
Remember me
All the required data for this study was collected in a single interview within a mean time span of three months after cardiac surgery. In this study pre-operative evaluation is not done, according to the research conducted by Gomes et al.,10 he stated that pre-operative QoL will be lower than post-operative QoL.

Figure 3:
Personal History

Figure 4:
Prevalence of co-morbidities In Study Population
Patients normally have a concept of thinking that after surgery everything is going to be normal, but it’s noticeable that the therapeutic method can only decrease the sign and symptoms but do not cure them. Coronary artery disease is the most common disorder which is life-threatening in the world. This study gives the overall idea of how health-related quality of life and medication adherence shows an impact in patients after cardiac surgery.11
In this study out of 152 patients, 13% indulged in habits such as Smoking and 14% were Alcoholic and the remaining 37% were non-smokers and 36% were non-alcoholic and in patients the most commonly seen co-morbidity was HTN with 54.60% and the least found co-morbidity was Osteomyelitis with 1% and Typhoid with 1%. Majority of patients in our study of about 54.60 were hypertensive. Contrary to this study conducted by Stana Pacaric et al.12 according to risk factors, 21 (45%) participants were smokers, 35 (75%) had hypertension, 16 (34%) had diabetes, and 29 (61%) had high cholesterol. And also, study conducted by Reeni John, et al.,12 which reveals that majority of their subjects were prone to smoking and alcoholism. Hypertension was found to be the most common comorbid condition with about 56% of patients suffering from it followed by renal diseases with 4.50%. The study by Reeni John et al.,12 also had diabetes as the most common comorbid condition.

Figure 5:
Physical Component Summary (PCS)
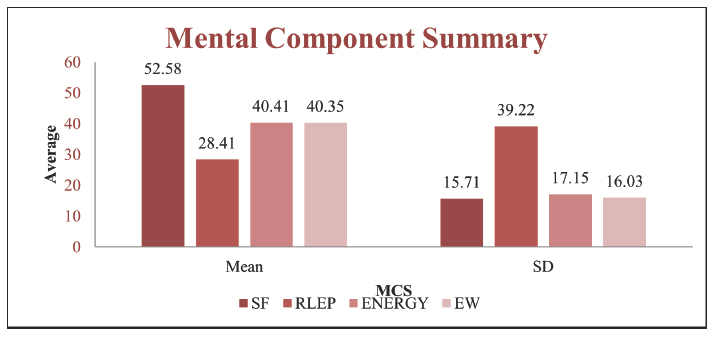
Figure 6:
Mental Component Summary (MCS)
HRQoL was assessed using SF-36 sub-scales scores, according to this study the Mean of Health changes, physical functioning, pain and role limitation of physical functioning to be 47.43, 58, 45.18, 30.44 respectively. Physical functioning dimension had highest mean and the lowest mean was seen in the role limitation due to physical functioning. And that of mental health revealed that the mean of social functioning, Role Limitation due to Emotional Problems (RLEP), energy, emotional well-being, to be 52.58, 28.41, 40.41, 40.35 respectively. Social functioning had the highest mean i.e., 52.58 and Role Limitation due to Emotional Problems (RLEP) had the lowest mean i.e., 28.41. Some of the following similar researches conducted on HRQoL assessment using SF-36 subscales showed following results, by Kurfirst et al.13 in Cardiac Surgery Department of Hospital Ceske Budejovice which showed significantly improvement in all 8 health domains and the mean of physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health was found to be 65.5, 51.1, 73.9, 51.8, 57.4, 73.6, 67.9, 70.6 which showed increased bodily pain and decreased role physical. By Colleen Gorman Koch et al.5 in those who have pre-operative baseline and follow up DASI (Duke Activity Status Index) which resulted in poor HRQoL after recovery from cardiac surgery. Here most patients reported improvement in functional quality of life after surgery. By Moheddine Younsi et al.,14 the average score of Physical functioning, role-physical, bodily pain, general health, social functioning, role-emotional, vitality, mental health were found to be 0.84, 0.53, 0.45, 0.50, 0.35, 0.37, 0.38, 0.34.
Comparison of the QOL scores in both males and females in the study revealed that females had slightly lower scores than males in MCS (role limitation due to emotional health, energy, emotional wellbeing, social functioning) with 21.525±35.020, 42.812±17.407, 38.562±16.231, 51.614±12.347 for females, 30.195±39.64, 38.936±16.645, 39.617±16.011, 53.165±16.32 for males, and there were all statistically significant differences in the QOL among the study subjects based of gender. These findings are consistent with the observations of Gautam et al.,15 where the QOL scores among males were higher in all domains except in general health.
Figure 7:
Physical Component Summary (PCS)
Figure 8:
Mental Component Summary (MCS)
Medication adherence was assess using MMAS-4 questionnaire tool and patients were sub scored as, highly adherent, moderately adherent and low adherent. In this study out of 152 patients, more patients were moderately adherent (39.47%) and patients were low adherent were least (28.29%) to their medication.
When correlating medication adherence with HRQoL, highly and moderately adherent patients to medication were having improved QoL. As a result of non-adherence patients did not get an appropriate benefit from surgical treatment and they showed low QoL. These results are similar to study done by Balasi et al.,11 where belief about medication adherence was good among most of the study patient and beneficially and effectiveness of drugs on quality of life after CABG surgery was promoted.
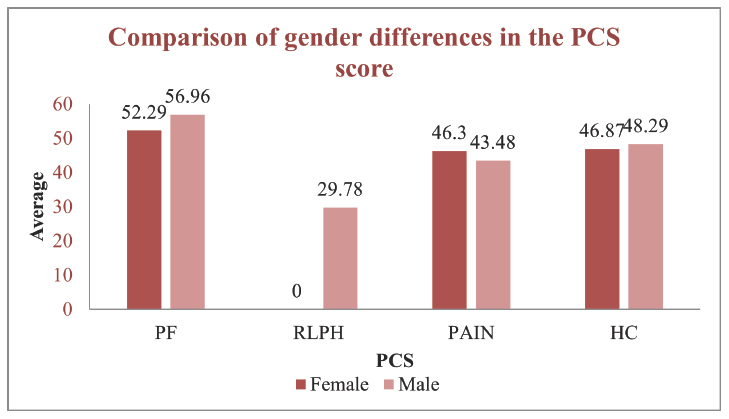
Figure 9:
Physical Component Summary (PCS)
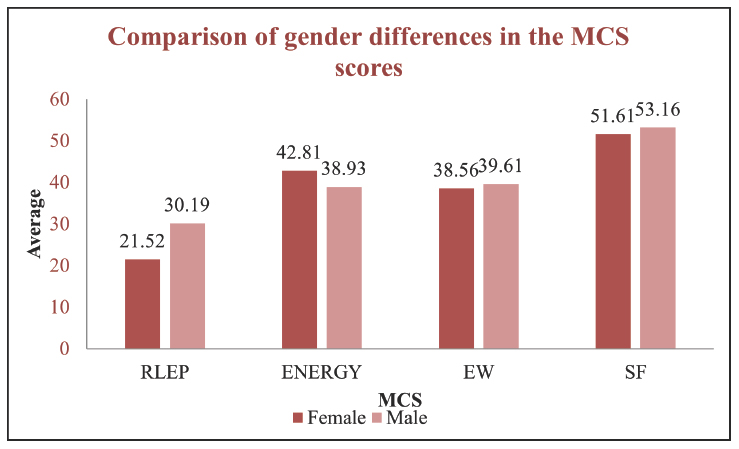
Figure 10:
Mental Component Summary (MCS)
The limited sample size and the fact that the study was conducted at a single location in one geographical area are both limitations of this study. One of the study’s shortcomings is that we lack sufficient data for economic evaluation, which will undoubtedly be the focus of future research. Patients undergoing emergency surgery were omitted from the study because they might not be able to offer reliable information about their health state before to surgery, which could be another research drawback. Patients who were receiving palliative revascularization were omitted from the trial, which might be a restriction since we couldn’t compare quality of life in patients with optimum revascularization to patients who were undergoing palliative revascularization. The findings of our study cannot be applied to the full population of CABG surgery patients in India, but they may be used to develop therapies that would enhance these patients’ quality of life.
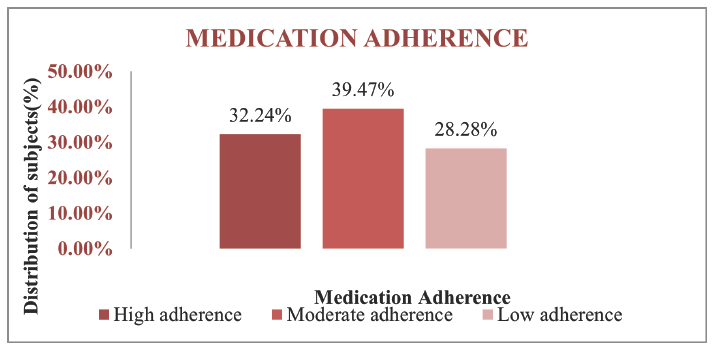
Figure 11:
Distribution of subjects based on Medication Adherence

Figure 12:
Physical Component Summary (PCS)
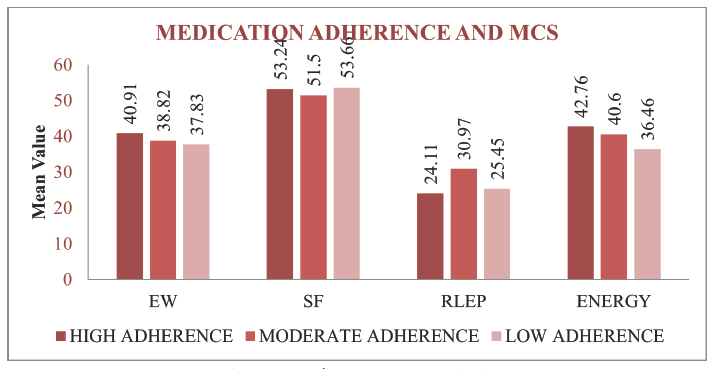
Figure 13:
Mental Component Summary (MCS)
Comments (0)