
記住我



This retrospective study was approved by the Institutional Review Board of our hospital. Five patients (age, 77–86 years; mean age, 80 years) with NSCLC who underwent SBRT between February 2017 and April 2019 were included in the study. The male:female ratio was 3:2. Table 1 summarizes patient characteristics. The mean gross tumor volume (GTV) from the exhale-phase 3DCT was 3.0 ± 0.9 cm3. At our hospital, tumors with a 3D migration of ≤ 10 mm are irradiated under free-breathing conditions. This study investigated the ITV settings for irradiation under free respiration, and all patients had tumors in the upper lobe with relatively small respiratory migration.
Table 1 Patient characteristics used in this study2.2 CT simulationIn all patients, a 3DCT scan of the thoracic region was performed in the axial mode, followed by a 4DCT scan using an Aquilion PRIME CT scanner (Canon Medical Systems Co., Tochigi, Japan) with a breath track (Engineering System Co., Ltd, Nagano, Japan) that acquired displacements of a marker on the patient's abdomen using a charge-coupled device camera. A thermoplastic sheet (Engineering System Co., Ltd., Nagano, Japan) was used as an abdominal compression device to limit the motion of the tumor to < 10 mm in the 3D vector. 3DCT scans were acquired with a 2.0 mm slice thickness under end-of-exhale and end-of-inhale breath-holds. During acquisition, the waveform of the breath-track system was used to visually confirm that the breath was held firmly.
In our hospital, to depict the entire movement of the tumor per respiratory cycle, 4DCT scans were acquired only around an area that included the lung tumor during un-coached free breathing in the axial cine mode. The cine duration was set to 10.5 s, which was sufficiently longer than the normal respiratory cycle (4 s). Furthermore, the slice thickness was 0.5 mm, and the reconstructed time interval was 0.5 s, which generated 21-phase images. The CT data were reconstructed in a field of view of 500 mm on a 512 × 512 grid for both CT scans. The measurement of tumor motion for 3DCT and 4DCT was performed using the contouring software in Eclipse version 13.6 (Varian Medical Systems, Palo Alto, CA, USA). The software created a tumor structure for each respiratory phase and analyzed the shift in the center of gravity from the reference structure in all three directions.
2.3 Treatment planningRadiation treatment planning, including the delineation of the GTV on the CT image, was performed using Eclipse. The following two approaches were used to define the ITVs: (1) the GTVs were outlined on end-of-exhale and end-of-inhale breath-hold images of 3DCT, which were combined to form a 3DCT-based ITV, and (2) the GTVs were outlined on each of the 21 phases of 4DCT, which were combined to form a 4DCT-based ITV. Here, 3DCT- and 4DCT-based ITV envelope the GTV of 3DCT and 4DCT, respectively. Tumor regions extracted by different radiation oncologists have been reported to differ by up to 3 mm, and this uncertainty and a setup margin of 5 mm are included in the planning target volume (PTV) margin (8 mm) [23].
Treatment planning was performed using eight non-coplanar static photon beams of 6 MV flattening filter-free (FFF) and a 2 mm multi-leaf collimator margin with a total prescribed dose of 48 Gy to 95% of the PTV in four fractions.
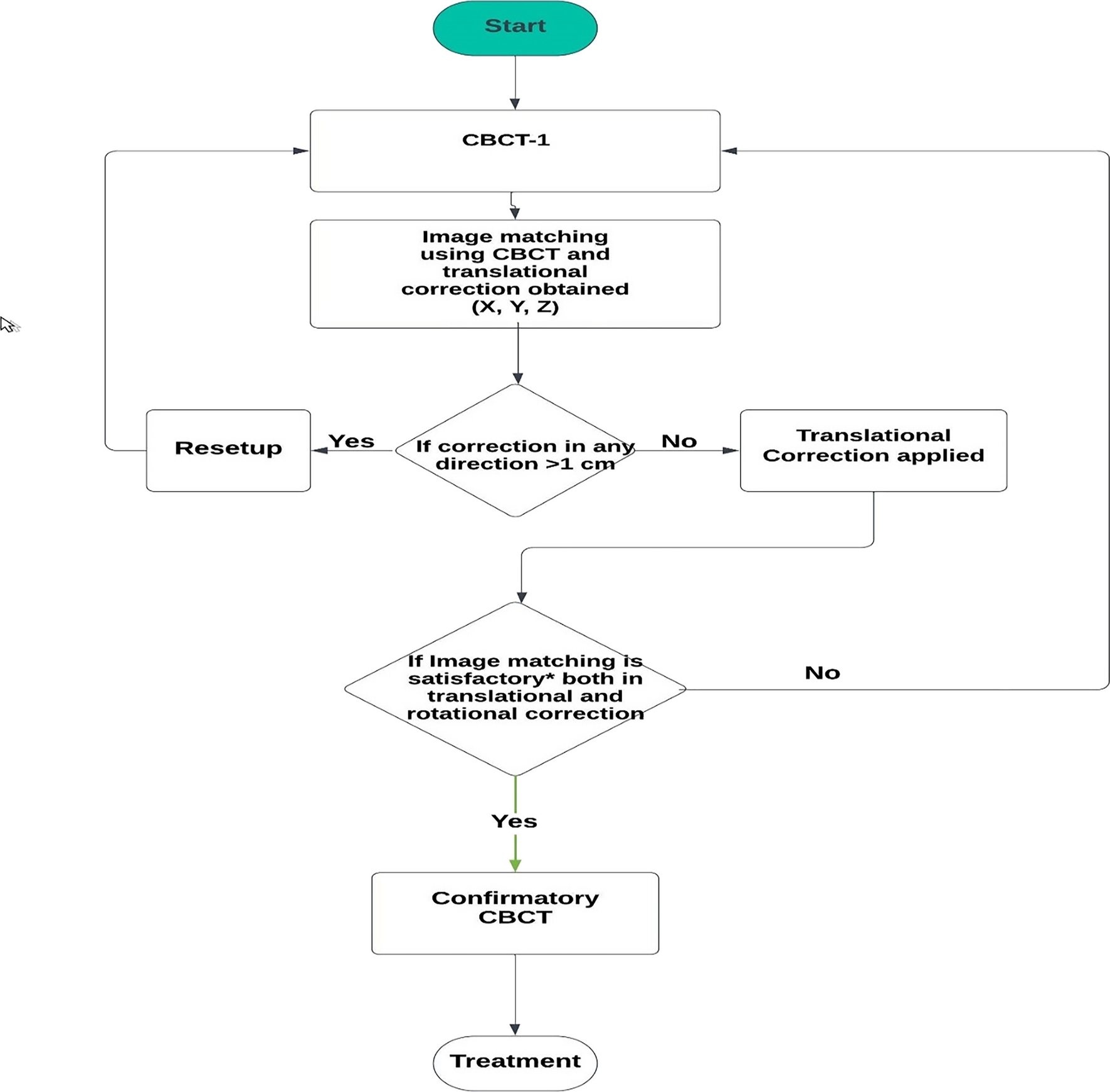
2.4 Image acquisitionFree-breathing cone-beam computed tomography (CBCT) was performed before irradiation to align the tumor with the isocenter. Initially, automatic registration of the bone anatomy was completed between the planning CT (end-of-exhale breath-hold 3DCT) and CBCT images, followed by manual refinement of the tumor location. To confirm the tumor location, EPID images (EPID 1st and EPID 2nd) were acquired sequentially using the first and second beams of each fraction under free-breathing conditions. Images of each patient were acquired using 6 MV FFF X-rays from a linear accelerator (TrueBeam STx, Varian Medical Systems, Palo Alto, CA, USA) in cine mode on an EPID (aS-1200, Varian Medical Systems). Using the cine mode of the EPID in this system, images were acquired every 0.04 s (image acquisition rate: 25 frame/s). During image acquisition, the source-to-axis distance (SAD) and source-to-imaging distance (SID) were set to 100 and 150 cm, respectively. The matrix size of the images was 1,024 × 768 pixels, and the pixel size was 0.392 mm. Forty image sets were acquired in four sessions for five cases, each consisting of images captured from two directions.
2.5 EPID analysis2.5.1 Target position reconstructionThe tumor position on an EPID image was defined as the center of gravity of the tumor area, which was manually determined by one radiation oncologist and two radiologists using image processing software (Image J, National Institutes of Health, USA). The relationship between the tumor position on the isocenter (X, Y, and Z) and its projection position (x and y) on an EPID image for an irradiation gantry angle θ can be defined using the following equations:
$$X = x\cdot \frac(180-\theta )}\cdot \frac (90\le \theta \le 180)\, or \,X = x\cdot \frac\left(\theta -180\right)}\cdot \frac (180\le \theta \le 270),$$
(1)
$$Y = x\cdot \frac(180-\theta )}\cdot \frac (90\le \theta \le 180)\, or \,Y = x\cdot \frac\left(\theta -180\right)}\cdot \frac (180\le \theta \le 270),$$
(2)
$$Z = y\cdot \frac.$$
(3)
where an SAD of 100 cm is the distance between the MV sources, and an SID of 150 cm is the distance between the MV sources and the EPID (Fig. 1).
Fig. 1
Relationship between the tumor position on the isocenter (X and Y) and its projection position x on an EPID image for an irradiation gantry angle θ. EPID, electronic portal imaging device
For each of the 20 treatment fractions, we calculated the magnitude of tumor motion in the 2D projection images. The irradiation gantry angles are listed in Table 1. The couch angle was set to 0°. In this case, there was no uncertainty in the motion in the CC direction, because the motion was perpendicular to the imaging beam at all gantry angles. However, the motion parallel to the beam cannot be resolved for motion in the LR and AP directions, and none of its moving components can be determined. Therefore, X and Y estimated the amount of movement using calculations. Because the projection images were acquired in two directions per fraction, calculations were performed for 40 treatment beam angles. Setup errors were obtained by averaging the residual tumor misalignment from the isocenter measured during irradiation in all patients.
2.6 Tumor coverageIn radiotherapy for tumors with respiratory movements, the ITV must cover the actual movement of the tumor while setting an irradiation field. Therefore, the movement range coverage during irradiation of the ITV and PTV sets during planning was calculated. This study used three standard deviations (± 3 SD) from the mean position of the tumor on the EPID images as the range of breathing motion during irradiation. For each patient, the SD for inter-observer variations was calculated from the root mean square (RMS) of the random errors in tumor motion by the observers, as follows:
$$SD = \sqrt\sum_^_}^}.$$
(4)
where N is the number of observers. σj represents the random error of tumor motion for an observer j.σj was given by
$$_ = \sqrt\sum_^_}^}.$$
(5)
where n is the number of image sets obtained using the EPID. σi,j represents the random error on an image set i for an observer j.
Tumor coverage was evaluated based on the extent to which the peak-to-peak breathing amplitude on the planning CT scan covered the range of tumor motion.
$$Tumor\ coverage = -(1-\frac)\times 100.$$
(6)
Using this equation, we evaluated whether the moving tumor was within the planned ITV during irradiation. PTV coverage was calculated by adding a PTV margin of 8 mm to the planned ITV. Here, the greater the planned ITV or PTV relative to the tumor motion during irradiation, the greater the tumor coverage. A value with a negative sign indicates that the tumor is outside the planned ITV or PTV.
2.7 Statistical analysisStatistical analyses were performed using JMP software version 16 (SAS Institute Inc., Cary, NC, USA). A paired t-test was used to determine whether 3DCT and 4DCT data were significantly different. Differences of P < 0.05 were considered statistically significant.
留言 (0)