Patient psychological responses to a PC diagnosis
FPC poses significant psychosocial challenges to the patient and his other family members. Persons diagnosed with FPC can have physical symptoms of pain, decreased appetite, and fatigue, accompanied by psychological reactions which include depression and anxiety [14]. Persons with PC have reported more anxiety, distress, and depression than those with other cancer types [15]. The frequent accompaniment of depression and anxiety with pancreatic cancer is not understood [16]. Feelings of depression may precede a diagnosis of PC, with the detection of depression occurring in a majority of persons with PC within six months of diagnosis [17]. It has been suggested that depression and anxiety may stem from biological, metabolic, or functional responses to the illness [16]. Czerw et al. [18] reported greater negative effects of anxiety and helplessness with less fighting spirit among persons with PC than other gastrointestinal cancers. In a large Delphi study of PC patients in treatment, patients prioritized four core psychosocial domains: overall quality of life, relationships with partners and family, satisfaction with providers, and fear of PC recurrence [19]. Information about the heritability of the cancer did not reach consensus as a priority among participants (≤ 60%) in that study.
The psychosocial impact of FPC on families
The discovery of PC is often devastating for individuals and families who may be blindsided by the diagnosis. PC in a family member can affect the lifestyle and daily habits of at-risk family members across generations. Family members can experience psychosocial distress because they are concerned about their health while simultaneously caring for family members suffering from PC symptoms and declining health. Family members may worry about the genetic risk for themselves and others [20] and have an increased risk perception for PC [1].
Family members fear of developing PC
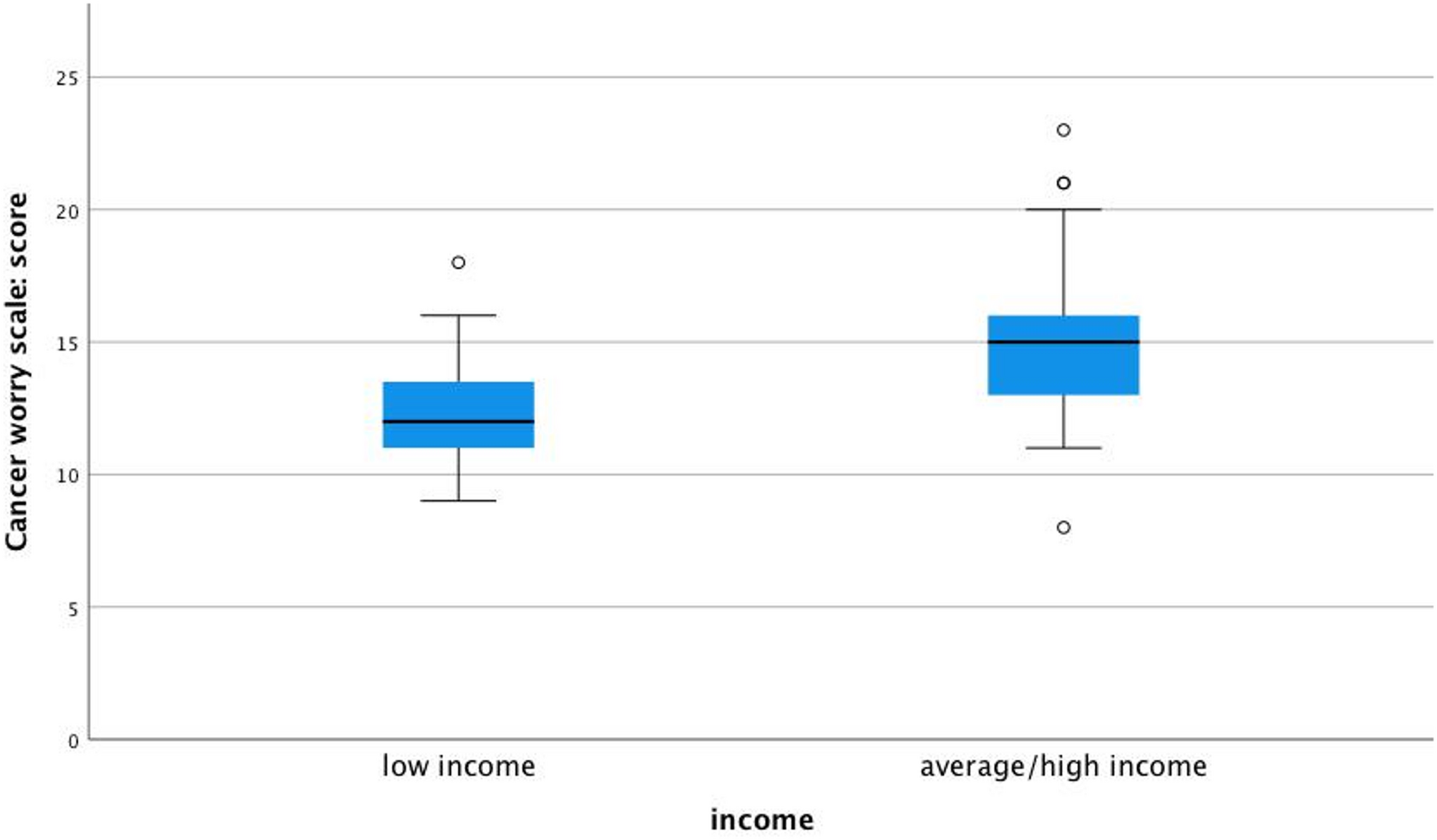
Fear can affect the psychological and social aspects of at-risk individuals. Underhill et al. surveyed patients at risk for developing FPC and found that approximately 58% reported they worried about developing PC anywhere from sometimes to all the time. Over half of the participants reported having some degree of worry about developing pancreatic cancer, and over 15% worried often or all the time [1]. This worry can occur throughout the caregiver’s life; however, it was greatest following caring for a family member with PC (within the last five years) or the recent death of family member from PC [1]. Breitkopf et al. found that 81% of people with a family history of FPC reported a degree of concern (anywhere from mild to extreme) in comparison to only 1% of the control group (those without a history of FPC) having concern about developing pancreatic cancer [2].
Researchers also recognized trends in the various times that patients with a history of FPC reported worry. Underhill et al. [1, 7] found that around 57% of participants said that they worried about developing pancreatic cancer when they are going in for screening tests, and around 58% of participants reported worrying when they are thinking about a loved one who has had pancreatic cancer. Other significant times of worry for participants included on their birthday or on the birthday of a loved one who has died from pancreatic cancer. Underhill et al. [7] show comparable results: participants in one-on-one interviews reported having the most “fear and worry” around screening and testing times, “anniversaries of loved ones’ deaths,” growing older, and having other friends surrounding them develop cancer. Underhill et al. [7] also found that when participants of this study thought about their future and dying, it was pancreatic cancer that they feared, not dying of any other cause.
These high percentages of worry show a need for family guidance and counseling when inherited pancreatic cancer is identified. Konings et al. [21] administered psychological screening questionnaires to family members at risk for FPC. The study found that participants with moderately high cancer worry should be thoroughly screened and counseled to improve psychosocial well-being [21]. In summary, people and families experiencing increased worry about developing PC require additional guidance and strategies for psychological support to decrease their concerns and improve their wellbeing.
Increased risk perception for those at risk for FPC
Those with a family history of FPC not only live with greater fear but also have a much higher perceived lifetime risk of developing pancreatic cancer [1]. In a study by Underhill et al. [1], most participants thought they had a 50% or higher risk of developing pancreatic cancer when the actual risk rarely exceeds 30% and can be as low as 4%. Although those with a family history of pancreatic cancer have an increased risk of developing the disease compared to the general population, they perceive their risk as much higher than the actual one [1]. Breitkopf et al. [2] found similar results when comparing those of the same gender, age, and race. When compared to a control group, 54% of those with a family history of FPC reported they were likely to develop pancreatic cancer at some point in their life. At the same time, only 6% of people without FPC reported a likelihood of having pancreatic cancer in the future [2].
Underhill et al. [7] and Konings et al. [21] found that the family experience of watching a family member ill with pancreatic cancer was highly correlated with inflated risk perceptions. Seeing a family member with the disease had a more significant impact on risk perception than testing positive for having a pathogenic variant associated with pancreatic cancer development. Although people knew they had a higher risk due to genetic mutations, their main reason for worrying was due to the diagnosis of a family member [7, 21]. This inflated risk perception of developing pancreatic cancer affects the lives of those with FPC and calls for greater assistance and supportive care for those diagnosed with FPC [7]. Such discrepancies between perceived and actual risk highlight the importance of advocacy and education programs for at-risk individuals.
Receptivity to screening and responses to surveillance for FPC
Persons at high risk for FPC may engage in long-term surveillance for early detection of FPC. Individuals more likely to undergo screening for pancreatic cancer had higher rates of cancer worry [2]. Breitkopf et al. [2] found that those with FPC were more receptive to endoscopic ultrasound screenings for pancreatic cancer than those without FPC (41% compared to 16%, respectively). Underhill et al. [7] reported that at-risk individuals were more likely to undergo less invasive screening tests. These individuals always worried about the outcome of their screening tests but still went through screening in hopes of identifying any cancerous changes early [7]. Of note, in a study by Maheu et al. [22], anxiety associated with participation in screening for FPC did not lead to general distress, increased risk perception, and cancer worry. In fact, cancer worry diminished over time which was attributed to counseling and screening activities [22]. O’Neill et al. [4] conducted a study to evaluate the effects of a short and long-term screening program using endoscopic ultrasound and or MRI for pancreatic cancer in a high-risk group (FPC/ BRCA2). Those with personal histories of cancer or positive BRCA2 mutations had increased worry of developing cancer at baseline. However, no negative impact appeared due to screening in the short term. Furthermore, long-term psychological benefits to screening were appreciated in lessening anxiety responses to screening, psychological consequences (emotional, social, and physical domains), and cancer worry [4]. Overbeek et al. [23] examined the burden of surveillance and noted that cancer worries increased during intensified surveillance (lesion identified or had surgery) but decreased with a return to regular surveillance schedules. Overall anxiety and depression measures were unchanged throughout, with quality of life scores in the months following surgery, scores for both physical and mental components were at comparable levels to the public at large [23]. In another study by Overbeek et al. [24], long-term surveillance of at-risk persons found ongoing engagement within the screening program was high.
Family psychosocial experiences related to FPC
Persons caring for family members with FPC or PC had increased psychosocial burdens related to their experiences of FPC and PC. Breitkopf et al. [2] found that the family experience with pancreatic cancer was the most significant factor related to increased worry. Pancreatic cancer has a lower survival rate than other cancers; therefore, caregivers experience more worry, suffering, guilt, and anticipatory grief as they watch their loved one deal with disease symptoms [20]. Sherman et al. [20] noted a number of salient categories in a qualitative study of caregivers of patients with advanced pancreatic cancer. These included crises related to the diagnosis of cancer, stressors of providing direct care, frustrations of interacting with medical personnel, financial burdens, the constriction of social life and loss of general pleasures in life. Caregivers reported long wait times at appointments, inconsistent medical advice, and sparse information or information overload as being some factors that impacted patient and caregiver experiences [20]. In some instances, study participants gained new insight into their personal strengths and were grateful for time spent with loved ones. However, other caregivers did not cope well and noted psychological withdrawal, stress, depression, and increased drinking and smoking, among other behaviors [20]. A coordinator to help navigate the health care system throughout the patient’s cancer journey could improve patient and family satisfaction with care. Similarly, Kim and Baek [25] reviewed the literature on PC families and found that the diagnosis fueled feelings of fear, stress, depression, anxiety, and helplessness, yet, in some instances, caregivers also reported positive coping mechanisms and enhanced experiences when caring for their loved ones.
Caregivers reported clinically significant levels of anxiety yet claimed better overall quality of life (physical and functional well-being) when compared with those in their care [26]. Age was a factor in this study, with increased anxiety and depression scores among younger (< 60 years) caregivers of persons with PC. A review by Chong et al. [27] revealed select consequences of caregiving included feelings of increased burden in managing a loved one’s symptoms, depression, and anxiety, affecting their quality of life. It also cited an unmet need for better navigation and communication within the health system [27]. Caregivers felt healthcare providers were insensitive, did not provide consistent advice, and provided either too much or too little information [27]. Protocols to guide patient-provider interactions may improve the patient’s and family’s overall satisfaction with care [27].
It is essential to identify individuals at risk for developing FPC and offer psychosocial support to them. Underhill et al. [7] explained that caring for those with FPC includes more than just identifying their risk. Care of these patients also needs to involve psychosocial support and understanding how the knowledge of an increased risk for developing pancreatic cancer can affect one’s life [7].
Lifestyle changes in at-risk subjects
People at elevated risk for FPC reported increased concern about their health [7]. At-risk individuals wanted to know what lifestyle changes they could make to decrease their risk. Improving their diet, exercising, and reducing tobacco and alcohol consumption were actions at-risk individuals believed could decrease their risk of developing pancreatic cancer. Although people reported wanting to improve their health, others took their increased risk for FPC as a sign to live their life to the fullest and felt it was not worth changing their lifestyle habits [7].



Comments (0)