Question no. 1: What is the effectiveness of preventive interventions for IUTI during emergency digestive surgery?Literature review
The current evidence on preventive interventions for IUTI is mainly derived from observational studies in colorectal and gynecological surgery. Pertinent studies included heterogeneous cohorts of patients treated in both elective and emergency surgical settings. Thus, data are blunted by potential confounders and biases, impacting on the estimate of IUTI incidence during emergency digestive surgery, and on the risks and benefits of some preventive interventions for IUTIs. Moreover, the literature concerns primarily preventive interventions for iatrogenic ureteral injuries.
Epidemiology of IUTIs
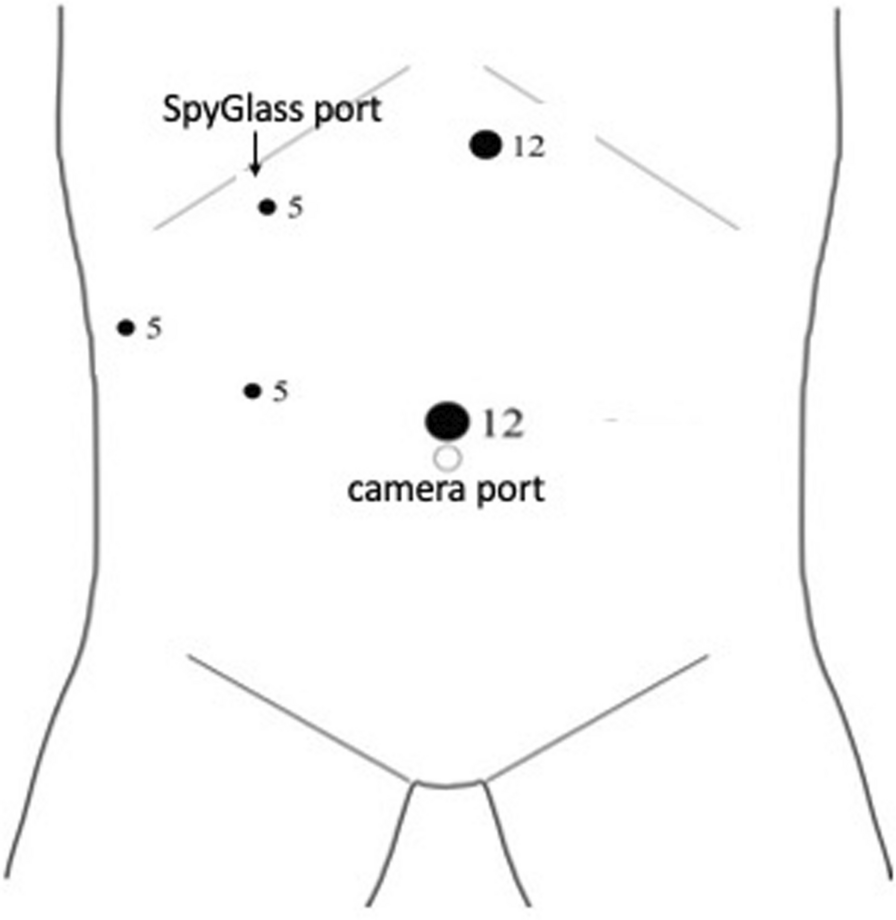
In a case series of laparoscopic emergency surgeries, the reported rate of bladder injuries was 0.36% [28]; these injuries usually occurred during the insertion of suprapubic trocars, with only 1 over 6 cases being recognized intraoperatively [28]. Therefore, it is essential to visually inspect the site on insertion and extraction to avoid unrecognized lesions [29,30,31].
Urethral injuries are rare and usually described in the context of elective rectal surgery that involves accessing the rectum and the mesorectal dissection from bottom to up, such as abdominoperineal and transanal total mesorectal excision [32,33,34,35,36,37].
Nowadays, there is no literature reporting data on the preventive strategies for renal, bladder, or urethral IUTIs, nor on preoperative imaging assessment to identify anatomical landmarks or proper trocar positioning [31]. Computed tomography (CT) with excretory phase is the best imaging technique to evaluate the kidneys and the urinary collecting system [38,39,40]. This phase is highly sensitive for the evaluation of urinary tract anatomy and its variations, even in patients with greater risk of IUTI (e.g., locally advanced sigmoid or rectal cancer) [41].
Ureteral injuries can have severe consequences with high morbidity and mortality rates, especially when their recognition is delayed [42, 43]. These injuries can also substantially increase healthcare costs and result in medico-legal litigations [44]. When the injury is identified during surgery, a timely repair generally leads to favorable outcomes [30]. However, in the majority of the cases, these injuries are missed intraoperatively (50–70%) and require further surgery when the symptoms related to the complication become apparent [45].
The incidence of ureteral IUTI during colorectal surgery varies between 0.28 to 0.69% based on several retrospective studies analyzing large national databases [7, 14, 43, 46, 47]. While the occurrence of IUTI can be expected to be higher in complex surgical scenarios, such as acute diverticulitis, locally advanced sigmoid or rectal cancer, inflammatory bowel disease, and emergency surgery, Chiu et al. [48] reported a 0.3% incidence of ureteral IUTI in a cohort of 811,071 partial colectomies and anterior rectal resections for diverticulitis. Halabi et al. [46] analyzed 2,165,848 elective and emergency colorectal surgical procedures and found higher rates of ureteral injuries in elective surgery compared to emergency surgery (3.0/1,000 vs. 2.4/1,000; p < 0.001). The highest rates of ureteral IUTI were associated with rectal cancer (7.1/1,000), followed by diverticular disease (2.9/1,000), Crohn’s disease (1.9/1,000) and ulcerative colitis (1.7/1,000) [46]. In a retrospective study by Joosten et al. [10], 126 patients who underwent salvage surgery for pelvic sepsis after low anterior resection or Hartmann's procedure for rectal cancer were examined. Among them, eight patients (6.3%) experienced ureteral injury, four patients (3.2%) experienced bladder injury and one (0.79%) experienced urethral injury. Notably, all patients who developed IUTI had undergone neoadjuvant radiotherapy.
Overall, an increasing incidence of IUTI in digestive and gynecological surgery has been reported over time [46, 47, 49]. While many authors have attributed the increased risk of IUTI to the increased use of minimally invasive surgery (MIS) [14, 43, 50], other authors observed contrasting results, reporting a decreased IUTI rates in association with the increased use of MIS over time [47, 48, 51].
Based on a recent nationwide survey of Swiss general surgeons, formal identification of the left ureter during sigmoid colectomy or rectal surgery was considered mandatory by 83.7% of participants, while only 31.7% considered the identification of the right ureter mandatory during right colectomy [52]. Intraoperative ureter identification is typically performed through visualization and exploration in both MIS and open surgery, or by manual palpation during open surgery. To minimize the risk of IUTI, surgeons need a technology that enhances intraoperative visualization of the ureters, preventing injuries, and facilitating prompt detection and subsequent repair in case of an injury. During the last decades, prophylactic ureteral stents, including lighted ureteral stents and near-infrared fluorescent ureteral catheters, and fluorescent dyes such as indocyanine green and methylene blue, have emerged as potentially useful and promising techniques for the prevention of IUTI [3, 53, 54].
Risk factors for ureteral injuries
Ureteral injuries can occur at various stages of colorectal surgery, including the mobilization of the colon and rectum, dissection of the mesentery, ligation of the inferior mesenteric artery, and division or anastomosis of the bowel. In particular, the dissection between Toldt’s and Gerota’s fascia and the ligation of the inferior mesenteric vessels are considered the most technically risky phases for IUTI. Several factors contribute to a higher risk of IUTI, including disease-related factors, such as inflammation, locally advanced colorectal cancers, and previous radiotherapy, as well as patient-related factors, such as visceral obesity and a history of previous colorectal or gynecological surgery, may result in more difficult dissection and a higher risk of IUTI [55]. Coakley et al. [7] showed that diverticular disease (OR = 2.115, 95% CI 1.635–2.736), T4 malignancy (OR = 1.797, 95% CI 1.168–2.766), and open surgery (OR = 1.316, 95% CI 1.027–1.686) were significantly associated with a higher risk of IUTI during colectomy, while body mass index (BMI) and Charlson Comorbidity Index did not show a significant association. Halabi et al. [46] identified rectal cancer (OR = 1.85), adhesions (OR = 1.83), metastatic cancer (OR = 1.76), history of weight loss and malnutrition (OR = 1.08), and surgery at teaching hospitals (OR = 1.05) as predictors of ureteral injuries at logistic regression model analysis. Additionally, a multivariable logistic regression analysis on 136,440 left-sided colectomies identified conversion to open surgery (OR = 1.39, 95% CI 1.08–1.79), higher BMI (OR = 1.02, 95% CI 1.01–1.03), diverticular disease (OR = 2.04, 95% CI 1.67–2.50), increasing operative complexity (OR = 1.04, 95% CI 1.04–1.05) and T4 colon cancer compared to T1 (OR = 3.3, 95% CI 1.6–6.9) as preoperative and operative characteristics associated with ureteral injury [56]. In preoperative surgical planning, it is crucial to consider and explore these risk factors to facilitate the adoption of appropriate preventive strategies for IUTI.
Ureteral stents and lighted ureteral catheters
Studies examining the usage trends of ureteral stents in colectomies for diverticulitis observed an increase in their utilization, particularly during laparoscopic surgery, with rates rising from 6.66 to 16.30% between 2000 and 2013 [48].
In 2014, the Clinical Practice Guideline Task Force of the American Society of Colon and Rectal Surgeons stated that prophylactic ureteral stents (PUS) should be “used at the discretion of the surgeon”, commenting that this was a weak recommendation based on low-quality evidence. The group noted that factors such as cost, increased operative times, and low frequency of injuries did not favor its routine use. However, they suggested that patient-specific factors, including morbid obesity, irradiated tissues, abnormal anatomy, and re-operative surgery, may justify PUS use [57].
Retrospective case series and cohort studies examining the impact of ureteral stents on IUTI prevention have reported conflicting results regarding the utility of PUS. Coakley et al. [7] analyzed 51,125 patients using the colectomy-targeted American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database and found a statistically significant association between PUS and lower rates of IUTI based on multivariate analysis. The most common use of PUS was observed in sigmoid colectomies for chronic (31.2%) and acute (10.9%) diverticular disease, malignancy (29.7%) and inflammatory bowel disease (10.2%) [7]. However, a more recent study by Dolejs et al. [56] using a 2:1 propensity score-matched analysis of the ACS NSQIP left-sided colectomy database showed no statistically significant difference in IUTI incidence with or without ureteral stenting (0.7% with stent vs. 0.9% without stent). Conversely, ureteral stent placement was associated with slightly higher morbidity, primarily related to postoperative ileus and kidney disease, as well as a 46-min longer operative time. Nevertheless, in the subgroup analysis that included only diverticular disease, PUS was significantly associated with a decreased rate of ureteral injuries (0.3% with stent vs. 0.8% without stent, p < 0.01) [56]. A systematic review conducted in 2019 identified 18 retrospective and 4 prospective cohort studies published between 1982 and 2018, which reported a pooled incidence of IUTI of 1.49% in patients with PUS compared to 0.17% in those without stents [58]. However, the increased rate of IUTI among stented patients likely reflects a selection bias due to the selective use of ureteral stents in more complex cases. Therefore, selective PUS should be considered as a marker of higher surgical complexity and increased risk of IUTI. When analyzing the pooled data on morbidity [58], the most frequent complications associated with PUS were transient hematuria [59], urinary tract infections (3.92%) [7, 59,60,61,62,63,64,65,66,67], acute kidney injury (3.05%) [62, 64, 67,68,69], ureteral injury due to stent placement (0.12%) [59,60,61,62,63,64,65,66, 69,70,71,72], transient ureteral obstruction (1.95%) [64, 69, 71], and urinary retention (3.5%) [59, 70, 72].
On the other hand, a more recent systematic review and meta-analysis conducted by Hird et al. [4] showed no difference in the odds of IUTI when comparing 3,064 stented patients to 50,060 controls (OR = 1.30, 95% CI 0.90–4.29). Moreover, PUS was not significantly associated with any postoperative adverse event. However, their use resulted in a 49-min increase in operating room time [4]. Similarly, Cirocco et al. [73] reported that the use of PUS leads to a longer operation time without any impact on IUTI rates, morbidity, mortality, or length of hospital stay.
Lighted ureteral catheters with near-infrared fluorescence have been developed to visualize ureters with minimal dissection and to overcome the lack of haptic feedback during MIS [74,75,76]. A systematic review published in 2022, based on 6 studies, showed a 0.33% incidence of IUTI after the use of lighted ureteral stents. The most common complications associated with stents were transient hematuria (97.6%), urinary tract infections (3.3%) and acute kidney injury (2.5%) [55]. More recently, Ryu et al. [77] investigated the utility of ureteral navigation using fluorescent ureteral catheters during laparoscopic colorectal surgery for locally advanced cancers. In their study, fluorescent catheters were inserted using cystoscopy before surgery in 143 patients with T4 colorectal cancer. There were no incidences of IUTI (0% with vs. 1.6% without fluorescent stents) or conversion to open surgery in the stented group, although statistical significance was not reached.
Currently, no randomized controlled trials directly compare the benefits and risks of PUS for preventing IUTI over conventional methods. The only randomized controlled trial compared simultaneous intraoperative with sequential PUS insertion in re-operative and complicated colorectal surgery. This trial demonstrated that the simultaneous insertion of stents significantly reduced the overall operative time by 19 min with no increased morbidity [







留言 (0)