
Remember me


Severe maternal morbidity (SMM) is associated with racial and ethnic health disparities in the United States, and Black pregnant people experience the highest rates.1,2 Sociodemographic factors and structural, and systemic racism are known causes of disparities in SMM.1,2 Prior studies demonstrate anemia as a risk factor for SMM, particularly among Black pregnant people.2–5 However, the differential association of antepartum anemia by race and ethnicity, in the absence of hereditary anemias, is not as well characterized.6 The World Health Organization estimates that one third of all reproductive-age people have anemia, and up to 38% of pregnant people worldwide experience anemia.7 Antepartum anemia contributes to adverse maternal and infant outcomes, including postpartum hemorrhage, preterm birth, low birth weight, and stillbirth.8 Understanding the contribution of antepartum anemia to SMM by race and ethnicity is essential.
National guidelines are inconsistent in recommendations for the evaluation and treatment of antepartum anemia.9 Many guidelines have not been updated to reflect evidence-based alternatives to screening for iron-deficiency anemia in pregnancy.10,11 Before 2021, guidelines endorsed race-based hemoglobin cutoffs, and the implications are staggering: Black pregnant women were less likely to receive treatment options during the antenatal period.12 Public health reporting on antepartum anemia prevalence is limited, and gaps in evidence may result in patients receiving disparate levels of care.3,9,11,12
Our objectives were to evaluate the prevalence of antepartum anemia by race and ethnicity, to assess whether such differences contribute to differences in SMM and nontransfusion SMM, and to estimate the contribution of antepartum anemia to SMM and nontransfusion SMM.3
METHODSWe conducted a population-based study using live-birth and fetal death certificate records data linked to delivery hospitalization records from 2011 to 2020. Our study cohort included singleton pregnancies at or after 20 weeks of gestation with available study variables (n=3,998,523). Pregnant patients with hereditary anemias, including hemoglobinopathies (eg, sickle cell disease), were excluded. Out-of-hospital births and unlinked births were not included in our final cohort. The Stanford University IRB and California Committee for the Protection of Human Subjects approved this study. Strengthening the Reporting of Observational Studies in Epidemiology guidelines were followed. Guided by the conceptual model to address pathways in racial and ethnic disparities1 and public health critical race praxis,14 our research team includes partnership with patient and community stakeholders to inform our research questions and study design.15,16 Parallel to this work, our team conducted culturally congruent focus groups with Black pregnant patients to elicit perspectives in regard to anemia and adverse pregnancy experiences. Our qualitative assessments will be submitted separately.
Research by the Human Genome Project and anthropologic investigations affirms that race is a social and cultural context, not a biological one.17,18 We focus on race and ethnicity because they sit at the intersection of many socioeconomic factors, social determinants of health, and structural and systematic racism in health care.19 In this study, race and ethnicity serve as a measure to inform health care policies for historically marginalized and minoritized populations.15,20 We collected race and ethnicity from vital records birth certificate data, and pregnant patients are referenced by self-reported race and ethnicity categories as captured in these data.21 Patients who identified as Hispanic are categorized as Hispanic. If Hispanic ethnicity was not listed, the first reported race category was captured in our data. We then classified race and ethnicity per U.S. Office of Management and Budget categories. Asian and Pacific Islander categories were disaggregated because of historical variation in perinatal outcomes across groups.22 Studies comparing California vital records data with self-report cite greater than 94% sensitivity for Black or African American, Asian-Pacific Islander, European, and Hispanic people.23 Patients reporting more than one racial group were categorized as multiracial. Patients without specified race (missing and other) constituted less than 0.33% of the population and were excluded from final analysis because of limited statistical power.
Severe maternal morbidity includes cases in which patients may have had a blood transfusion as the only qualifying event for SMM (ie, any of the 21 indicators for SMM defined by the Centers for Disease Control and Prevention [CDC]) during the birth hospitalization.24 Nontransfusion SMM (SMM excluding blood transfusion–only cases) includes SMM cases defined by any of the 20 or more SMM indicators by the CDC except for blood transfusion as the only indicator. We identified variables for SMM and nontransfusion SMM with International Classification of Diseases (ICD), Ninth and Tenth Revision codes (Appendices 1 and 2, available online at https://links.lww.com/AOG/D327).
Antepartum anemia is defined by the CDC as hemoglobin less than 11 g/dL in the first and third trimesters and less than 10.5 g/dL in the second trimester.25 We identified antepartum anemia on birth admission by race and ethnicity using ICD-9 and ICD-10 codes.3,26–30 Additional covariates identified included social determinants of health (age, insurance, education), prepregnancy body mass index (BMI, calculated as weight in kilograms divided by height in meters squared), prenatal care, parity, mode of delivery, obstetric comorbidity score (composite score of maternal comorbidities), and anemia.8,31 Maternal comorbidities included hypertension (chronic or gestational), gestational diabetes mellitus, and preexisting diabetes. The variables from the hospitalization data include anemia, SMM, comorbidities, and payment. All other variables are from the birth certificate data. We conducted a complete case analysis for missing data (Appendix 3, available online at https://links.lww.com/AOG/D327).
In aggregate data by race and ethnicity, descriptive statistics were used to examine maternal characteristics, social determinants of health, and obstetric comorbidities by antepartum anemia and SMM status. We identified antepartum anemia prevalence by race and ethnicity from 2011 to 2020. To evaluate for disparities in the prevalence of anemia and its contribution to SMM, we performed multivariable logistic regression models for the association between race and ethnicity and SMM. We sequentially adjusted the models for social determinants of health (age, education, insurance), clinical factors (parity and obstetric comorbidity score, not including anemia), delivery mode, and anemia. Models represented known confounders of the relationship between anemia and SMM.8,25,30 Antepartum anemia was adjusted last to isolate the effect on SMM status and evaluate whether anemia is a mediator of SMM and race. The estimated odds ratios approximated risk ratios (RRs) because of the rare outcome of SMM and are reported as such. All multivariable analyses were replicated for the outcome of nontransfusion SMM.
Next, to estimate the contribution of antepartum anemia to SMM by race and ethnicity, we used parametric g-computation to calculate population attributable risk percentages within each racial–ethnic group: ( ).32,33 We bootstrapped these simple substitution models (parametric g-computation) 1,000 times to obtain 95% CIs. This statistical method offers indirect estimation of the total effect of anemia on SMM and nontransfusion SMM.32 The population attributable risk percentages were adjusted for the same set of covariates: age, education, insurance, obstetric comorbidity score, parity, and delivery method. We used bootstrapping to estimate 95% CIs for the adjusted population attributable risk percentages of SMM and nontransfusion SMM. Data were analyzed in SAS 9.4 and R 4.1.3.
).32,33 We bootstrapped these simple substitution models (parametric g-computation) 1,000 times to obtain 95% CIs. This statistical method offers indirect estimation of the total effect of anemia on SMM and nontransfusion SMM.32 The population attributable risk percentages were adjusted for the same set of covariates: age, education, insurance, obstetric comorbidity score, parity, and delivery method. We used bootstrapping to estimate 95% CIs for the adjusted population attributable risk percentages of SMM and nontransfusion SMM. Data were analyzed in SAS 9.4 and R 4.1.3.
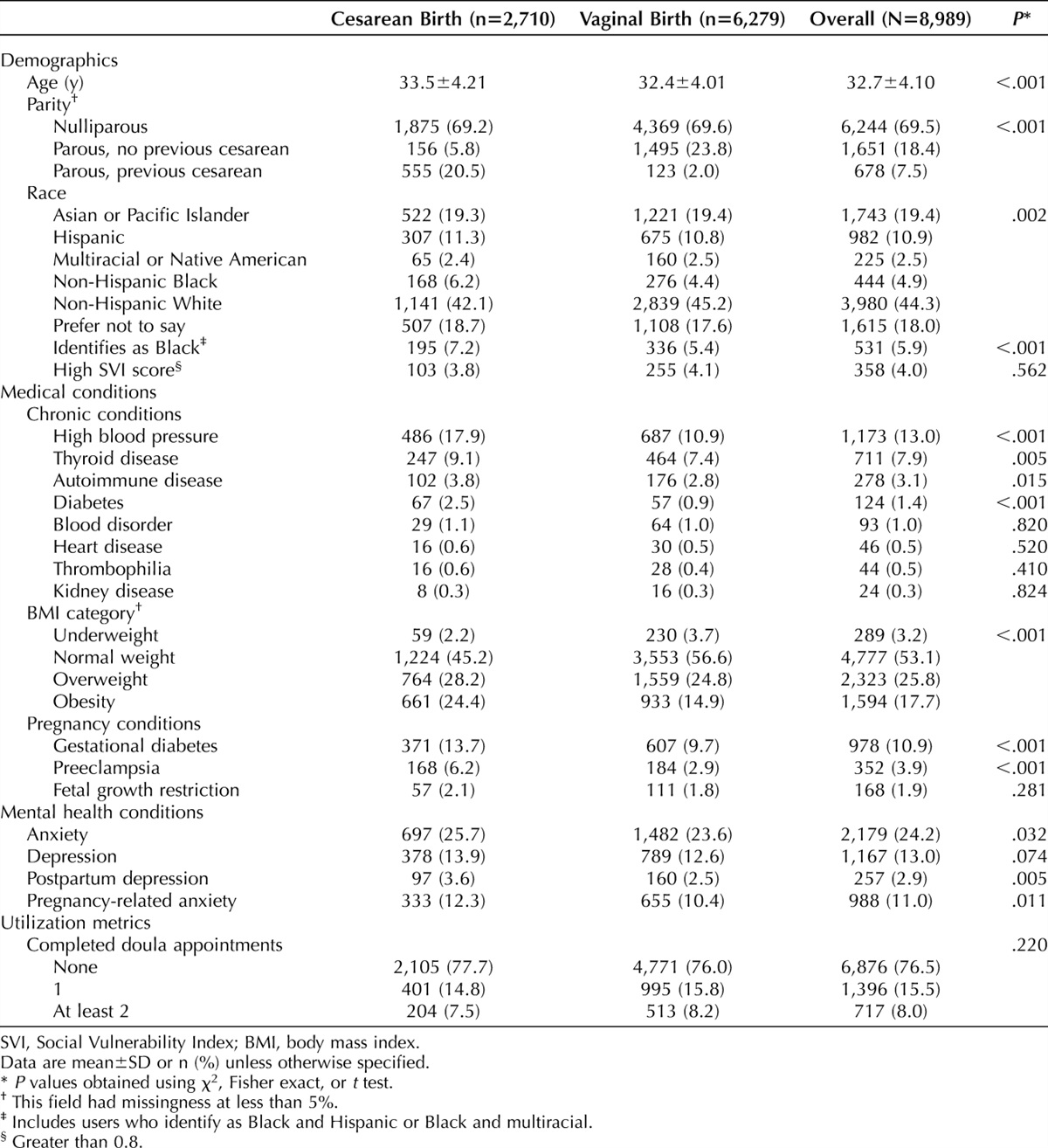
During the study period, there were 4,740,434 births in California. We analyzed 3,863,594 births after exclusion criteria were applied (Fig. 1). Most patients were aged 25–34 years, initiated prenatal care in the first trimester, had prepregnancy BMIs lower than 30, and had at least one prior birth (Table 1). Gestational diabetes mellitus, pregestational diabetes, and hypertension disorders of pregnancy were more common in patients with antepartum anemia and SMM, and obstetric comorbidity scores were higher in this group. Cesarean deliveries were more common among patients with SMM.
 Fig. 1.:
Fig. 1.: Study sample selection. *Race, ethnicity, age, education, nativity, parity, gestational age, and delivery body mass index.
 Table 1.:
Table 1.: Distribution of Maternal Characteristics in Pregnant Patients With Antepartum Anemia in California, 2011–2020 (n=4,414,118)*
In 2020, Black pregnant people had the highest prevalence of antepartum anemia (21.5%), followed by Pacific Islander (18.2%), American Indian–Alaska Native (14.1%), multiracial (14.0%), Hispanic (12.6%), Asian (10.6%), and White (9.6%) pregnant patients (Fig. 2 and Appendix 2, https://links.lww.com/AOG/D327). Next, we assessed differences in antepartum anemia by race and ethnicity. Anemia prevalence doubled to tripled from 2011 to 2020 for all groups: American Indian–Alaska Native (4.3–14.1%), Asian (5.0–10.6%), Black (10.7–21.5%), Hispanic (6.1–12.6%), multiracial (6.0–14.0%), Pacific Islander (7.1–18.2%), and White (4.5–9.6%) pregnant patients (Fig. 2). A significant and persistent disparity in anemia was noted between Black and White pregnant patients over time (an absolute difference of 6.2 percentage points in 2011 and 11.9 percentage points in 2020) (Fig. 2).
 Fig. 2.:
Fig. 2.: Trends in antepartum anemia in pregnant patients, 2011–2020.
We then evaluated how differences in antepartum anemia by race and ethnicity contributed to disparities in SMM. The incidence of SMM was higher in all pregnant patients with anemia compared with those without anemia (Table 2). The SMM incidence in patients with anemia was highest in Pacific Islander (6.5%), followed by American Indian–Alaska Native (6.3%), Black (5.1%), Hispanic (4.6%), multiracial (4.2%), Asian (3.8%), and White (3.4%) pregnant patients. In comparison, when anemia was not present, the SMM incidence across different racial and ethnic groups ranged from 1.0% to 1.8% (Table 2). Compared with White patients, the unadjusted risk for SMM was elevated in Pacific Islander (crude RR 2.06, 95% CI 1.85–2.28), Black (RR 1.91, 95% CI 1.85–1.98), and American Indian–Alaska Native (crude RR 1.85, 95% CI 1.64–2.08) pregnant patients. Modeling for sociodemographic, clinical, and delivery factors reduced the relative risk of SMM for most groups (Table 2). Compared with the reference group, sequential modeling for social determinants of health, clinical factors, and delivery mode to antepartum anemia decreased the relative risk for SMM among Black patients (approximated RR 1.47, 95% CI 1.42–1.53 to approximated RR 1.27, 95% CI 1.22–1.32). SMM decreased minimally after similar adjustments for antepartum anemia in American Indian–Alaska Native, Asian, Pacific Islander, and Hispanic pregnant patients (Table 2). Compared with White patients, the full adjusted risk for SMM was highest among American Indian–Alaska Natives (approximated RR 1.53, 95% CI 1.35–1.73), Asian (RR1.32, 95% CI 1.30–1.37), and Black (approximated RR 1.27, 95% CI 1.22–1.32) patients.
 Table 2.:
Table 2.: Disparities in Severe Maternal Morbidity by Race and Ethnicity, California, 2011–2020 (N=3,863,594)
Next, we estimated the contribution of antepartum anemia to SMM by race and ethnicity. The RR of SMM and anemia within each racial and ethnic group was calculated; for all groups, anemia was associated with an approximately threefold increased SMM risk (Table 3). Population attributable risk percentages were adjusted for covariates within each race and ethnicity (Table 3). Antepartum anemia contributed to 21.4% (95% CI 17.5–25.0%) of SMM prevalence in multiracial patients, 20.9% (95% CI 18.1–23.4%) in Black patients, 20.9% (95% CI 19.9–22.1%) in Hispanic patients, 16.7% (95% CI 5.2–29.0%) in American Indian–Alaska Native patients, and 16.4% (95% CI 7.3–26.4%) in Pacific Islander patients. Asian and White pregnant patients had the lowest population attributable risk of antepartum anemia on SMM (Table 3).
 Table 3.:
Table 3.: Associations Between Anemia and Severe Maternal Morbidity by Race and Ethnicity, California, 2011–2020 (N=3,863,594)
The absolute incidence of nontransfusion SMM was less than 1% among all racial and ethnic groups without antepartum anemia (Table 4). Compared with White patients, the unadjusted risk of nontransfusion SMM was high in Black (RR 1.87, 95% CI 1.78–1.98), Pacific Islander (1.77, 95% CI 1.50–2.09), American Indian–Alaska Native (RR 1.40, 95% CI 1.14–1.73), Asian (RR 1.32, 95% CI 1.27–1.37), multiracial (RR 1.30, 95% CI 1.19–1.41), and Hispanic (RR 1.16, 95% CI 1.13–1.20) patients. Adjustments for available social determinants of health did not substantially modify the relative risk of nontransfusion SMM for any cohort (Table 4). Asian, Black, and Pacific Islander patients continued to have elevated nontransfusion SMM risk relative to most other racial and ethnic groups after full sequential adjustment of covariates. It is notable that Asian pregnant patients' nontransfusion relative risk (crude RR 1.32, 95% CI 1.27–1.37) remained relatively unchanged after full adjustment for covariates (approximated RR 1.34, 95% CI 1.29–1.40); a similar finding was noted among Hispanic patients (crude RR 1.16, 95% CI 1.13–1.20 to approximated RR 1.12, 95% CI 1.08–1.17) (Table 4).
 Table 4.:
Table 4.: Disparities in Nontransfusion Severe Maternal Morbidity by Race and Ethnicity, California, 2011–2020 (N=3,863,594)
Population attributable risk percentages showed that antepartum anemia contributed to less than 8 percent of nontransfusion SMM in pregnancy (Table 5). Not all results were statistically significant and are potentially reflective of small sample size within each racial and ethnic category.
 Table 5.:
Table 5.: Associations Between Anemia and Nontransfusion Severe Maternal Morbidity by Race and Ethnicity, California, 2011–2020 (N=3,863,594)
DISCUSSIONIn our cohort of 3,863,594 births, antepartum anemia was associated with SMM and nontransfusion SMM and contributed to nearly one in five SMM cases in Black pregnant patients. Disparities in anemia were also identified among American Indian–Alaska Native, Hispanic, multiracial, and Pacific Islander pregnant patients and contribute to disparities in SMM.
Our study identified a rise of anemia among every racial and ethnic group during the past decade. Black patients experienced a 100% increase in antepartum anemia, the greatest of any group, and Black–White disparities grew over time.34 The reasons for the increase and disparity in anemia are multifactorial. Causes of antepartum anemia can include preexisting gynecologic conditions (abnormal uterine bleeding, fibroids), pregnancy physiology, chronic illnesses, or inflammatory- and immune-mediated states.35 Structural racism, “the totality of ways societies foster racial discrimination,” is also evident in historical race-based hemoglobin cutoffs and the intersectionality of nutrition security with race and ethnicity.36–40 Persistent disparities in anemia suggest implicit inequalities in how historically marginalized communities are assessed and treated for anemia.9 Despite American College of Obstetricians and Gynecologists’ recommendations for routine complete blood cell count screening, there are screening inconsistencies in clinical settings.13,41 Many believe that national guidelines reflect outdated evidence on anemia in pregnancy and promulgate inequalities by race and ethnicity.9,34,42
Our data support a strong correlation between antepartum anemia and SMM; antepartum anemia drives SMM more than nontransfusion SMM for every racial and ethnic group. Although the adjusted population attributable risk percentages demonstrated that antepartum anemia contributed to one fifth of SMM among Black, Hispanic, and multiracial patients, it also contributed to one sixth of SMM among Pacific Islander and American Indian–Alaska Native patients. Reducing antepartum anemia can potentially reduce SMM. Our data also show that antepartum anemia also contributed to about 8% of nontransfusion SMM. This suggests that blood transfusions are a particular driver of SMM and that nontransfusion SMM may be a sign of increased risk for maternal end-organ injury and morbidity.
Our study has several strengths. These data reflect a diverse cohort of patients receiving obstetric care at more than 200 hospitals throughout California. We excluded patients with hereditary anemias because they warrant separate screening and management. We also identified antepartum anemia, anemia present at birth on admission, by billing codes. Our cohort allowed us to specify outcomes for American Indian–Alaska Native and Pacific Islander patients, groups not typically well represented in studies, and to identify that SMM remains elevated for these groups after adjustments for social determinants of health and obstetric comorbidities. In addition, we were able to disaggregate outcomes between SMM and nontransfusion SMM to identify the effect of antepartum anemia on each.43
Our study has several limitations, including risk of misclassification bias with the use of ICD-9 and ICD-10 codes to capture diagnosis and procedures. The possibility for measurement error remains if misclassification occurs. Although birth certificate data are informed by patient self-report during hospitalization, congruency among birth certificate data for Native Americans had a sensitivity of 54%.23 We were also unable to comment on the intersection of racial and ethnic disparities in anemia with index of concentrations at the extremes or social vulnerability index.15,44,45 Stratification of outcomes within the multiracial group was underpowered for additional analysis.46 Causality of antepartum anemia is also unknown because we did not have access to iron indices, hemoglobin values (anemia severity), and treatment. However, similar work analyzing antepartum anemia has demonstrated the reliability of the ICD-9 and ICD-10 codes.3,26,28–30 In addition, data reinforce that mild anemia (9–10.9 g/dL) is a risk factor for blood transfusion.8,47
The population attributable risks show that antepartum anemia also increases the risk of SMM among most racial and ethnic groups. Efforts to understands gaps in addressing antepartum anemia—especially inequalities in anemia screening and management and drivers of structural racism in antepartum anemia—are needed to narrow disparities of SMM.48 Fifty percent of pregnant patients in high-resource settings may have iron deficiency, and 1 in 10 enrollees in federal nutrition support programs is anemic.25,49 Qualitative assessments with diverse pregnant patient groups are important to understand patients' lived experience with anemia.19,50 Treatment of anemia is critical; a longitudinal observational cohort showed that adequate treatment of antepartum anemia can reduce preterm birth and preeclampsia.41 Comprehensive approaches inclusive of patient stakeholders are key to avoid proposing solutions that could inadvertently cause harm.51,52 We can glean valuable information from these data, informing future obstetric quality measures and interventions. Antepartum anemia is modifiable, and addressing anemia through an equity lens has potential for closing disparity gaps in SMM.
REFERENCES 1. Howell EA. Reducing disparities in severe maternal morbidity and mortality. Clin Obstet Gynecol 2018;61:387–99. doi: 10.1097/GRF.0000000000000349 2. Mujahid MS, Kan P, Leonard SA, Hailu EM, Wall-Wieler E, Abrams B, et al. Birth hospital and racial and ethnic differences in severe maternal morbidity in the state of California. Am J Obstet Gynecol 2021;224:219.e1–15. doi: 10.1016/j.ajog.2020.08.017 3. Leonard SA, Main EK, Scott KA, Profit J, Carmichael SL. Racial and ethnic disparities in severe maternal morbidity prevalence and trends. Ann Epidemiol 2019;33:30–6. doi: 10.1016/j.annepidem.2019.02.007 4. Early ML, Eke AC, Gemmill A, Lanzkron S, Pecker LH. Comparisons of severe maternal morbidity and other adverse pregnancy outcomes in pregnant people with sickle cell disease vs anemia. JAMA Netw Open 2023;6:e2254545. doi: 10.1001/jamanetworkopen.2022.54545 5. Freese KE, Bodnar LM, Brooks MM, McTigue K, Himes KP. Population-attributable fraction of risk factors for severe maternal morbidity. Am J Obstet Gynecol MFM 2020;2:100066. doi: 10.1016/j.ajogmf.2019.100066 6. Pavord S, Daru J, Prasannan N, Robinson S, Stanworth S, Girling J. UK guidelines on the management of iron deficiency in pregnancy. Br J Haematol 2020;188:819–30. doi: 10.1111/bjh.16221 7. World Health Organization. Anaemia. Accessed January 19, 2023. https://who.int/health-topics/anaemia 8. Smith C, Teng F, Branch E, Chu S, Joseph KS. Maternal and perinatal morbidity and mortality associated with anemia in pregnancy. Obstet Gynecol 2019;134:1234–44. doi: 10.1097/AOG.0000000000003557 9. Jefferds MED, Mei Z, Addo Y, Hamner HC, Perrine CG, Flores-Ayala R, et al. Iron deficiency in the United States: limitations in guidelines, data, and monitoring of disparities. Am J Public Health 2022;112:S826–35. doi: 10.2105/AJPH.2022.306998 10. Siu AL. Screening for iron deficiency anemia and iron supplementation in pregnant women to improve maternal health and birth outcomes: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2015;163:529–36. doi: 10.7326/M15-1707 12. Hamm RF, Wang EY, Levine LD, Srinivas SK. Association between race and hemoglobin at delivery or need for transfusion when using race-based definitions for treatment of antepartum anemia. Obstet Gynecol 2021;138:108–10. doi: 10.1097/AOG.0000000000004439 13. Marcewicz LH, Anderson BL, Byams VR, Grant AM, Schulkin J. Screening and treatment for iron deficiency anemia in women: results of a survey of obstetrician-gynecologists. Matern Child Health J 2017;21:1627–33. doi: 10.1007/s10995-016-2252-1 14. Ford CL, Airhihenbuwa CO. The public health critical race methodology: praxis for antiracism research. Soc Sci Med. 2010;71:1390–8. doi: 10.1016/j.socscimed.2010.07.030 15. Alson JG, Robinson WR, Pittman L, Doll KM. Incorporating measures of structural racism into population studies of reproductive health in the United States: a narrative review. Health Equity 2021;5:49–58. doi: 10.1089/heq.2020.0081 16. Braveman PA, Arkin E, Proctor D, Kauh T, Holm N. Systemic and structural racism: definitions, examples, health damages, and approaches to dismantling. Health Aff (Millwood) 2022;41:171–8. doi: 10.1377/hlthaff.2021.01394 17. Mersha TB, Abebe T. Self-reported race/ethnicity in the age of genomic research: its potential impact on understanding health disparities. Hum Genomics 2015;9:1. doi: 10.1186/s40246-014-0023-x 18. Johnson JD, Louis JM. Does race or ethnicity play a role in the origin, pathophysiology, and outcomes of preeclampsia? An expert review of the literature. Am J Obstet Gynecol 2022;226:S876–85. doi: 10.1016/j.ajog.2020.07.038 19. Scott KA, Britton L, McLemore MR. The ethics of perinatal care for Black women: dismantling the structural racism in “mother blame” narratives. J Perinatal Neonatal Nurs 2019;33:108–15. doi: 10.1097/JPN.0000000000000394 20. Smedley A, Smedley BD. Race as biology is fiction, racism as a social problem is real: anthropological and historical perspectives on the social construction of race. Am Psychol 2005;60:16–26. doi: 10.1037/0003-066X.60.1.16 21. Borrell LN, Echeverria SE. The use of Latinx in public health research when referencing Hispanic or Latino populations. Soc Sci Med 2022;302:114977. doi: 10.1016/j.socscimed.2022.114977 22. Wall-Wieler E, Bane S, Lee HC, Carmichael SL. Severe maternal morbidity among US- and foreign-born Asian and Pacific Islander women in California. Ann Epidemiol 2020;52:60–3.e2. doi: 10.1016/j.annepidem.2020.07.016 23. Baumeister L, Marchi K, Pearl M, Williams R, Braveman P. The validity of information on “race” and “Hispanic ethnicity” in California birth certificate data. Health Serv Res 2000;35:869–83. 24. Centers for Disease Control and Prevention.Severe maternal morbidity in the United States. Accessed January 21, 2023. https://cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html 25. Anemia in pregnancy. ACOG Practice Bulletin No. 233. American College of Obstetricians and Gynecologists. Obstet Gynecol 2021;138:e55–64. doi: 10.1097/AOG.0000000000004477 26. Leonard SA, Kennedy CJ, Carmichael SL, Lyell DJ, Main EK. An expanded obstetric comorbidity scoring system for predicting severe maternal morbidity. Obstet Gynecol 2020;136:440–9. doi: 10.1097/AOG.0000000000004022 27. Snyder AB, Lane PA, Zhou M, Paulukonis ST, Hulihan MM. The accuracy of hospital ICD-9-CM codes for determining sickle cell disease genotype. J Rare Dis Res Treat 2017;2:39–45. doi: 10.29245/2572-9411/2017/4.1124 28. Sharma AJ, Ford ND, Bulkley JE, Jenkins LM, Vesco KK, Williams AM. Use of the electronic health record to assess prevalence of anemia and iron deficiency in pregnancy. J Nutr 2021;151:3588–95. doi: 10.1093/jn/nxab254 29. Shi H, Chen L, Wang Y, Sun M, Guo Y, Ma S, et al. Severity of anemia during pregnancy and adverse maternal and fetal outcomes. JAMA Netw Open 2022;5:e2147046. doi: 10.1001/jamanetworkopen.2021.47046 30. Beckert RH, Baer RJ, Anderson JG, Jelliffe-Pawlowski LL, Rogers EE. Maternal anemia and pregnancy outcomes: a population-based study. J Perinatol 2019;39:911–9. doi: 10.1038/s41372-019-0375-0 31. Crear-Perry J, Correa-de-Araujo R, Lewis Johnson T, McLemore MR, Neilson E, Wallace M. Social and structural determinants of health inequities in maternal health. J Womens Health 2021;30:230–35. doi: 10.1089/jwh.2020.8882 32. Rothman KJ, Greenland S, Lash TL. Modern epidemiology. Lippincott Williams & Wilkins; 2008. 33. Richiardi L, Bellocco R, Zugna D. Mediation analysis in epidemiology: methods, interpretation and bias. Int J Epidemiol 2013;42:1511–9. doi: 10.1093/ije/dyt127 34. Kanu FA, Hamner HC, Scanlon KS, Sharma AJ. Anemia among pregnant women participating in the Special Supplemental Nutrition Program for Women, Infants, and Children–United States, 2008–2018. MMWR Morb Mortal Wkly Rep 2022;71:813–9. doi: 10.15585/mmwr.mm7125a1 35. Petraglia F, Dolmans MM. Iron deficiency anemia: impact on women's reproductive health. Fertil Steril 2022;118:605–6. doi: 10.1016/j.fertnstert.2022.08.850 36. Odoms-Young AM, Bruce MA. Examining the impact of structural racism on food insecurity: implications for addressing racial/ethnic disparities. Fam Community Health 2018;41:S3–6. doi: 10.1097/FCH.0000000000000183 37. Mei Z, Cogswell ME, Looker AC, Pfeiffer CM, Cusick SE, Lacher DA, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1999–2006. Am J Clin Nutr 2011;93:1312–20. doi: 10.3945/ajcn.110.007195 38. Le CHH. The prevalence of anemia and moderate-severe anemia in the US population (NHANES 2003-2012). PLoS One 2016;11:e0166635. doi: 10.1371/journal.pone.0166635 39. Dennard E, Kristjansson E, Tchangalova N, Totton S, Winham D, O'Connor A. Food insecurity among African Americans in the United States: a scoping review. PLoS One 2022;17:e0274434. doi: 10.1371/journal.pone.0274434 40. Chambers BD, Arabia SE, Arega HA, Altman MR, Berkowitz R, Feuer SK, et al. Exposures to structural racism and racial discrimination among pregnant and early post-partum Black women living in Oakland, California. Stress Health 2020;36:213–9. doi: 10.1002/smi.2922 41. Detlefs SE, Jochum MD, Salmanian B, McKinney JR, Aagaard KM. The impact of response to iron therapy on maternal and neonatal outcomes among pregnant women with anemia. Am J Obstet Gynecol MFM 2022;4:100569. doi: 10.1016/j.ajogmf.2022.100569 42. Auerbach M, Georgieff MK. Guidelines for iron deficiency in pregnancy: hope abounds. Br J Haematol 2020;188:814–6. doi: 10.1111/bjh.16220 43. Gyamfi-Bannerman C, Srinivas SK, Wright JD, Goffman D, Siddiq Z, D'Alton ME, et al. Postpartum hemorrhage outcomes and race. Am J Obstet Gynecol 2018;219:185.e1–10. doi: 10.1016/j.ajog.2018.04.052 44. Hailu EM, Maddali SR, Snowden JM, Carmichael SL, Mujahid MS. Structural racism and adverse maternal health outcomes: a systematic review. Health Place 2022;78:102923. doi: 10.1016/j.healthplace.2022.102923 45. Jeffers NK, Berger BO, Marea CX, Gemmill A. Investigating the impact of structural racism on Black birthing people: associations between racialized economic segregation, incarceration inequality, and severe maternal morbidity. Soc Sci Med 2023;317:115622. doi: 10.1016/j.socscimed.2022.115622 46. Heck KE, Parker JD, McKendry CJ, Schoendorf KC. Multiple-race mothers on the California birth certificate, 2000. Ethn Dis 2001;11:626–32. 47. Association of Anaesthetists. Gestational anaemia and severe acute maternal morbidity: a population‐based study. Accessed January 21, 2023. https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.15222 48. Owens DC, Fett SM. Black maternal and infant health: historical legacies of slavery. Am J Public Health 2019;109:1342–5. doi: 10.2105/AJPH.2019.305243 49. Teichman J, Nisenbaum R, Lausman A, Sholzberg M. Suboptimal iron deficiency screening in pregnancy and the impact of socioeconomic status in a high-resource setting. Blood Adv 2021;5:4666–73. doi: 10.1182/bloodadvances.2021004352 50. Smith KL, Shipchandler F, Kudumu M, Davies-Balch S, Leonard SA. “Ignored and invisible”: perspectives from Black women, clinicians, and community-based organizations for reducing preterm birth. Matern Child Health J 2022;26:726–35. doi: 10.1007/s10995-021-03367-1 51. Zakai NA, McClure LA, Prineas R, Howard G, McClellan W, Holmes CE, et al. Correlates of anemia in American Blacks and Whites: the REGARDS renal ancillary study. Am J Epidemiol 2008;169:355–64. doi: 10.1093/aje/kwn355 52. Golden B, Asiodu IV, Franck LS, Ofori-Parku CY, Suárez-Baquero DFM, Youngston T, et al. Emerging approaches to redressing multi-level racism and reproductive health disparities. NPJ Digit Med 2022;5:169. doi: 10.1038/s41746-022-00718-2 Figure
Figure
Comments (0)