
記住我

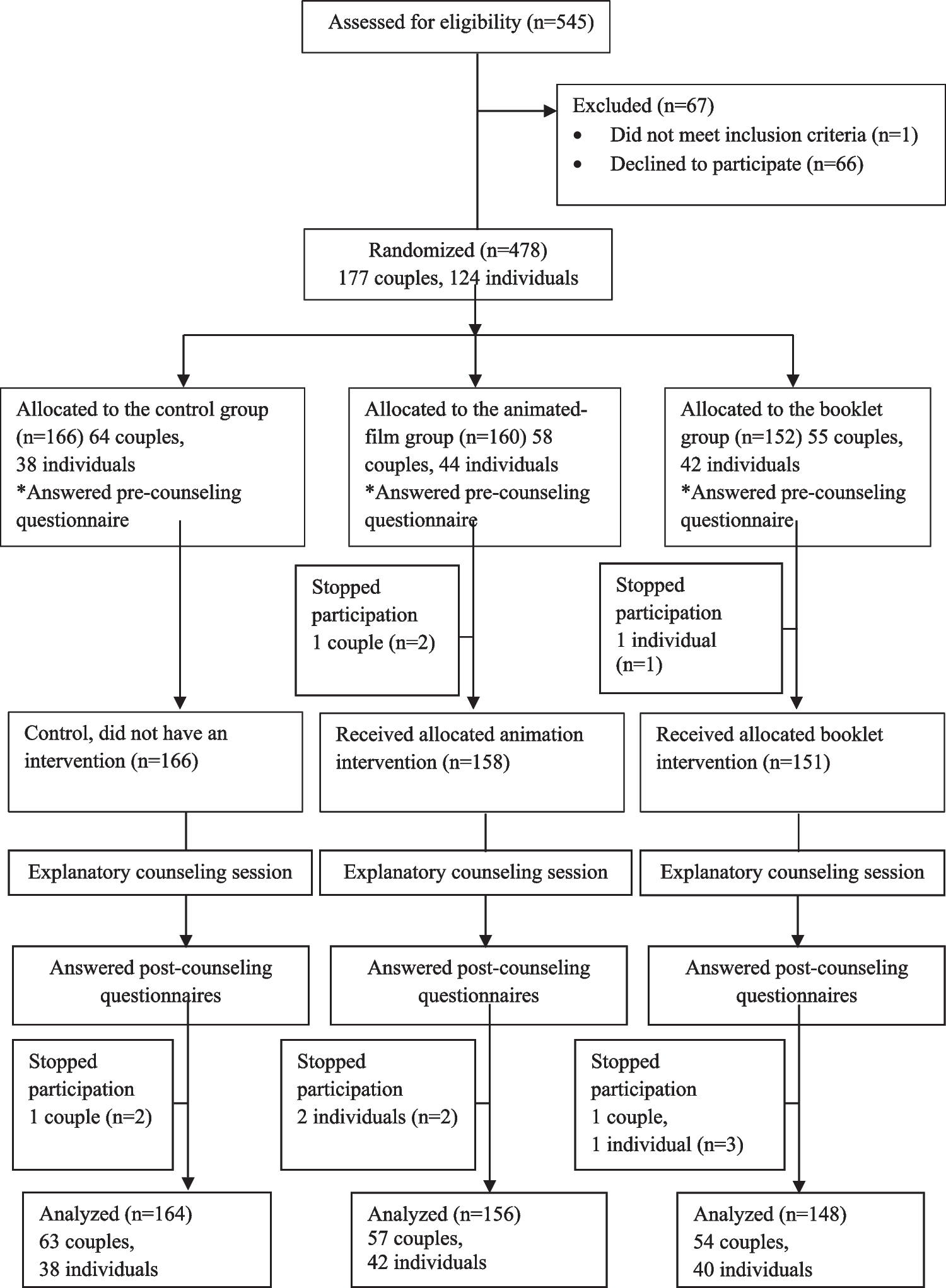
One hundred thirty-one patients, 19 men, and 112 women, were considered eligible for the study. Seventy-two patients were lost at first contact, including 64 who died and 8 whose telephone numbers were no longer active and could not be traced. Fifty-nine patients were contacted by telephone: 6 refused counseling and 53 agreed to make an appointment at the BRCA outpatient clinic of the Mauriziano Umberto I Hospital. Three patients canceled the counseling visit, and only 50 patients joined the study and answered the questionnaires.
The sample consisted of 50 subjects, 49 women and 1 man, aged 43 to 87 years, with a mean age of 61 years (S.D. 1.55).
After pre-test counseling, approximately 1 month after counseling, 39 patients (78%) underwent BRCA1/2 genetic testing (test group, TG), while 11 (22%) refused (no-test group, NTG). Among the latter only 3, in the context of second telephone contact, preferred not to share the reasons for their decision and therefore did not respond to questionnaire C.
The TG consisted of 38 women and one man, while the NTG consisted of 11 women.
Of the 39 subjects who decided to undergo testing, 2 had a positive result for class 5 mutation; of these two, one patient was diagnosed with ovarian cancer at the first visit with transvaginal ultrasound. In 29 subjects, no mutation was identified, and 8 have not yet received the result.
TG patients showed a trend towards a younger mean age at cancer diagnosis of 45.3 years (S.D. = 1.57) compared to the NTG with a mean age of 52.3 years (S.D. = 3.79) (p = 0.056); this difference appears remarkable, but not statistically significant. The mean time from cancer diagnosis to genetic testing prescription was similar between the two groups: 14.4 years (S.D. = 2.3) for the TG and 13.2 years (S.D. = 3.97) for the NTG (p = 0.65). The mean age at the time of the genetic testing proposal was 59.7 years (S.D. = 1.63) for the TG and 65.5 years (S.D. = 3.88) for the NTG (p = 0.126).
Socio-demographic indicators, medical comorbidities of the sample under study, and the personal context obtained through questionnaire A are shown in Table 1.
Table 1 Socio-demographic indicators, medical comorbidities of the sample under study, and the personal context of the test group and no-test group. S.D.: standard deviationSubjects in the NTG were more likely to have a partner (p = 0.048). Subjects in the NTG show a lower tendency to tobacco use than the TG (p = 0.06), and adherence to screening campaigns for breast and/or cervical cancer tends to be higher in the TG (71.8%) compared to the NTG (45.5%) (p = 0.103); these differences appear noteworthy, although not significant.
A higher proportion of patients in the TG has daughters, 63.3% vs 37.5% in the NTG (p = 0.189), although these results do not reach statistical significance, while the percentage of male offspring looks superimposable.
In both samples, perceived knowledge about BRCA1/2 gene mutations was overlapping, in the TG, 23% considered themselves well-informed, 29% had heard of the topic, and 28% had never heard of it, compared to 27%, 27%, and 46% of the NTG, respectively.
During the pre-test counseling, the study participants were asked to rate on a scale from 1 = “very important” to 4 = “it is not important at all,” the level of involvement concerning each proposed question. The role of personal and family history of cancer was investigated, and no differences emerged between the groups in the choice to undergo testing; 20.5% of TG vs 27.3% of NTG patients consider oncological family history to be “very important” (Fig. 1). Personal history of cancer is a decisive factor in the counseling process according to both groups, for 98% of the patients in the TG and 100% of the NTG (p = 0.99).
Fig. 1
Role of family history of cancer in the decision to undergo genetic testing
According to both groups, the need to protect their offspring was "very important" in the decision to undertake genetic testing to an almost superimposable degree (64.1 TG vs 54.5 TG, p = 0.99). Moreover, regarding the fear of passing on the possible genetic mutation to their offspring, the two groups overlapped, with 33.3% in the TG and 27.3% in the NTG (p = 0.7344).
Subjects in the TG were more likely to discuss the possibility of genetic testing with their family (94.9% of the TG versus 54.5% of the NTG, p = 0.004). In contrast, 45.5% of NTG considered it inappropriate to inform or discuss pre-test counseling with relatives (p = 0.004). The 82.1% of the TG appears to have a family more supportive of genetic testing, compared with 54.5% of the NTG (p = 0.105). Only 33.3% of the TG claimed to have been influenced by family members in their decision to take the BRCA1/2 genetic test, in contrast, 54.5% of those who refused the test reported having been influenced by their family (p = 0.293), although not statistically significant, these differences appear remarkable.
To assess the impact of the decision to undergo oncogenetic counseling as a distressing experience, the IES was proposed. The results were analyzed using the mean of the answers; higher results correspond to higher levels of distress of the subject. Comparing the mean scores of the two groups, a mean of 19.85 (S.D. 1.11) for the TG, and a mean of 23.36 (S.D. 2.56) for the NTG (p = 0.164) has been calculated.
Participants in the study were asked to describe their everyday life attitude, thus defining a personal tendency towards positivity or negativity as seen in Fig. 2.
Fig. 2
Everyday life attitude of patients under study
Those who considered themselves positive in dealing with everyday life events were 69.2% of the TG vs 54.5% of the subjects in the NTG. Only in the NTG did 18.2% of subjects claim to have a negative approach to everyday life events. (p = 0.025).
Between the NTG, 75% of the subjects felt a sense of fear about the consequences of any information related to genetic testing, both personally and concerning their family, fear of having passed the mutation on to offspring emerged in 37.5% of patients. Sixty-three percent did not think it was fair to involve family members in this decision. More than half of the patients (62.5%) raised logistical issues as a reason for refusing the test: the hospital is far away, and the possibility of potentially carrying a mutation would have meant numerous follow-up visits in case of a positive genetic test result.
留言 (0)