
記住我
HIV testing has undergone significant transformations throughout the history of the HIV pandemic, and it has moved from a positive test result being a probable death sentence to routine testing being part of a broader prevention plan (Redoschi et al., 2017). Combined prevention starts with regular testing for sexually active people. Among key populations, such as men who have sex with men (MSM), the recommendation is annual testing, and for those involved in situations of greater risk exposure, HIV testing is indicated once every six months or more frequently. However, testing frequency recommendations should be targeted based on an assessment of individual characteristics and exposure risk level (DiNenno et al., 2017).
Regular testing has overall health benefits because early HIV diagnosis can reduce morbidity and mortality and transmission rates. However, the prevalence of HIV testing among MSM varies according to the estimation method and social and cultural context, ranging from 53.15% to 88.2% (Bhattacharjee et al., 2020; Liu et al., 2019; Nanin et al., 2020). A systematic review with meta-analysis identified that recent and regular testing is suboptimal (Liu et al., 2019), and in a sample of 1,657 Chinese MSM, 29.7% reported biannual testing (Hill et al., 2019).
Low adherence to regular testing may be related to different access barriers faced by MSM: stigma; fear of false results; concern for secrecy; fear of disclosing sexual orientation; limited access to health services; not knowing the place where the test is performed; not having health insurance; fear of the outcome; engaging in safe sex practices; and the perception of low risk (Horridge et al., 2019; Zhang et al., 2021). Barriers are varied and may be more evident depending on the culture and social conditions of MSM. For barriers related to confidentiality, both related to the test result itself and sexual orientation, there are alternatives such as the self-test that can be performed in a place with the desired level of privacy, which includes being performed at home. Evidence indicates that self-testing contributed to the increased frequency of HIV testing among high-risk MSM (Katz et al., 2018). Other studies conducted with younger MSM identified fear of disclosing sexual orientation to parents, association of infection with death, issues related to communication with health professionals, and even the test result itself as additional concerns (Dowson et al., 2012; Schwarcz et al., 2011; Song et al., 2011; Wei et al., 2014; Wong et al., 2012).
Knowledge about barriers to accessing health services faced by MSM in Brazil is scarce, and there is a need for more information on the subject to guide actions that improve access to health services, with testing and timely initiation of treatment. In this sense, valid and reliable instruments can be support tools to assess the barriers to HIV testing experienced by Brazilian MSM. Scales to monitor barriers to HIV testing are scarce worldwide. The Barriers to HIV Testing Scale-Karolinska version (Wiklander et al., 2015) is a scale developed from a preexisting instrument (Awad et al., 2004) and allows the identification of different types of barriers to HIV testing, presenting itself as an option for cultural adaptation and validation for application in the Brazilian reality. Thus, the aim of this study was to culturally adapt and evaluate the psychometric properties of the Barriers to HIV testing scale-Karolinska version among Brazilian MSM.
Methods DesignThis is an instrument adaptation, methodological study. Developed in six steps, as shown in Figure 1, the Barriers to HIV Testing Scale-Karolinska version (Wiklander et al., 2015) was translated from English to Brazilian Portuguese, adapted, and validated with a sample of 1,290 MSM.
 Figure 1.:
Figure 1.: Flowchart of the scale adaptation and validation process.
The instrument adaptation process is described in the following six steps:
Step 1—TranslationAfter authorization from the original author of the scale, two certified and independent translators translated the scale from English into Brazilian Portuguese.
Step 2—Assessment by the evaluators committeeA committee of evaluators met to assess the two translated versions of the scale and find a consensus version. This committee was composed of five evaluators—four experts on the subject and one member of the MSM population. All evaluators were proficient in both English and Portuguese and were all native Brazilians. Furthermore, the evaluators needed to meet at least one of the following criteria to be included: having clinical experience with people living with HIV, being a researcher in the field of HIV, having defended a thesis/dissertation in the field of HIV, or belonging to the population of interest.
This in-person meeting lasted for 65 minutes. During this meeting, the committee evaluated the instrument item by item and selected the translated item that was most related to the Brazilian culture and health context.
Step 3—Back-translationThen, back-translation was performed by two, independent, certified translators who were different from the translators who performed the initial English to Brazilian Portuguese translations. Two versions in English were obtained, and a meeting was held between the five researchers from the committee of evaluators to obtain a consensual version. The original author of the scale had contact with the back-translated version and agreed with the version presented.
Step 4—Semantic analysis of itemsThis is the first step in which a sample of participants was recruited for the adaptation and validation process. The objective of this stage was to verify the comprehensibility of all the scale items by the participants who constituted the study population. Data collection for this stage took place from February 11, 2020, to February 19, 2020. Men who have sex with men were selected for semantic analysis through two social media platforms—Instagram and WhatsApp. Text messages, containing an invitation to participate, were posted on each social media platform. If individuals agreed to participate, an online questionnaire was sent; this included an online free and informed consent form. The procedure used to collect data in this stage was sending the invitation and the link through the online form to participate. The online questionnaire contained four sections: 1:free and informed consent form; 2: closed and open questions about the sociodemographic and clinical characterization of the participants; 3: questions about the assessment of the scale; and 4: semantic analysis for each item.
In total, 51 invitations were sent. Two participants did not complete the answers and therefore were excluded. In the end, 49 MSM participated in the semantic analysis. Participants were selected considering their education levels, measured according to the number of years of study completed. Invitations were purposely sent to MSM with differing levels of education.
Step 5—PretestAfter the adaptation process, the final Brazilian Portuguese version of the Barriers to HIV Testing Scale-Karolinska version was tested in a sample of MSM with the purpose of evaluating the performance of data collection in virtual environments. Data collection for this stage took place from March 10, 2020, to March 25, 2020. Fifty-three MSM participated in the pretest. Men who have sex with men were selected through intentional sampling, a nonprobabilistic sampling method (Hair et al., 2009), by means of the availability of the questionnaire link on Instagram.
Step 6—Assessment of psychometric properties Study sampleData collection for the analysis of psychometric properties took place between the April 1, 2020 and May 19, 2020. The first response was received on April 1, 2020, and the last on May 10, 2020. Participant recruitment was done through the internet, through an online questionnaire built on the SurveyMonkey® platform. Inclusion criteria were as follows: being 18 years or older; identifying as a man; having Brazilian nationality (native or naturalized Brazilians); having access to the internet; having had sex with another man at least once in their life; and being without HIV/unknown (already tested and/or never tested for HIV) or newly diagnosed with HIV (<6 months).
The questionnaire link was published on different social networks: Instagram, Twitter, Facebook, and Grindr. The invitation message to participate in the research contained information about the research, the research objectives, and the inclusion criteria of the participants. A total of 1,830 people accessed the questionnaire link, and 1,298 answered the complete questionnaire with no data missing, which included all items in the scale. The response completion rate was 70.92%, and the average response time was 7 min. Of the 1,298 participants, eight were excluded for not meeting the preestablished inclusion criteria, which produced a final sample size of 1,290 for the psychometric analysis stage. This sample size is suitable for psychometric analyses in which authors recommend a minimum of 10 responses per item (Hair et al., 2009).
Data Analysis Characterization of participantsDescriptive statistics were used to analyze the following variables: sociodemographic characterization such as gender identity (cisgender man, transgender man, intergender, other); sexual orientation (gay, heterosexual, bisexual, pansexual, asexual, other); age in full years; region of the country (North, Northeast, Midwest, South and Southeast); skin color (white, black, brown, yellow, do not wish to declare, other); education (no education or <1 year of study, incomplete primary education, complete primary education, incomplete secondary education, complete secondary education, incomplete higher education, complete higher education, specialization, master's, doctorate); work status (formal, informal, unemployed, retired/pensioner, student); family income (<1 minimum wage, 1–2 minimum wages, 3–4 minimum wages, 5–6 minimum wages, 7 or more minimum wages, no income); and marital status (single, married, stable/living together, divorced, separated).
The skin color of the Brazilian population is self-declared, that is, the person is asked how he defines himself in relation to the color of his skin, according to the Brazilian Institute of Geography and Statistics. The minimum wage in Brazil was R$1,039, and the average Brazilian income was R$1,450 (IBGE, 2020)
ReliabilityThe reliability of the adapted version of the scale was assessed through the analysis of internal consistency using Cronbach alpha coefficient. Values range from 0 to 1, and values above 0.7 are considered acceptable (Hair et al., 2009).
Construct validityThe total sample of 1,290 participants was divided in two using an SPSS software tool for random division of cases; this was done to allow for two independent samples in conducting the factor analyses. The process resulted in two random samples, each corresponding to approximately 50% of the cases. The methodological procedure of dividing a sample into two different samples, at random, is recommended when there are large samples, as stated by Hair et al. (2009), and this resource has already been used by other authors (Todd et al., 2020). The sample for the exploratory factor analysis (EFA) consisted of 649 MSM, and the sample for the confirmatory factor analysis (CFA) was composed of 641 MSM. The two samples showed statistical differences when comparing the two groups in relation to a score calculated from the mean of the sum of the scale values.
Exploratory factor analysisThe EFA was performed to verify the behavior of the variables and the factorial structure of the scale. All assumptions for this type of analysis were verified. The matrix of correlations between the variables in which the variables were expected to be correlated was observed, which was confirmed. All correlations were statistically significant (p < .5). Two other tests were performed to observe the convenience of applying the factorial model: the Bartlett sphericity test and the Kaiser–Meyer–Olkin (KMO) measure of sample adequacy.
The KMO interpretation is that the closer it gets to 1, the more the perfect prediction of each variable is determined by the other variables. Values below 0.50 indicate that the factors found cannot satisfactorily describe the variations in the original data (Corrar et al., 2007), and items that did not load at 0.50 level on any factor were omitted in the results. For Bartlett test of sphericity, the p value should be observed, which is significant at p <.001 (Hair et al., 2009). Observing the eigenvalue criterion for determining the number of factors, only factor solutions with eigenvalues above 1 are considered. This solution is based on the Kaiser criterion (Kaiser test) or latent root criterion (Corrar et al., 2007).
Factor extraction was performed using principal components and oblimin rotation. Based on the Kaiser criterion, a number of factors were defined (Hair et al., 2009). The commonalities of each variable were also observed, and the acceptable level of explanation must be higher than 0.5 (Hair et al., 2009).
Floor and ceiling effects were also analyzed; floor effect being the percentage of participants who scored their responses at a lower level, and the ceiling effect being the percentage of participants who scored their responses at a higher level (Bennett et al., 2002). No changes were made after EFA, and thus, the final version of the scale was named.
Confirmatory factor analysisConfirmatory factor analysis was performed after extracting the factors to assess the stability of the factor model results and the degree of generalizability of the results. The CFA is essential because only through this is it possible to describe whether the data structure is representative (Hair et al., 2009).
The assumptions for this type of analysis were respected: normal distribution of sample data, which was verified by means of univariate asymmetry (skewness) and univariate flattening or kurtosis (kurtosis). Values greater than three for skewness and greater than 10 for kurtosis were considered to violate this assumption and indicate that the estimation of the model is inadequate (Kline, 2005).
For this analysis, the maximum likelihood method was used. A total of four factors were considered. Adjustment measures were considered for estimating the model: absolute fit measures, incremental fit measures, and parsimonious fit measures. The various adjustment measures, each with their respective particularities and values, must be evaluated together for the acceptance of a final model. Isolated value analyses should not be considered.
Adjustment measures Reference values Absolute fit measures Chi square (χ2) p > .05 Degrees of freedom (GL): χ2/GL (Kline, 2005). χ2/GL<3 Goodness of fit index (GFI) (Lisboa et al., 2012). GFI > 0.90 Root-mean-square error of approximation (RMSEA) (Hair et al., 2009). RMSEA < 0.08 Incremental adjustment measures Tucker–Lewis index (TLI) (Hair et al., 2009). TLI ≥ 0.90 Normed fit index (NFI) (Hair et al., 2009). NFI ≥ 0.90 Comparative fit index (CFI) (Hair et al., 2009). CFI ≥ 0.90 Incremental fit index (IFI) (Hu & Bentler, 1999). IFI ≥ 0.95 Parsimonious fit measures Parcimonious normed fit index (PNFI) (Hair et al., 2009) PNFI = 0.06–0.09 Parcimonious goodness fit index (PGFI) (Mulaik et al., 1989) PGFI ≅ 0.5The validity of the scale was assessed as the final stage of quality analysis. Composite reliability (CC) was used to verify the convergent validity. Values greater than 0.7 were considered satisfactory (CC > 0.7; Hair et al., 2009). The discriminant validity was verified using the heterotrait–monotrait ratio of correlations (HTMT) criterion (Henseler et al., 2015); the parameter is that the result of the HTMT verification is less than 0.85 if taken as a rigorous measure or less than 0.9 if taken as a more liberal measure (Henseler et al., 2015).
Ethical aspectsThe research project was approved by the Research Ethics Committee (CEP) of the Nursing School of Ribeirão Preto under opinion no. 3.172.445 and CAAE no. 06609319.0.0000.5393. All participants gave their free and informed consent in writing. The anonymity of the participants was guaranteed. Data were stored on the SurveyMonkey platform, during the data collection, in a private database accessed only by the main researcher.
ResultsA total of 1,392 MSM from the five regions of Brazil participated in the study: 49 from the semantic analysis; 53 from the pretest; 1,290 from the assessment of psychometric properties (649 from the EFA and 641 from the CFA).
PretestFifty-three MSM participated in this stage. The majority identified themselves as cisgender male (n = 48; 90.6%), gay (n = 47; 88.7%), from Piauí (n = 42; 79.2%), of brown skin color (n = 25; 44.6%), with higher education incomplete (n = 21; 39.6%), with formal work (n = 22; 41.5%), single (n = 45; 84.9%), without a steady partner (n = 31; 58.5%), used alcohol (n = 43; 81.1%), did not use tobacco (n = 46; 86.8%), had a sexual partner in the past three months (n = 22; 41.5%), and the most frequent sexual practice was the receptive anal position (passive) (n = 21; 39.6%). Participants responded to all items on the scale, with no loss of responses on any of the items.
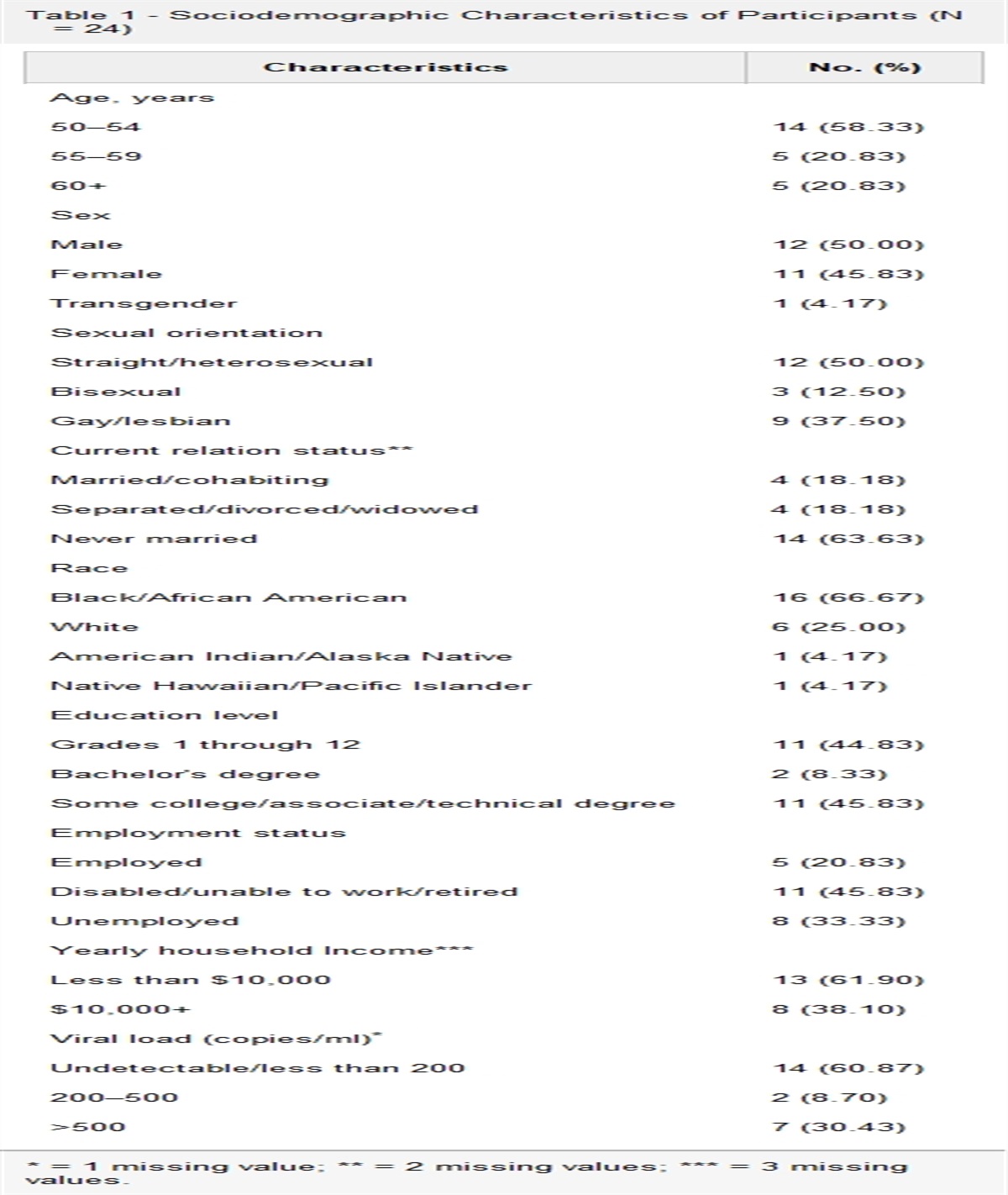
Exploratory Factor Analysis Results of sociodemographic characterizationA total of 649 MSM participated in this stage, 584 were cisgender men (90%), 547 identified as gay (84.3%), 448 aged 18–29 years (69%), 317 identified as White (48.8%), 194 with higher education incomplete (29.9%), 312 entered the formal labor market (48.1%), 224 with family income of up to two minimum wages (34.5%), and 550 were single (84.7%), as shown in Table 1.
Table 1. - Sociodemographic Characterization of the EFA Stage Participants (n = 649) Variables n (%) Gender identity Cisgender man 584 (90.0) Transgender man 8 (1.2) Intergender 8 (1.2) Other 49 (7.6) Sexual orientation Gay 547 (84.3) Heterosexual 6 (0.9) Bisexual 71 (10.9) Pansexual 16 (2.5) Asexual 2 (0.3) Other 7 (1.1) Age (full years) 18–29 448 (69.0) 30–39 159 (24.5) 40–49 29 (4.5) 50–59 13 (2) 60 years and more — Country region Northeast 291 (44.83) Southeast 221 (34.05) South 75 (11.55) Midwest 46 (7.08) North 16 (2.46) Skin color White 317 (48.8) Black 75 (11.6) Brown 241 (37.1) Yellow 9 (1.4) Not declared 6 (0.9) Other 1 (0.2) Education No education or <1 year of study — Incomplete elementary school 4 (0.6) Complete primary education 6 (0.9) Incomplete high school 21 (3.2) Complete high school 91 (14.0) Incomplete university education 194 (29.9) Complete higher education 173 (26.7) Specialization 109 (16.8) Master's degree 36 (5.5) Doctorate degree 15 (2.3) Job Formal work 312 (48.1) Informal work 85 (13.1) Unemployed 84 (12.9) Retired/pensioner 3 (0.5) Student 165 (25.4) Family incomea Less than 1 minimum wage 67 (10.3) Between 1 and 2 minimum wages 224 (34.5) Between 3 and 4 minimum wages 171 (26.3) Between 5 and 6 minimum wages 76 (11.7) 7 or more minimum wages 96 (14.8) No income 15 (2.3) Marital status Not married 550 (84.7) Married 25 (3.9) Stable union 70 (10.8) Divorced 2 (0.3) Widower 2 (0.3)Note. Ribeirão Preto, SP (2020). EFA = exploratory factor analysis.
aMinimum salary in Brazil at the time of data collection: R$1,035.00.
The overall reliability of the scale using Cronbach alpha was 0.89.
Exploratory Factor AnalysisThe visual examination of the matrix allowed the verification that all variables were correlated and with statistically significant relationships. To verify the convenience of applying the factorial model, Bartlett sphericity tests and the KMO sample adequacy measure were performed, as shown in Table 2.
Table 2. - Bartlett Sphericity Tests and the Kaiser–Meyer–Olkin Measure of Sample Adequacy Kaiser–Meyer–Olkin Sample Adequacy Measure 0.896 Bartlett sphericity test Approximate Chi-square 5,105.426 DF 153 Sig. (p value) .000Note. Ribeirão Preto, SP (2020). df = degree of freedom; Sig. = significance or p value.
The solution defined was that of four factors, 62.09% of the variance was explained by the factorial solution. No item had high factor loadings in more than one factor.
From the factorial solution, the factors were named according to the denomination received in the original scale, except for the last one, observing the change in the grouping order: F1: personal consequences; F2: structural barriers; F3: confidentiality; and F4: economic consequences and individual concerns. The first factor is responsible for 36.66% of the variance, with an eigenvalue of 6.599. This factor is consistent with the interpretation of personal consequences, incorporating item 13 “I was afraid of losing my family,” originally allocated to another factor. The second factor is responsible for 11.01% of the variance, with an eigenvalue of 1.982 and comprises the structural barriers. The third factor accounts for 7.76% of the variance, with an eigenvalue of 1.398. The factor is consistent with the interpretation of confidentiality, incorporating item 5 “I didn't like the people at the test site.” The fourth factor accounts for 6.66% of the variance, with an eigenvalue of 1.199. The factor comprises economic consequences such as “health insurance” (item 10) and “employment” (item 11) and individual concerns such as “the test result” (item 9) and “no cure” (item 8), illustrated in Table 3.
Table 3. - Factorial Loads and Commonalities (H2) Based on the Principal Component Extraction Method and Oblimin Rotation (Standard Matrix) on the Barriers to HIV Testing Scale-Karolinska Version Scale Items Item F1 F2 F3 F4 H2 Item 16 .833 .604 Item 15 .800 .631 Item 14 .759 .710 Item 18 .717 .558 Item 12 .661 .586 Item 13 .618 .639 Item 17 .563 .592 Item 4 .824 .695 Item 1 .746 .634 Item 2 .745 .605 Item 3 .692 .480 Item 7 .877 .790 Item 6 .812 .739 Item 5 .699 .567 Item 8 .823 .661 Item 9 .732 .553 Item 10 .694 .569 Item 11 .407 .564Note. Ribeirão Preto, SP (2020). Name of the factors: F1, personal consequences; F2, structural barriers; F3, confidentiality; F4, economic consequences and individual concerns; items assigned to factor from highest load.
Means, SDs and floor and ceiling effects are shown in Table 4. Floor and ceiling effects have moderate results. The internal consistency of all scales showed excellent levels, with all Cronbach alpha > 0.7.
Table 4. - Descriptive Statistics for the Barriers to HIV Testing Scale-Karolinska Version; Number of Scale Items, Mean, SD; Floor/Ceiling Effect and Cronbach's Alpha (α) Scalea Number of items Mean DP Effect Floor/Ceiling (%)b α Personal consequences 7 1.085 .63 36.49/44.95 .886 Structural barriers 4 0.908 .57 41.33/32.16 .767 Confidentiality 3 0.985 .76 39.60/38.11 .756 Economic consequences and social concerns 4 0.685 .22 58.36/26.81 .746Note. Ribeirão Preto, SP (2020).
aPossible range for all scales: 0–2, with higher levels indicating more barriers.
bPercentage of ratings on the lowest/highest possible score.
A total of 641 MSM participated in the CFA stage. As for the sociodemographic characterization, 578 were cisgender men (90.2%), 539 were gay (84.1%), 438 aged 18–29 years (68.3%), 284 were White (44.3%), 198 with incomplete higher education (30.9%), 309 entered the formal labor market (48.2%), 193 with a family income of up to two minimum wages (30.1%), and 524 were single (81.7%), according to Table 5.
Table 5. - Sociodemographic Characterization of CFA Stage Participants (n = 641) Variables N (%) Gender identity Cisgender man 578 (90.2) Transgender man 5 (0.8) Intergender 3 (0.5) Other 55 (8.6) Sexual orientation Gay 539 (84.1) Heterosexual 7 (1.1) Bissexual 72 (11.2) Pansexual 17 (2.7) Asexual 2 (0.3) Other 4 (0.6) Age (full years) 18–29 438 (68.3) 30–39 167 (26.1) 40–49 27 (4.2) 50–59 7 (1.1) 60 years and more 2 (0.3) Country region Northeast 268 (41.80) Southeast 233 (36.34) South 61 (9.51) Midwest 56 (8.7) North 23 (3.58) Skin color White 284 (44.3) Black 76 (11.9) Brown 265 (41.3) Yellow 4 (0.6) Not declared 9 (1.4) Other 3 (0.5) Education No education or <1 year of study 1 (0.2) Incomplete elementary school 2 (0.3) Complete primary education 5 (0.8) Incomplete high school 17 (2.7) Complete high school 87 (13.6) University education incomplete 198 (30.9) Complete higher education
留言 (0)