
Remember me





In this study, we analyzed the predicted volume of interosseous interference between the proximal and distal segments of the osteotomized mandible before surgery. Using the 3D information of the predicted bony interference by occlusion-based surgical simulation, the bony interference could be clearly defined. The purpose of this study was to address the following questions: (1) which side shows more interosseous interference? and (2) what is the major influencing factor for interosseous interference in SSRO for asymmetric mandibular prognathism? To answer the key questions, we investigated (1) the pattern and volume of interosseous interference according to the groups and (2) the predictor variable that affected the volume of osseous interference.
The results of the current study showed the following: (1) the anticipated interosseous interference was more frequently noted on the contralateral side of deviation (long side) than the deviated site (short side). However, osseous interference could be existed on any side, unilaterally or bilaterally. (2) Amount of Me deviation and the degree of ramal inclination significantly influenced the predicted 3D volume of bony collision. Age, sex, amount of setback at Pog, or side (long vs short) was excluded from influencing factor to interference volume.
The interbony interference can directly cause changes in the condylar position and influence the temporomandibular function and long-term stability. Bony interference can occur not only in the horizontal but also in the vertical plane, particularly when the mandibular distal segment is mobilized with yaw, roll, or pitch rotation. In general, the more the chin deviation, the greater the amount of bone interference. Our result indicated that the amount of interference was larger on the long side (177.7 ± 348.4 mm3) than on the short side (54.4 ± 124.4 mm3). Furthermore, the contralateral side of deviation (long side) showed a narrower ramal inclination than the deviated side (short side), and the amount of asymmetry was proportional to the difference in the volume of bone interference. Simultaneously, the bilateral differences in ramal inclination were significantly correlated with the volume of bone interference. The results suggest that on the side with more mandibular setbacks (long side), more interferences can be anticipated and need to be considered before surgery. We investigated the side with greater interference volume. In the case of severe asymmetry (group 3), there was more interference on the long side (n = 29) than on the short side (n = 21). These findings indicated that even though it can be anticipated that there would be more interference on the long side, the short side also can have interosseous interferences. This means that osseous interference could be existed on any side, unilaterally or bilaterally in patients with or without asymmetry.
We usually perform CASS based on the simulated postoperative occlusion and intercuspation; distal mandibular segments would be mobilized in various directions. Only the 3D-simulated image can be seen after finishing the occlusion-based segment mobilization, which is a complex spatial movement. Therefore, it cannot be the same as a 2-dimensional prediction from posteroanterior cephalometry. Different types of set-up occlusion can result in different sites of bony interference or gap (Fig. 7). The site and volume of interosseous interference could be determined by the complex direction and amount of yaw or roll rotation of the distal segment according to the planned occlusion and skeletal position change. Therefore, preoperative 3D surgical simulation is important to minimize osseous interference and successfully control the bony collision. Our results indicated that 3D interference needs to be individually analyzed and surgical modification be the patient-specific condition.
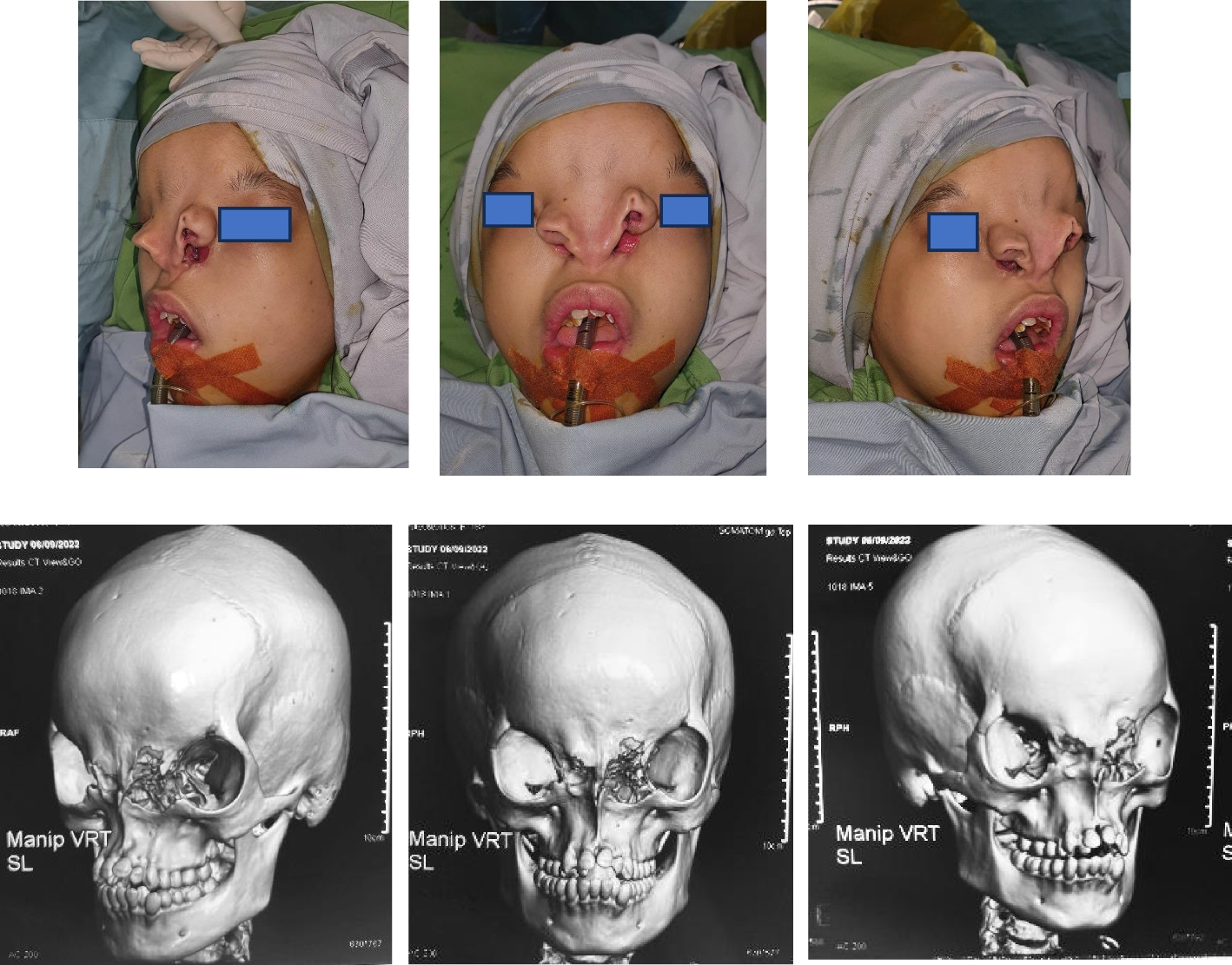
Fig. 7
Different setup occlusion can result in different sites of interference or gap. The severity or location of interosseous interference is determined by the transverse or rotational movement of the mandibular distal segment according to the planned occlusion and skeletal position. A Preoperative occlusion and skeletal position in a patient with mandibular deviation to the right side. B Simulation #1, 3D simulation based on a planned occlusion resulted in interosseous interference on the right side and a gap on the left side. C Simulation #2, another set-up occlusion shows interosseous interference on the left side and a gap on the right side
Various efforts have been made to reduce the bony interference between the proximal and distal bone segments. SSRO modification was suggested by changing the cutting design [13, 17,18,19], resection of interfering bony part (or mandibular angle) in proximal segments [20], or intentional posterior ostectomy of the distal segment had been added after the sagittal splitting [13, 21]. When severe interference was anticipated, secondary lingual osteotomy was recommended [5, 15, 22]. In a previous study, maxillary surgery was added to mobilize the mandibular distal segment-maxilla complex simultaneously to minimize the mandibular proximal–distal segment interference [6].
If we can establish a threshold (cutoff value) for the level of interference, it would be helpful to decide to add a specific surgical approach if the projected volumetric interference surpasses a specific threshold. However, it was difficult to establish such a cutoff value or threshold to select the specific surgical technique because the volume of interference was not directly correlated with the real severity of interference at the operation theater. For example, even though there were similar degrees of asymmetry, some patient shows a large volume of interference at the anterior-lingual region of proximal segments that can be removed by simple grinding. However, another patient shows a narrow but deep bony collision at the posterior part of the distal segment, which can be managed by lingual osteotomy.
In our institution, the aforementioned techniques are currently used in the operation room to eliminate the premature contact of the segments that interferes with passive segment adaptation. If the volume of interference is not significant, grinding the lingual side of the proximal segment is usually enough. However, if severe interference is present, posterior ostectomy or lingual osteotomy is accompanied during the SSRO surgery. Previous reports also showed that the prediction of premature bony contact or interosseous interference can be efficiently simulated from the CASS and is beneficial for surgeons [5, 6]. Ramal inclination can be intentionally changed for esthetic purposes in our clinic. For example, ramal inclination at the short side is wider than the long side before surgery. Furthermore, ramal inclination on the short side needs to be adjusted and narrowed to match similar to the long side. Therefore, intentional change in ramal inclination change is necessary for asymmetry patients. Oriental patients usually want a slender facial shape rather than a square shape. Hence, they prefer narrowing the ramal inclination rather than maintaining the original ramal inclination after SSRO. For functional and esthetic purposes, the elimination of osseous interference and ramal inclination change would increase patient satisfaction.
Our results indicated that the transverse Me position was stable after significant narrowing of the bilateral ramal angle after the surgery. Not only the symmetry group but also the asymmetry group showed a significant reduction in ramal inclination, and the ramal inclination was maintained during the postoperative follow-up period (ΔT2–T1). Although there were significant anteroposterior relapses, the amount was nearly 1 mm, which is not greater than in previous reports [23, 24].
Using CASS, accurate diagnosis can be obtained for the surgery which can improve patient safety and the outcomes [10]. The 3D simulation also facilitates the virtual splitting of the skull into separate segments and 3D movements of bone segments to determine the final position of the separated mandibular segment [25].
To the best of our knowledge, this is the first study to quantify the volume of interference and investigated the influencing factor to osseous interference. We could collect data on interosseous interference through subtraction of proximal and distal osteotomized segments using Boolean operation in the computer software. This method would also be useful for analyzing the anticipated segment collision in any type of orthognathic surgery.
This study and other previous studies had limitations that need to be acknowledged. In general, the actual osteotomy in the operation room is not the same as the 3D virtual osteotomy in the CASS. Thus, although it does not influence the outcomes, the osteotomized segment would be different from virtual planning. Valls-Ontanon (2020) reported that 3D CASS was sensitive (100%) but showed low specificity (51.6%) in predicting proximal and distal segment interferences [5]. Further development of CASS needs to proceed to implement more precise and predictable 3D virtual planning. In this study, we did not experience TMJ disorder or significant functional problems after changing the ramal inclination in our patients. However, a detailed clinical examination was not conducted in this study. Further study is needed to clarify this issue.
Comments (0)