
Remember me







Pelvic sacroiliac complex fractures are mostly caused by high-energy trauma, mostly in motor vehicle accidents. The percutaneous surgical approach is a popular method for restoring the pelvic anatomy and securing rigid fixation. Both IS and TITS screw fixation are excellent percutaneous fixation methods for surgical stabilization. However, due to the complexity of the sacroiliac structure, accurate screw placement with minimal soft-tissue dissection is highly technically demanding. Our study showed that a percutaneous approach provided rigid internal fixation with good reduction quality and clinical outcomes. However, there was a potential high risk for screw malposition while inserting the TITS screws. In addition, patients with larger PI values were found to be at significantly higher risk for TITS screw malposition.
Accurate screw placement remains of paramount importance, as it is related to pelvic construct stability and optimal outcomes. The screw malposition rate varies over a wide range (0–58.8%) in the published literature [24,25,26,27]. Our study demonstrated a malposition rate of 3.07% and 22.86% in the IS and TITS screw groups, respectively. Even though our results were comparable with previous studies, the high malposition rates raised concerns about neurovascular injury and needed to be addressed.
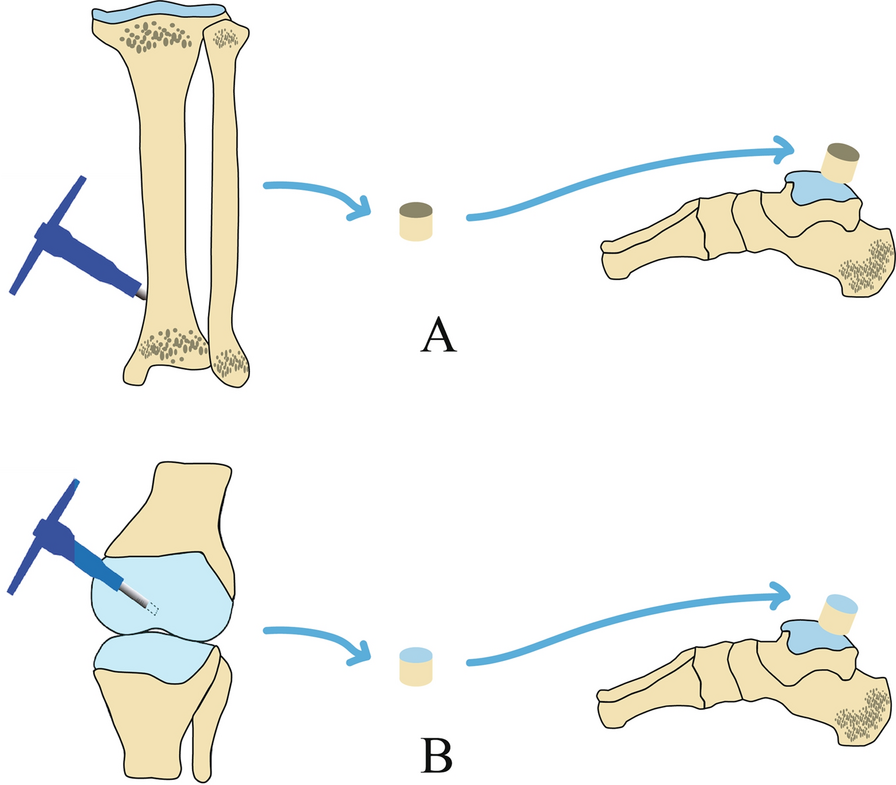
After analyzing the associated radiographic parameters, we found that the values of PI had a significant influence on the screw malposition rate in TITS screw fixation patients. In the IS screw fixation group, a 0% screw perforation rate was observed in patients with smaller PI values, compared to 8.33% in patients with larger PI values (p = 0.133). Interestingly, in the TITS screw group, the screw malposition rate was significantly lower in patients with smaller PI values (13.51%) when compared to those with larger PI values (33.33%; p = 0.049). This result can be explained by the difficult positioning of an intraoperative fluoroscope to obtain clear visualization of pelvic inlet and outlet projections in said patients. In general, in order to acquire good-quality images of inlet and outlet projections, the central ray projects at an angle 45° cephalic and 45° caudal to best demonstrate the pelvic ring configuration, and the projection angle might require minor adjustment to account for anatomical variations among individuals in order to optimize surgical outcomes. Ricci et al. found that, to achieve the intraoperative visualization of special bone corridors, an average caudal tilt of 21° of inlet angle was needed to profile the S1 anterior body; meanwhile, the average cephalad tilt outlet angle was 63° perpendicular to the S1 vertebral body and 57° for the S2 level [28]. Typically, patients with larger PI values require a greater cephalad tilt of the fluoroscope. With a horizontal fluoroscope placement, a clear pelvic outlet image can be obtained with the superimposed anterior and posterior rings of the first and second sacrum segments. The optimal images were often difficult to acquire when the fluoroscope trajectory was hindered or blocked by excess fatty tissue in the abdomen or thighs. Therefore, the inability to steer the fluoroscope to achieve an appropriate angle of trajectory might lead to a higher frequency of malpositioned TITS screws in patients with larger PI values (Fig. 1).
Fig. 1
A With larger PI values, a greater fluoroscope cephalad tilt and a more horizontal projector placement were required. However, it was difficult to steer the fluoroscope to an appropriate angle of trajectory to get an optimal and clear pelvic outlet image due to hindrance from the radiolucent table or the patient’s thigh. When setting the pelvic inlet projection, the beamer of the single-arm fluoroscopic intensifier had to be aligned more perpendicularly with respect to the patient. The radiation could pass through excessive abdominal and buttock fat and bowel flatus, which could further interfere with and degrade the resolution of the images. B With smaller PI values, it is easier to position the fluoroscope to project the appropriate cephalad and caudal tilt angles. Solid ine caudad tilt of the fluoroscope, dashed line cephalad tilt of the fluoroscope, dotted line ideal cephalad tilt of the fluoroscope, dashed-dotted line PI angle, PI pelvic incidence
The PI was defined as the angle between the line perpendicular to the sacral endplate at its midpoint and the line connecting this point to the center of the femoral heads [10, 29]. In a given individual, this value remains constant after puberty and unchanged in any posture [30]. Moreover, PI values show a wide distribution range in the normal population. Abola et al. reported that a larger PI value was significantly correlated with a highly angulated and curved sacrum and corresponded to a more linear sacroiliac joint and narrower sacral alae in the sagittal plane [31]. Coudert et al. also described a similar finding in the horizontal plane and found that the articular surface orientation of the sacroiliac joint had a significant correlation with the PI value [32]. In our study, patients with larger PI values were found to have a significantly increased risk of screw malposition in the TITS screw group (p = 0.049), with logistic regression analysis also confirming that larger PI values were a significant risk factor in the TITS group (p = 0.010). We found that, even with an oblique osseous pathway of the sacral isthmus when inserting the IS screw, the surgeon was able to modify the screw trajectory while determining the safety zone and to make it slightly deviate from being perpendicular to the sacroiliac joint. This resulted in fewer patients with screw malposition.
Sacral dysmorphism is a common anatomical variant, which was first characterized as collinearity, mammillary processes, noncircular and misshapen anterior first sacral neuroforamina, and residual S1/S2 disc space by Routt et al. on plain radiographs [14]. In addition, Kaiser et al. used quantitative characteristics to define sacral dysmorphism, including coronal and axial angulation of the first sacral osseous corridor and the anatomic variation of the sacrum that prevents safe trans-sacral screw placement [16]. In our study, sacral dysmorphism was identified in 31.11% of patients, and we observed that it was significantly more common in patients with smaller PI values in both the IS and TITS screw fixation groups (p = 0.027 and 0.003, respectively). When sacral dysmorphism is present, an oblique and angulated trajectory makes screw placement difficult and demanding, even for experienced surgeons. However, no correlation was found between sacral dysmorphism and screw malposition rate in our study. This lack of correlation can be explained by the frequent insertion of IS screws at the level of the first sacral segment S1 (96.92%) in our study, while TITS screws were often placed at the level of the second sacral segment, S2 (74.29%). In the preoperative planning of IS screw placement, it was easier to modify the screw trajectory angle at the upper sacral segment in patients with sacral dysmorphism. Moreover, the second sacral segment was less influenced by the sacral dysmorphism, which should be considered when aiming for safe TITS screw placement.
Considering the close proximity of several neurovascular structures, the potential risk of neurovascular bundle damage due to screw malposition is a major concern in IS and TITS screw osteosynthesis procedures. Published studies have reported neurovascular complication rates ranging from 0% to 3.2% [25, 26, 33]. The exiting sacral nerve roots, descending lumbar nerve roots, as well as the iliac vessels and their distal branches are all critical structures that should be recognized to avoid any iatrogenic injury. Regarding the concerns about screw malposition, there is limited literature available that addresses specific scenarios in which screw removal or revision surgery is valid. Remiger et al. did not report screw removal in their cases [34], while Routt et al. suggested that removal should only be performed in cases of screw breakage or dislodgement [9]. A review from Yücel et al. highlighted that removal may be reasonable in patients with an infection or persistent local pain or neurological symptoms caused by screw malposition [35]. In our study, despite the screw malposition rates of 3.07% and 22.86% in the IS and TITS screw groups, respectively, no perioperative vascular injuries were detected, and none of the patients reported experiencing any post-operative neurological symptoms or deficits. The only patient who underwent revision surgery had a concurrent brain injury, which hindered the comprehensive assessment of post-operative neurologic function. Therefore, we decided to remove the malpositioned screw during debridement surgery for wound dehiscence in the hope of preventing potential undiagnosed neurological conditions.
Whether to perform reduction with precise and quick percutaneous screw placement with the patient in the supine or prone position is still under debate. Initially, IS and TITS screw fixation procedures were performed with the patient in the prone position, but in 1992 Routt et al. introduced the use of the supine position when performing the surgery [36]. The prone position allowed the surgeons to focus on the posterior pelvic sacroiliac complex fracture. However, that position had some limitations, as the pelvic deformity could be accentuated by gravity, which could make reduction more difficult. Second, it could induce an increase in intra-abdominal pressure as a consequence of the prone positioning [37, 38]. In contrast, performing the surgery in the supine position had several advantages in terms of the pelvic ring and hemodynamic stability. Moreover, to ensure a smooth workflow, the supine position allowed surgeons to simultaneously perform other procedures for other concomitant injuries, such as intra-abdominal/genitourinary organ injuries or limb fractures, without changing position and re-draping the surgical fields. In our study, 74.81% of patients underwent the surgery in the supine position (70.77% and 78.57% in the IS and TITS screw groups, respectively). In the supine position, when setting the pelvic inlet projection, the beamer of the single-arm fluoroscopic intensifier had to be aligned more perpendicularly with respect to the patient for larger PI values, and this could result in the radiation passing through excessive abdominal fat and bowel flatus, which could interfere with and degrade the resolution of the images. This interference may make large PI values a risk factor for screw malposition (Fig. 1).
Our work had some limitations. First, the study design was a single-center, retrospective study with two groups, which were then divided into four sub-groups with small and unequal sample sizes, and this may have compromised the generalizability of our results. Second, all the procedures were performed by a single surgeon. With an improvement in surgical performance over time, a decrease in the screw malposition rate could be expected, which could affect surgical outcomes. Despite these inherent limitations, our work has important implications for surgeons performing TITS screw fixation in patients with large PI values, as preoperative surgical planning is paramount when attempting to reduce screw malposition and potential neurovascular complications (Fig 2).
Fig. 2
A TITS screw placement at the S2 level was successfully executed along the intended projection. B, C A TITS screw placed at the S2 level was found to be malpositioned within the spinal canal. TITS trans-iliac trans-sacral
Comments (0)