Branch retinal vein occlusion in a case of recalcitrant diffuse anterior scleritis treated with tofacitinib
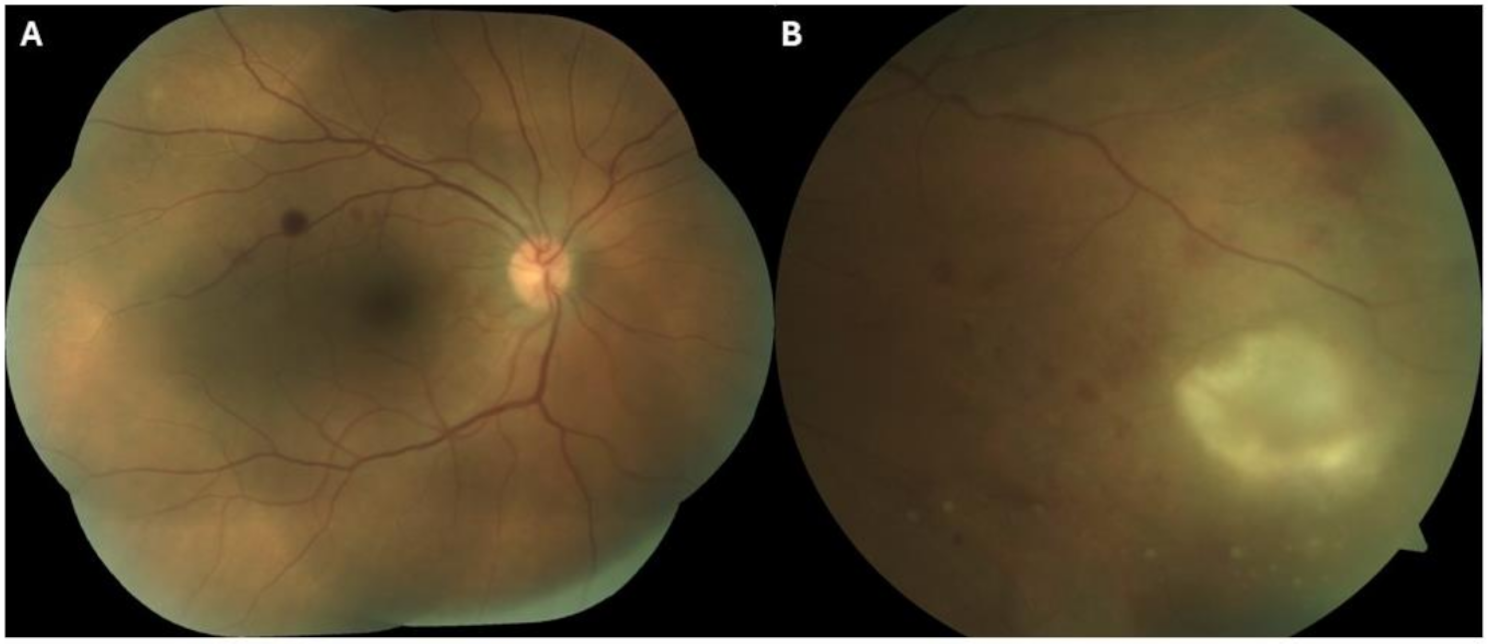
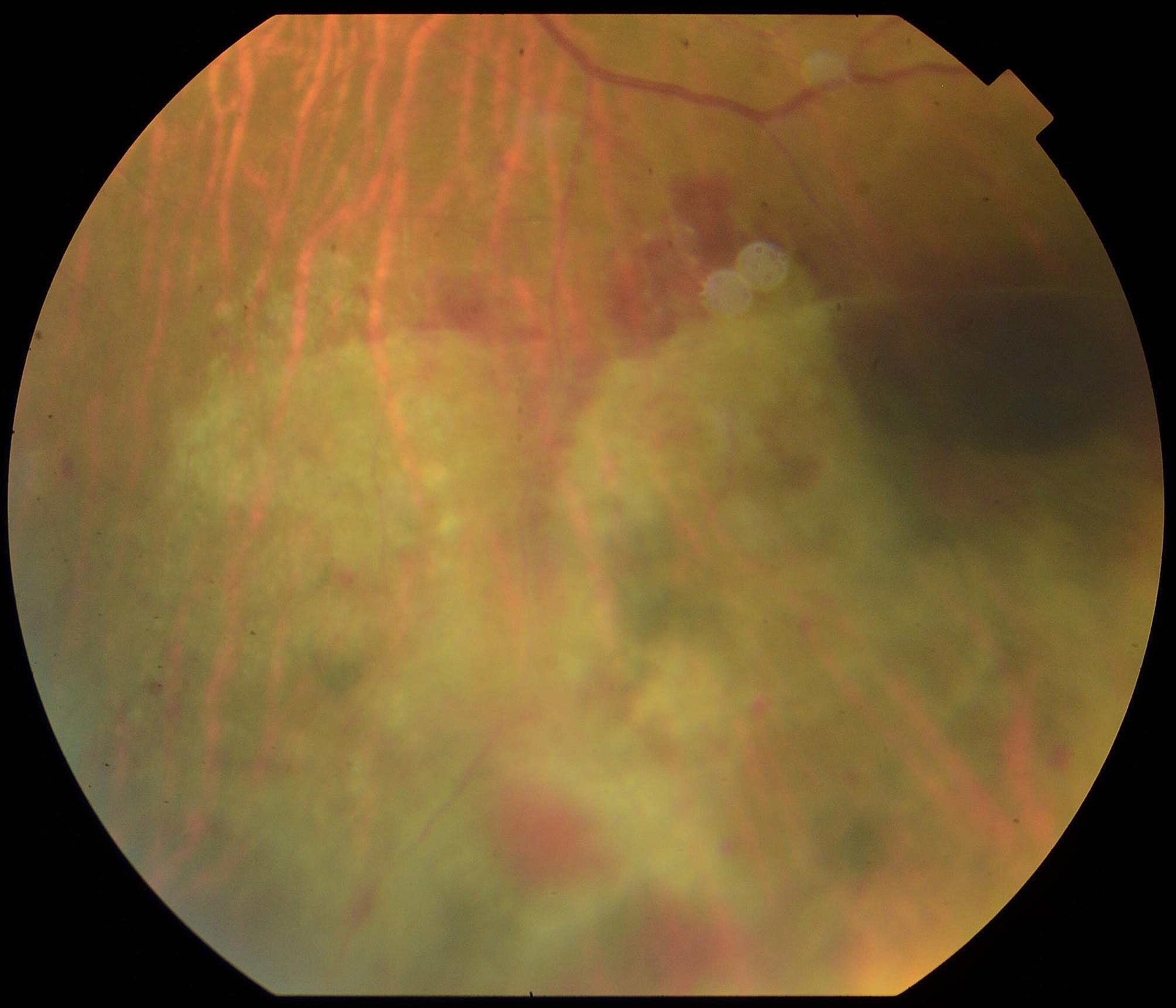
Tofacitinib, an oral small-molecule Janus kinase inhibitor, has been reported by several authors, including our group, to be effective in treating scleritis at a dosage of 5 mg twice daily [1,2,3]. The drug has been approved by US Food and Drug Administration (FDA) for the treatment of rheumatoid arthritis (RA), psoriatic arthritis, and ulcerative colitis. Our patient was started on oral tofacitinib before using conventional immunosuppressives. Several studies have highlighted the effectiveness of tofacitinib as monotherapy, and there has been an increasing trend in the use of the drug in the management of RA in recent years [4]. However, the FDA has issued a warning about the increased risk of blood clots and death in patients with rheumatoid arthritis who were treated with a 10 mg twice-daily dose of tofacitinib. This warning was based on interim data from an ongoing safety study that showed a higher risk of pulmonary embolism and overall mortality in patients receiving the higher dose compared to those receiving a TNF inhibitor [5]. The risk was found to be higher in patients over 50 years old, with a history of cardiovascular disease, or receiving high doses of corticosteroids [6]. Patients with pre-existing thromboembolic risk factors, such as those on prothrombotic or antithrombotic treatments, were also found to be at increased risk of thromboembolic episodes with the use of tofacitinib [7]. Also, long-standing inflammatory systemic disorders, increased age, and traditional cardiovascular risk factors such as obesity, diabetes, hypertension, hyperlipidemia, and smoking, further increased the risk of thrombosis [8]. Other adverse events associated with the use of tofacitinib include increased risk of herpes zoster infection, [9] reactivation of tuberculosis, [10] malignancy, [11] increased levels of liver transaminases, and serum lipid derangements [12]. The index case presented with diffuse active scleral inflammation, along with a history of rheumatoid arthritis and systemic hypertension. Given the severity of the inflammation, its resistance to systemic corticosteroid treatment, and the patient’s underlying systemic disease, both a rheumatologist and ophthalmologist decided to begin tofacitinib therapy. Tofacitinib has been found to be helpful in the management of treatment-resistant cases of scleritis [1,2,3]. At our setup, the drug is often preferred over the TNF-alpha agents, particularly by the patients, as it is cheaper and available as oral formulation. The tofacitinib therapy was successful in resolving the scleral inflammation, but unfortunately, the patient developed superior-temporal BRVO. It is difficult to determine the exact cause of this event, particularly given the presence of systemic hypertension in the patient. However, it is worth noting that the patient was receiving regular medical care and was closely monitored by an internist. Nevertheless, the potential risk of ocular thromboembolic events must be considered when initiating tofacitinib therapy, particularly in patients with systemic comorbidities.





Comments (0)