
Remember me


The prevalence of hypertensive disorders of pregnancy is increasing, and they complicate up to 8% of pregnancies.1 These disorders are associated with long-term cardiovascular disease and are the leading cause of postpartum readmission.1,2 Hypertensive disorders of pregnancy contribute to 7.1% of all maternal deaths in the United States.3 Postpartum stroke is the leading cause of mortality related to hypertensive disorders of pregnancy and is at its maximum risk within 10 days of discharge after delivery.4 The American College of Obstetricians and Gynecologists (ACOG), therefore, recommends that patients with hypertensive disorders of pregnancy present for a blood pressure check within 7–10 days postpartum, which is traditionally performed in-person at the office where patients received obstetric care.5 Despite this recommendation, it has been estimated that up to 70% of patients do not present for follow-up.6
Telehealth is a promising intervention that has been shown to improve patient satisfaction without compromising the patient–physician relationship.7 Evidence suggests remote blood pressure monitoring may be a feasible, cost-effective strategy for managing postpartum hypertension.8,9 We tested the hypothesis that remote blood pressure monitoring would increase the rates at which postpartum patients would record their blood pressure shortly after hospital discharge.
METHODSThis multisite randomized controlled trial was approved by the Prisma Health IRB with IRB reliance for the other site and was conducted between April 2021 and September 2021 at two academic training institutions. Patients were eligible for inclusion if they were postpartum and were diagnosed with gestational hypertension, preeclampsia, or chronic hypertension with superimposed preeclampsia in the antenatal or immediate postpartum period of the delivery admission. Diagnoses were made using ACOG criteria.1 Patients were excluded from participation if they were younger than age 18 years, did not speak English, had body mass indexes (BMIs, calculated as weight in kilograms divided by height in meters squared) of 50 or higher, or did not have a phone with unlimited texting capability or the ability to receive calls. Patients with BMIs of 50 or higher were excluded to ensure accuracy of patient-acquired blood pressure measurements.
Members of the research team approached eligible patients on the postpartum floor. For patients who agreed to participate, the team obtained written informed consent and block randomization was performed using REDCap. Patients were randomized to an in-person outpatient blood pressure check within 10 days of discharge or remote blood pressure monitoring using a home blood pressure cuff and smartphone application (app). Patients in the clinic-based follow-up group were given the date and time of their appointment at time of discharge; patients assigned to remote monitoring were provided with an appropriately sized home blood pressure cuff and instructed on proper use for accurate measurements. Patients downloaded and installed the smartphone app on their personal cell phone. They were instructed to take their blood pressure daily and educated on how to manually input their blood pressure within the app. All blood pressures documented within the app were automatically uploaded to a secure web-based platform for remote review by designated physicians at each site.
The study team designed a blood pressure triage protocol after input from health care professionals caring for postpartum patients and nursing leadership at each clinical site (Appendix 1, available online at https://links.lww.com/AOG/D317). If patients documented an elevated blood pressure (140 or higher/90 or higher), they received a text-based survey to assess for symptoms of visual changes, right upper quadrant pain, or headache. A 24/7 on-call operator employed by the remote blood pressure monitoring service contacted patients if they did not respond to the survey, reported clinical symptoms that could be consistent with preeclampsia with severe features, or reported a second blood pressure measurement 160 or higher/100 or higher. Although 160 or higher/110 or higher is the accepted range for a severe blood pressure, a diastolic blood pressure of 100 or higher was chosen after discussion with nonresearch clinical staff and concern for patient safety with use of a higher threshold with remote monitoring. If patients reported clinical symptoms or blood pressure 160 or higher/100 or higher, they were instructed to present to the labor and delivery obstetric triage unit at each site for further evaluation. The on-call operator was not responsible for further assessment or provision of medical advice. Otherwise, their blood pressures were reviewed daily by the assigned physicians on the secure web-based platform. If patients had persistent blood pressures of 150 or higher/100 or higher, they were individually contacted by a physician and either initiated or up-titrated on antihypertensive medication as outlined in the blood pressure triage protocol. Remote monitoring of patient blood pressures continued for 16 days postdischarge, after which patients could no longer enter measurements into the app. All patients received a survey by email 16 days after discharge to assess their attitude toward and comfort with remote blood pressure monitoring. Patients enrolled in remote monitoring had additional survey questions related to their use of the blood pressure cuff and smartphone software. If patients did not respond, they received a single reminder email after 7 days.
The primary outcome of this study was the ascertainment of any blood pressure within 10 days postpartum. Patients assigned to remote monitoring were considered to have satisfied the primary outcome even if their qualifying blood pressure was attained in-person, but after discharge. Secondary outcomes included rates of initiation or up titration of antihypertensive medications, unscheduled outpatient or obstetric triage visits for hypertension, readmission for hypertension, and attending standard postpartum follow-up 6–8 weeks after delivery. A univariate subanalysis was performed comparing the difference in the primary outcome among different races and ethnicities.
We calculated a sample size using previously published data from a study by Hirshberg et al10 that used text-based remote blood pressure monitoring. In their cohort, a blood pressure was obtained within 10 days of discharge in 43.7% of patients who were undergoing usual care and in 92.2% of patients who were using text-based monitoring. Using an estimate of a 50% rate of blood pressure ascertainment with usual care and a more conservative estimate of 70% with remote monitoring, as well as a two-sided alpha of 5% and 80% power to detect a 20% difference in the primary outcome between groups, we calculated a total sample size of 186, with 93 patients per arm.
Statistical analysis was performed using STATA 16. Continuous variables were assessed for normality using the Shapiro-Wilk test. All continuous variables demonstrated a nonparametric distribution, and the Wilcoxon rank sum test was, thus, used for comparison. Categorical variables were compared using the χ2 test or Fisher exact test, as appropriate. Demographic data were patient-reported as documented in the medical record. Race was purposefully included because Black patients experience higher morbidity and mortality related to hypertensive disorders of pregnancy, and our hope was that remote monitoring could improve outcomes for this group of pregnant people.
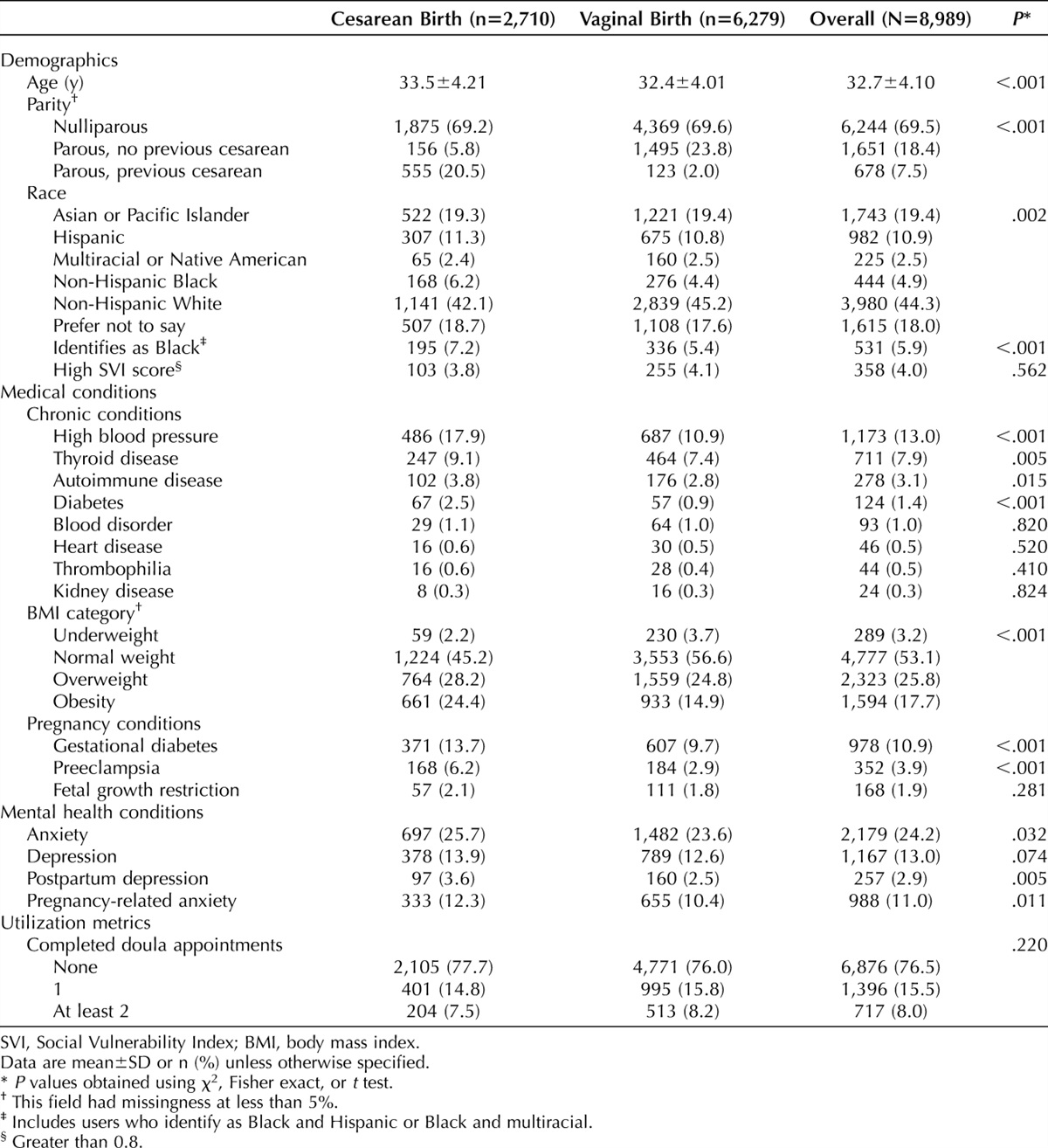
RESULTSOf the 273 postpartum patients approached for enrollment in the study, 71 declined to participate, four withdrew consent after randomization, and one was deemed ineligible after study completion due to being misclassified as having a diagnosis of a hypertensive disorder of pregnancy. The final study population included 197 patients, with 101 in the office-based monitoring group and 96 in the remote monitoring group (Fig. 1). The study arms were balanced, with no differences in baseline (Table 1) or prehospital discharge obstetric outcomes (Table 2), including receipt of magnesium for seizure prophylaxis, administration of intravenous antihypertensive medications while inpatient, and rates of requiring oral antihypertensive medications at discharge.
 Fig. 1.:
Fig. 1.: Participant flowchart.
 Table 1.:
Table 1.: Demographics
 Table 2.:
Table 2.: Obstetric Outcomes
Patients randomized to the remote monitoring arm had significantly higher rates of blood pressure ascertainment within 10 days of discharge (91.7% vs 58.4%, P<.001) (Table 3). There were 11 (11.5%) patients in the intervention arm whose only qualifying blood pressure was a postdischarge in-person ascertainment, yielding a true remote monitoring uptake rate of 80.2%. In those who had at least one remote blood pressure measure (n=77), the median number of blood pressure checks was 15 (6–26) and the median duration of remote monitoring use was 14 days (9–16). There were no significant differences in rates of antihypertensive initiation or up-titration postdischarge (9.4% vs 6.9%, P=.530), readmission for hypertension (5.0% vs 4.2%, P=.792), or unscheduled visits for hypertension (5.0% vs 12.5%, P=.059) compared with office-based monitoring. Overall, attendance at postpartum visits was high regardless of treatment arm (78.1% vs 70.3%, P=.210).
 Table 3.:
Table 3.: Postdischarge Outcomes
When the primary outcome was stratified by race and randomization group, a smaller percentage of Black patients assigned to in-office surveillance had their blood pressures checked, compared with White patients (41.2% vs 69.5%, P=.007), but there was no difference for patients assigned to remote management (92.9% vs 92.9%, P>.99 [Fig. 2]). There were not enough patients in the other racial or ethnic categories for further analysis. Primary and secondary outcomes stratified by race and randomization group are depicted in Table 4.
 Fig. 2.:
Fig. 2.: Blood pressure ascertainment in each arm, stratified by race.
 Table 4.:
Table 4.: Postdischarge Outcomes Stratified by Race and Randomization Group
Only 47 (23.9%) patients completed the poststudy survey: 19 (40.4%) were assigned to in-office surveillance and 28 (60.6%) to remote monitoring. Of the respondents, 91.4% either somewhat or strongly agreed that blood pressure follow-up is important for long-term health. Of those randomized to office-based monitoring, 52.6% reported that they would have preferred to monitor their blood pressure at home rather than present to an in-person visit. Of those enrolled in remote monitoring, 96.4% were either comfortable or very comfortable with home blood pressure monitoring; one respondent remained neutral.
DISCUSSIONIn this randomized controlled trial evaluating postpartum blood pressure monitoring, we found that remote monitoring increased the rate of blood pressure ascertainment within 10 days of hospital discharge after delivery and erased the disparity in ACOG guideline–concordant care between Black and White patients in the remote arm. These findings are consistent with evidence from other trials that found increased blood pressure ascertainment in patients participating in remote monitoring.6,10 Moreover, the total number of blood pressures recorded and duration of monitoring among remote monitoring participants was greater than the data obtained through the current standard of care. Therefore, remote monitoring presents an opportunity to improve follow-up for patients with hypertensive disorders in the postpartum period.
Neither the number of unscheduled visits for hypertension nor the number of antihypertensive medications initiated after discharge differed significantly between groups, which is consistent with prior studies.6 Though not statistically significant, the remote monitoring group had an increased number of unscheduled ambulatory visits, primarily in the hospital obstetric triage. This increase likely reflects that the protocol for the remote monitoring group worked as intended as it identified patients at risk of complications and in need of further evaluation. However, it is unclear whether this increased use of resources decreased the rate of hypertension-related complications. Notably, the improved rate of follow-up did not translate into fewer readmissions, which contrasts with previous studies.6,9 Due to the low postpartum readmission rate, it is possible we were underpowered to assess this important clinical outcome. To reduce the number of higher-cost emergent visits, it would be prudent to establish safe protocols for further evaluation of patients in the outpatient, rather than inpatient, setting. However, it is important to note that this study was not powered for these secondary outcomes when taking these results into consideration for future studies and protocols.
In our study, remote monitoring eliminated the disparity in postpartum blood pressure ascertainment between Black and White patients. Inequities in social determinants of health, and root causes including racism and discrimination, contribute to increased barriers to care for people with historically marginalized identities, including lower attendance at postpartum visits by Black individuals.11–15 Black patients are disproportionately affected by preeclampsia and more likely to experience maternal and fetal complications related to hypertensive disorders of pregnancy in the postpartum period.16–19 As hypertensive disorders of pregnancy are among the most preventable causes of maternal mortality, it is imperative to seek improvement in this domain. Our study adds to the evidence that remote access strategies reduce racial disparities in utilization of postpartum care, including hypertension-related follow-up.20,21 However, remote monitoring in isolation will not solve the systematic issues that contribute to poorer outcomes for Black patients. Moreover, future studies will need to examine whether the observed reduction in racial disparities in postpartum blood pressure ascertainment translates to better clinical outcomes, thus promoting health equity.
There are several strengths to our study. This was a well-powered multicentered randomized controlled trial, which reduces the effect that confounding factors may have on the results. There was a well-established prespecified postpartum hypertension triage protocol that was adhered to throughout the study time frame. This protocol, as well as the limited number of physicians monitoring and interpreting remote blood pressures, likely improved consistency in clinical management of patients. Lastly, this trial purposefully included two of the largest-volume obstetric institutions in the state, where remote monitoring had not previously been studied, resulting in a diverse study population of high-risk patients affected by hypertensive disorders of pregnancy and allowing for a high degree of generalizability.
There are also limitations to our study. Participants in this study comprised a diverse group, but our study excluded patients who did not speak English, thus limiting application to non–English-speaking patients. Although this study was powered to detect a difference in blood pressure ascertainment rates, it was not powered for our secondary outcomes, particularly readmission rate. Recent studies show that an estimated 2.5–5.1% of patients with hypertensive disorders of pregnancy are readmitted due to hypertension-related issues.22,23 Based on these data, a larger sample size would be necessary to analyze this important, though relatively uncommon, event. Another crucial element for instituting remote monitoring is patient satisfaction. Multiple studies have shown that patients prefer remote monitoring.6,10,24 Patient satisfaction was an intended secondary outcome for our study as well, but too few patients responded to perform a meaningful analysis. Large-scale implementation of remote blood pressure monitoring would require more staff and technology, particularly for practices caring for high numbers of patients with hypertensive disorders of pregnancy. We recognize that not all institutions may have staff resources to support remote monitoring platforms, which would limit generalizability of this approach. It is unclear whether the reduction of in-office visits would counter the increased resource need for remote monitoring. Before practices and hospital systems can adopt remote monitoring, large-scale analysis of cost and effect on long-term hypertensive complications will be necessary. Our study adds to the body of evidence that remote monitoring for postpartum hypertension is feasible and effective for a variety of patient populations, though cost analyses and long-term outcomes have rarely been assessed.6,9,10,24
In conclusion, the postpartum period has been identified as a particularly useful target for telehealth interventions. Our findings suggest that remote blood pressure monitoring is not only feasible, but significantly improves blood pressure ascertainment with the potential to promote health equity.Authors' Data Sharing Statement Will individual participant data be available (including data dictionaries)? Yes. What data, in particular, will be shared? Trial protocol and de-identified individual participant data. What other documents will be available? Not available. When will data be available (start and end dates)? After publication. By what access criteria will data be shared (including with whom, for what types of analyses, and by what mechanism)? At discretion of authors, by email from the corresponding author for researchers who provide a methodologically sound proposal for performing individual participant data meta-analysis.
REFERENCES 1. Gestational hypertension and preeclampsia. ACOG Practice Bulletin No. 222. Obstet Gynecol 2020;135:e237–60. doi: 10.1097/AOG.0000000000003891 2. Clapp MA, Little SE, Zheng J, Robinson JN. A multi-state analysis of postpartum readmissions in the United States. Am J Obstet Gynecol 2016;215.113.e1–10. doi: 10.1016/j.ajog.2016.01.174 3. Petersen EE, Davis NL, Goodman D, Cox S, Mayes N, Johnston E, et al. Vital signs: pregnancy-related deaths, United States, 2011–2015, and strategies for prevention, 13 states, 2013–2017. MMWR Morb Mortal Wkly Rep 2019;68:2013–7. doi: 10.15585/mmwr.mm6818e1 4. Too G, Wen T, Boehme AK, Miller EC, Leffert LR, Attenello FJ, et al. Timing and risk factors of postpartum stroke. Obstet Gynecol 2018;131:70–8. doi: 10.1097/AOG.0000000000002372 5. Stuebe A, Borders AE, Bingham D. Optimizing postpartum care. Obstet Gynecol 2016;127:1192–3. doi: 10.1097/AOG.0000000000001487 6. Hoppe KK, Thomas N, Zernick M, Zella JB, Havighurst T, Kim K, et al. Telehealth with remote blood pressure monitoring compared with standard care for postpartum hypertension. Am J Obstet Gynecol 2020;223:585–8. doi: 10.1016/j.ajog.2020.05.027 7. Denicola N. Implementing telehealth in practice. Obstet Gynecol 2020;135:e73–9. doi: 10.1097/AOG.0000000000003671 8. Hoppe KK, Williams M, Thomas N, Zella JB, Drewry A, Kim K, et al. Telehealth with remote blood pressure monitoring for postpartum hypertension: a prospective single-cohort feasibility study. Pregnancy Hypertens 2019;15:171–6. doi: 10.1016/j.preghy.2018.12.007 9. Niu B, Mukhtarova N, Alagoz O, Hoppe K. Cost-effectiveness of telehealth with remote patient monitoring for postpartum hypertension. J Matern Fetal Neonatal Med 2022;35:7555–61. doi: 10.1080/14767058.2021.1956456 10. Hirshberg A, Downes K, Srinivas S. Comparing standard office-based follow-up with text-based remote monitoring in the management of postpartum hypertension: a randomised clinical trial. BMJ Qual Saf 2018;27:871–7. doi: 10.1136/bmjqs-2018-007837 11. Thiel de Bocanegra H, Braughton M, Bradsberry M, Howell M, Logan J, Schwarz EB. Racial and ethnic disparities in postpartum care and contraception in California's Medicaid program. Am J Obstet Gynecol 2017;217:47.e1–7. doi: 10.1016/j.ajog.2017.02.040 12. Bryant AS, Haas JS, McElrath TF, McCormick MC. Predictors of compliance with the postpartum visit among women living in healthy start project areas. Matern Child Health J 2006;10:511–6. doi: 10.1007/s10995-006-0128-5 13. Henderson V, Stumbras K, Caskey R, Haider S, Rankin K, Handler A. Understanding factors associated with postpartum visit attendance and contraception choices: listening to low-income postpartum women and health care providers. Matern Child Health J 2016;20:132–43. doi: 10.1007/s10995-016-244-7 14. Parekh N, Jarlenski M, Kelley D. Prenatal and postpartum care disparities in a large Medicaid program. Matern Child Health J 2018;22:429–37. doi: 10.1007/s10995-017-2410-0 15. Romagano MP, Williams SF, Apuzzio JJ, Sachdev D, Flint M, Gittens-Williams L. Factors associated with attendance at the postpartum blood pressure visit in pregnancies complicated by hypertension. Pregnancy Hypertens 2020;22:216–9. doi: 10.1016/j.preghy.2020.10.003 16. Johnson JD, Louis JM. Does race or ethnicity play a role in the origin, pathophysiology, and outcomes of preeclampsia? An expert review of the literature. Am J Obstet Gynecol 2022;226:S876–85. doi: 10.1016/j.ajog.2020.07.038 17. Shahul S, Tung A, Minhaj M, Nizamuddin J, Wenger J, Mahmood E, et al. Racial disparities in comorbidities, complications, and maternal and fetal outcomes in women with preeclampsia/eclampsia. Hypertens Pregnancy 2015;34:506–15. doi: 10.3109/10641955.2015.1090581 18. Gyamfi-Bannerman C, Pandita A, Miller EC, Boehme AK, Wright JD, Siddiq Z, et al. Preeclampsia outcomes at delivery and race. J Matern Neonatal Med 2020;33:3619–26. doi: 10.1080/14767058.2019.1581522 19. Wagner JL, White RS, Tangel V, Gupta S, Pick JS. Socioeconomic, racial, and ethnic disparities in postpartum readmissions in patients with preeclampsia: a multi-state analysis, 2007–2014. J Racial Ethn Heal Disparities 2019;6:806–20. doi: 10.1007/s40615-019-00580-1 20. Hirshberg A, Sammel MD, Srinivas SK. Text message remote monitoring reduced racial disparities in postpartum blood pressure ascertainment. Am J Obstet Gynecol 2019;221:283–5. doi: 10.1016/j.ajog.2019.05.011 21. Khosla K, Suresh S, Mueller A, Perdigao JL, Stewart K, Duncan C, et al. Elimination of racial disparities in postpartum hypertension follow-up after incorporation of telehealth into a quality bundle. Am J Obstet Gynecol MFM 2022;4:100580. doi: 10.1016/j.ajogmf.2022.100580 22. Mogos MF, Salemi JL, Spooner KK, McFarlin BL, Salihu HH. Hypertensive disorders of pregnancy and postpartum readmission in the United States: National surveillance of the revolving door. J Hypertens 2018;36:608–18. doi: 10.1097/HJH.0000000000001594 23. Lovgren T, Connealy B, Yao R, Dahlke JD. Postpartum management of hypertension and effect on readmission rates. Am J Obstet Gynecol MFM 2022;4:100517. doi: 10.1016/j.ajogmf.2021.100517 24. Hauspurg A, Lemon LS, Quinn BA, Binstock A, Larkin J, Beigi RH, et al. A postpartum remote hypertension monitoring protocol implemented at the hospital level. Obstet Gynecol 2019;134:685–91. doi: 10.1097/AOG.0000000000003479
Comments (0)