological Treatment 2009; 20(1):19–26 Subgroup analysisThe Cochrane Risk of Bias 2 tool15 was used to assess the risk of bias (RoB) across 5 domains (plus one subdomain) within each study. The randomization process performed best across all studies because 75% had a low risk of bias. Fifty percent reported sufficient time between identification and eventual randomization and likewise for following intended interventions. The domain related to missing outcome data performed worst across studies because 50% had a high RoB, and one study did not provide information to make a determination. One study13 had a low RoB across 5 of the 6 domains (and subdomains) and was thus deemed to have the lowest RoB of all studies (Fig. 2).
 Figure 2.:
Figure 2.: Risk of bias table of studies.
3.4. Primary outcomeThe results were grouped according to the topical intervention and presented sequentially below.
3.4.1. Overview of ibuprofen interventionsFour studies were included that reported the use of ibuprofen foam as their intervention.8,12,13,33 Two studies compared ibuprofen foam (ibuprofen concentration: 0.5 mg/cm2) with a nonmedicated placebo foam.12,13 Two hundred forty-two patients (n = 12012; n = 12213) were randomised across the 2 studies with 27 and 29 participants not completing each study, respectively. Fogh et al.12 explicitly prohibited the use of per need medication while the study of Gottrup et al.13 allowed regular medication; provided dose and timing remained consistent. The remaining 2 studies compared ibuprofen foam (ibuprofen concentration: 0.5 mg/cm2) with local best practice.8,33 877 patients (n = 8538; n = 2433) were randomised across the 2 studies with 77 and 0 participants not completing each study, respectively.
3.4.2. Ibuprofen foam vs controlBoth Gottrup et al.13 and Fogh et al.12 required participants at entry to have a minimum ulcer size of 1.6 cm in any direction and an ankle brachial pressure index of >0.8 as well as a minimum pain score of moderate on a 5-point scale. Dressing changes occurred on a 48-hour interval13 and was not specified by Fogh et al.12 The primary outcome assessed in the study of Gottrup et al.13 was both pain relief and pain intensity. Pain relief was assessed using a 5-point verbal rating scale and intensity using an 11-point numeric box scale. Patients rated both measures after dressing change and wound cleaning on day 2 and day 5 as well as days 45 and 47. Fogh et al.12 used a 5-point pain relief scale self-documented twice daily (morning and evening) day 1 through day 5.
Gottrup et al.13 reported significant improvements for the ibuprofen group on pain relief starting from the first evening and continuing to day 5 (P < 0.05). Seventy-four percent of the ibuprofen group experienced pain relief compared with 58% in the comparator group. Pain intensity was likewise better for the ibuprofen group days 1 to 5 (P < 0.003) with a reduction from 6.8 at baseline to 4.1 for the ibuprofen (40% reduction) while a 6.6 to 4.6 (30% reduction) was seen in the comparator. The wound pain intensity decreased for all patient's overtime from days 1 through 5 (P < 0.001).
Fogh et al.12 reported significantly greater pain relief in the intervention group (P = 0.044). This was found when calculating cut-off points of at least 50% improvement in pain relief. Evening responder data were analysed separately with findings remaining consistent in favour of the ibuprofen foam group (P = 0.006) with 35% of the foam group experiencing at least 50% pain relief compared with 16% in the comparator group. However, they did not report on the changes between baseline and subsequent pain relief or improvement on which the combined outcome was based.
3.4.3. Ibuprofen foam vs local best practiceSibbald et al.33 and Domenech et al.8 required a minimum wound area of 0.5 cm × 0.5 cm and 1 cm2, respectively. All patients in the study of Sibbald et al.33 at study entry experienced at least 3 on a 10-point verbal analogue scale. The study of Sibbald et al.33 comprised a 1-week intervention period with pain relief and pain intensity scores recorded twice daily (morning and evening). Pain relief was assessed using a 5-point verbal rating scale while intensity was measured using an 11-point numeric box scale. Domenech et al.8 similarly comprised a 1-week intervention period where participants recorded pain relief twice daily (morning and evening).
Sibbald et al.33 despite measuring pain relief and reporting as a primary outcome does not provide data on this outcome. Pain intensity scores improved in favour of the ibuprofen group (P = 0.04) in the morning with evening values showing similar results (P = 0.02). The pooled data (morning and evening) was likewise in favour of the ibuprofen group (P = 0.02). No additional information on percentage or frequency of improvement was provided.
Domenech et al.8 reported significant pain relief scores in favour of the intervention group (P < 0.0001) with almost 80% of patients experiencing relief within the first 24 hours compared with 59% in the local best practice group. Pain intensity decreased for both groups over time but with a larger reduction exhibited in the intervention group (P < 0.0001). Baseline intensity scores were 6.2 for the intervention group and 5.2 for the local best practice. After day 7, mean scores had reduced by 3.7 (60% reduction) in the intervention group and 1.5 (28% reduction) in the local best practice.
3.4.4. Overview of morphine interventionsTwo studies were included which reported morphine as the intervention and compared it with a control.2,11 34 participants (n = 13,11 2003; n = 212) were randomised across both studies with 6 and 4 participants not completing each study, respectively. Flock11 assessed pain scores using a 5-point scale through nursing staff asking participants to rate their ulcer-related pain. Pain was assessed before, 1 hour, and 12 hours after gel application. Bastami et al.2 used an 11-point visual analogue scale (VAS) assessed directly after gel application as well as at 2, 6, 12, and 24 hours.
Flock11 noted similar pain scores between groups before application and significant improvement for the intervention group at 1 (P = 0.003) and 12 hours (P = 0.005) of follow-ups. All patients (n = 6) had improved pain scores both at 1 and 12 hours with 4 patients being pain-free after 1 hour. Bastami et al.2 noted no significant difference between intervention and placebo condition when analysed as a whole (P = 0.172) despite higher mean pain scores in the placebo group (4.3 ± 2.8) vs morphine (3.8 ± 2.7).
3.4.5. PHMB vs local silver dressingOne study compared the efficacy of BWD + PHMB vs a best local standard silver dressing (Ag) (Eberlein et al.,10). Fifty patients were randomised, of whom 38 individuals (BWD + PHMB, n = 21; Ag, n = 17) with a total of 42 wounds (BWD + PHMB, n = 24; Ag n = 18) were included in the final analysis. Dressing changes occurred every second day or every third day over the weekends. Pain was assessed using a 10-point VAS comparing day 0 (start) and day 28 (end) and pain reduction over time.
For trial inclusion, all patients had to have a baseline pain score of >4 or 4 on a 10-point scale where 0 was no pain to 10 being worst possible pain. At day 0, those in BWD + PHMB reported a mean VAS pain score of 6.13 ± 1.43 vs 5.42 ± 1.43 in Ag group. These significantly reduced by day 28 for both groups (P < 0.001). Between-group comparisons are reported as VAS scores continuing to decrease by significantly greater amounts and faster over the 28-day study period for BWD + PHMB compared with AG-treated patients, although the results of between-group analysis to support this are lacking.
3.4.6. EMLA vs usual care/local best practicePurcell et al.29 compared the efficacy of 12 weeks of local usual care (dressing type and frequency determined by individual practitioner) with the usage of daily dressing change combined with a dose of EMLA cream (1–2 g/10 cm2). This was performed for 4 weeks before reverting to usual care for the remaining 8 weeks of the trial.29 Pain was assessed before dressing change, during the procedure, and within 10 minutes after the change of dressing. 60 patients were randomised, of whom 59 were included for analysis (intervention, n = 30; usual care, n = 29). Collected group demographics were comparable (eg, age, ulcer type, pain medications) except CLU duration in weeks which varied between groups (intervention, M = 26.4; usual care, M = 20.5).
Participants in both groups similarly reported congruent levels of wound-related pain at baseline assessment (intervention, M = 7.26, SD = 1.89; usual care, M = 7.36, SD = 1.89). Pain scores before dressing changes decreased across both groups over time with participants in both groups reporting similar pain throughout the duration. This indicates the intervention did not influence pain before dressing change (eg, week 2, intervention, M = 3.04, SD = 2.26; usual care, M = 3.64, SD = 2.22; P = 0.34).
This was in opposition to a previously conducted pilot study of Purcell et al.28 which found mean pain scores after dressing change were significantly lower for the intervention group over the 4-week period.
3.5. Secondary outcomes 3.5.1. The proportion of participants with any reduction or improvement in pain intensityFlock11 notes that 85% of patients (6 of 7) experienced an improvement in pain intensity 1 and 12 hours after morphine gel application. 57% (4 of 7) were pain-free after 1 hour, and 43% (3/7) remained so after 12 hours had passed.
3.5.2. Reported changes in disability or physical functionalityDomenech et al.8 report on overall mobility improvement in their study as reported by patients. Thirty-seven percent of the ibuprofen treatment group experienced increase in mobility compared with 18% in the comparator group (P < 0.001). There were also lower levels of deterioration for the treatment group (9%) vs the comparator group (16%).
3.5.3. Reported changes in emotional functionality or impact on mental health (eg, anxiety, depression, mood, etc)Domenech et al.8 report well-being improved significantly more in the ibuprofen treatment group 40% (n = 187) vs the comparator group 15% (n = 58) (P < 0.001). There were also lower levels of deterioration for the treatment group (4%) vs the comparator group (9%). Gottrup et al.13 reported on mood but found no significant differences between groups.
3.5.4. Reported changes to quality-of-life score, measured using any quality-of-life assessment toolQuality-of-life (QoL) metrics were reported in 3 studies.8,10,13 Domenech et al.8 used the WHO-5 Well-Being Index3 and observed improvements in the ibuprofen foam group vs nonmedicated control in 4 health parameters (appetite [22% vs 9% improvement], overall well-being [40% vs 15% improvement], mobility [37% vs 18% improvement], and social activities [17% vs 6% improvement]).
Gottrup et al.13 recorded data on quality-of-life indicators at baseline, day 5, and day 43. Both intervention and control influenced the patients' well-being and individual quality-of-life parameters positively. All patients' overall QoL improved during the trial from day 5 to day 43. Percentage of participants who experienced improvements from baseline in the ibuprofen group are as follows: sleep 53%, mood 45%, well-being 39%, and appetite 24%. However, no statistically significant differences were evident between groups.
Eberlein et al.10 assessed QoL using the Wurzburger quality-of-life score which consists of 19 different questions related to patients with chronic wounds. As pain was the primary outcome of the study, the authors modified the Wurzburger tool and removed the questions related to pain resulting in 17 questions remaining. Authors report that the dressings used in both the PHMB and silver dressing groups contributed to an improvement of various aspects of the patients' reported QoL with the same 4 subscores improving significantly over the study period (day 1, 2, 3, 14) (P < 0.05). Further detail is not provided.
Purcell et al.29 used the Cardiff Wound Impact Schedule (CWIS)26 which noted similar levels of health-related QoL scores at baseline. Scores in all subscales increased throughout the study in both groups; however, in the intervention group, only well-being reached significance (P = 0.03) and only from baseline to week 4. The effect dissipated after the conclusion of the intervention.
3.5.5. Adverse eventsAdverse events have been reported with consideration given to the PRISMA harms checklist where appropriate.36 The frequency of adverse events was reported in all studies. Two studies reported no adverse events having occurred in either group.10,33
Gottrup et al.13 reported 7 (12%) participants experiencing 10 adverse events in the ibuprofen foam group and 12 (19%) participants experiencing 21 adverse advents in the control group. In the ibuprofen group, the following were experienced: combined urticaria and eczema, n = 1; eczema alone, n = 1; and blisters, n = 2. In the comparator group, the following were experienced: eczema alone, n = 2, and blisters, n = 2. A breakdown of the severity of the adverse events was provided (Table 3).
Table 3 - Adverse events presented on severity and device relatedness.13 Type Ibuprofen foam Comparator group Unrelated Possibly related Related Total Unrelated Possibly related Related Total Mild (N/%) 1 (5) 3(14) 4 (19) 8 (38) 0 (0) 1 (10) 2 (20) 3 (30) Moderate (N/%) 2 (10)
留言 (0)