
Remember me





What is known about the topic?
Urinary retention is common in perinatal women. The incidence of postpartum urinary retention in Taiwan is 7.78%, but this condition is usually diagnosed late, often leading to serious sequelae, including infection, chronic dysuria, and renal failure. Despite the known significance of bladder management during the perinatal period, all the care provided by most healthcare professionals does not meet the requirements of established guidelines.What does this article add?
A baseline audit and two follow-up audit cycles were used to identify barriers to bladder management and conduct ongoing monitoring of perinatal care. Implementing the clinical practice guidelines for improving perinatal bladder care reduced the rate of urinary retention, catheterization frequency, and first and second voiding time after delivery. It also increased awareness of this common condition. Long-term and individual education methods are indispensable strategies for improving women's knowledge about bladder care. IntroductionPostpartum urinary retention is a common disorder and is defined as the absence of the ability to urinate spontaneously more than 6 h after vaginal delivery or after the removal of a urinary catheter, or as having a postvoid residual volume of ≥150 ml after spontaneous urination.1 The reported incidence varies considerably, from 1.7% to 17.9%.2 The estimated incidence of this condition in Taiwan is 7.78%, and it is often diagnosed late.3
Postpartum urinary retention is likely a multifactorial disorder. It can occur as a result of anatomical changes that occur during pregnancy and/or vaginal delivery; prolonged labor, especially in the second stage; assisted or instrumented labor; episiotomy; or regional analgesia.4 Cesarean section also involves anesthesia, and continuous or intermittent urinary catheterization is necessary to assist women in emptying their bladder during and after delivery.5
Any misdiagnosis or delay in diagnosis of persistent urinary retention can be detrimental because bladder over-distension may cause irreversible bladder damage,6 which in turn, can lead to serious sequelae, including infection, chronic dysuria, and renal failure.7 It is also associated with an increased risk of postpartum depression, longer hospitalization, and increased medical costs.8
Given that the importance of protecting perinatal women with bladder function is undeniable, a meta-analysis has shown that urinary tract infection rates did not differ between women receiving intermittent or continuous catheterization while in labor under epidural analgesia,9 but bladder function may normalize earlier with intermittent catheterization compared with transurethral indwelling catheterization.10 The Royal College of Nursing's bladder management guidelines recommend recording the timing and volume of the first void following birth and the times at which the indwelling urinary catheter was inserted and removed.11 If the increased postvoid residual urine volume is unresolved for more than seven days, it may lead to persistent voiding disorders.12 The goal of bladder management during the intrapartum and postpartum periods, therefore, is to assess the patient for signs of bladder retention, detect any deviations from normal, and manage them in a timely manner to avoid complications of postpartum urinary dysfunction.13 To date, there have been few evidence-based studies that deal with the optimization of care for perinatal bladder problems.14 Despite the known significance of bladder management during the perinatal period, there is no consensus on the necessity for routine assessments to be included in the care provided by healthcare professionals. There is also a lack of formal and evidence-based education programs in the intrapartum and postpartum wards. This highlights a need to establish better management strategies for bladder issues in hospitals to avoid voiding dysfunction in perinatal women.
Effective nursing leadership ensures that appropriate staffing and other resources are available to achieve high-quality care and optimal patient outcomes.15 Cummings et al.16 found that relationship-focused nursing leadership practices encourage positive outcomes in the nursing workforce, including job satisfaction, retention, and well-being. Relational leadership is considered a more effective method of organizing and implementing leadership to meet organizational challenges in the twenty-first century.17 It encourages the practice of caring for colleagues, enabling others to act, acknowledging and learning from one's mistakes, and being emotionally authentic.17 Therefore, incorporating the concept of relational leadership into practical implementation projects can help leaders to engage actively in work groups, maintain positive operational relationships, emphasize partnerships with the staff, and facilitate the inclusion of different perspectives and opinions.18
ObjectivesThe aim of this project was to use relational leadership theory, which integrates inclusion, empowerment, purposefulness, ethical behavior, and process orientation, to improve the practice of bladder management for intrapartum and postpartum women to prevent urinary disorders. The success of the project was evaluated using evidence-based criteria. The specific objectives were as follows:
(1) Determine current compliance with evidence-based criteria regarding bladder management; (2) Design and implement strategies to improve compliance with best practices in bladder management in intrapartum and postpartum women; (3) Reduce intrapartum and postpartum urinary disorders (e.g., urinary retention, frequency of catheterization, postpartum time to voiding); (4) Improve compliance with evidence-based criteria for bladder management. MethodsThis evidence-based implementation project used the JBI Practical Application of Clinical Evidence System (JBI PACES),19 and the implementation was planned using the Getting Research into Practice (GRiP) audit and feedback tool. Using the JBI PACES and GRiP framework, we collected and compared data, conducted audits, identified gaps and barriers, and developed a final implementation plan. The project involved seven phases of activity, which took place between 1 October 2021 and 31 March 2022. It consists of seven phases including: identification of practice area, engagement of change agents, assessment of context and readiness to change, review practice using evidence-based audit criteria, implement changes to practice using GRiP, re-assessment of practice through a follow-up audit, and consider sustainability of the project.20
Ethical considerationsThis project was registered with the research hospital in Taiwan as a quality improvement activity. It did not need formal ethical approval because it was not within the scope of Taiwan's Human Subjects Research Act. The data collected were anonymized, with all identifying parameters removed.
Phase 1: Identify the practice areaThe project was implemented in a ward with 20 beds and 18 nursing staff at a maternity hospital located in northern Taiwan; the birth rate in this region was approximately 900 per 153 000 newborns in 2021. On average, two or three nurses are scheduled for duty during each morning, afternoon, or night shift, and they are responsible for nursing and care during the delivery and postpartum periods. The incidence of postpartum urinary retention at this birth center was approximately 10% in October 2021. The hospital director, hospital executive, and medical center resident were the leaders of this hospital. We held meetings with them to persuade them to adopt this implementation project. Ultimately, the agreement was finalized and permission was granted to run the project at this birth center.
Phase 2: Engagement of change agentsThe project team comprised five people: two faculty members, a nurse midwife, a supervisor nurse, and a head nurse. The two faculty members, who were employed at a local nursing university, developed and coordinated the project and were responsible for designing and elaborating the protocol, conducting the training program, and organizing data collection. The nurse midwife helped to build rapport with the staff in order to facilitate the implementation and monitoring of the new bladder management practices in the ward. The nursing supervisor and head nurse empowered the ward staff members and worked with their strengths to implement the new care practices.
The project team used relational leadership theory17 to emphasize the relationships between staff members and considered everyone's viewpoint and experiences when making decisions. While the leader ultimately made the final decision, all perspectives were weighed carefully to develop the GRiP and implementation strategies for improving the quality of care in the management of bladder issues in perinatal women. The team also used communication skills to invite all nurses to participate in identifying the problems, barriers, and resources related to the care of perinatal women.
Phase 3: Assess context and readiness to changeWe selected hospitalized perinatal women aged over 18 years whose babies had no medical complications. In the baseline audit, 70 women were enrolled, and in each of the subsequent follow-up audits, 30 women were enrolled. The 18 nurses in the ward were all involved in the baseline and follow-up audits. However, there was a large range in the nurses’ level of experience; their time working ranged from 2 months to 21.42 years (average: 6.88 years).
The women who gave birth in this birth center were predominantly healthy, and exceptions who developed medical complications were rare. They routinely visited the outpatient clinic for postpartum follow-up after discharge. The JBI-recommended bladder management practice in intrapartum and postpartum women includes 18 criteria (Appendix I, Supplemental Digital Content, https://links.lww.com/IJEBH/A113). The hospital implemented the following audits, which included keeping routine records of the first two voids after birth and using a urinary catheter until at least 12 h after a cesarean section. The hospital did not use a bladder scanner as part of their clinical care, so we excluded eight audit criteria. We used 10 audit criteria for monitoring this project (Table 1).
Table 1 - Audit criteria, sample size, and methods used to evaluate compliance with best practice guidelines Audit criteria Sample Method used to measure compliance (%) with best practice 01 During the intrapartum period, the woman receives information regarding bladder management Baseline: 70 womenAll team members were involved in developing the work observation table, checklist, and questionnaires for the baseline and follow-up audits, as well as the bladder management package. As a group, they had a clear purpose, and a meeting was held at the beginning of the study and fortnightly thereafter to discuss strategies, challenges, and progress.
The project audit criteria (Table 1) were developed based on a JBI evidence summary.21 The audit assessed the practices of all 18 nurses and the care and education that was provided to the patients. When women presented to the birth center, an auditor shared written project information with them and invited them to participate in the program.
A baseline audit to assess the current bladder management practices of the ward was conducted based on the JBI PACES program. The team training, which was held in the first 2 weeks of October 2021, involved all the project team members, and the JBI best practice standards were introduced. Next, the baseline audit, which would identify any gaps in the current practice, was planned. During the planning meeting, the team members discussed the necessary sample size and the approach to each auditing standard recommended by JBI. Items were then identified for conducting the audits. The work observation table and questionnaires for checking compliance with the audit criteria were designed to assess whether the patients were receiving adequate education from the nurses. The accuracy of the bladder management procedures was assessed by evaluating the nurses’ performance based on a medical record checklist and other data collection methods. This assessment was conducted to ensure that the nurses competently applied their nursing knowledge and skills.
Phase 5: Implement changes to practice using Getting Research into PracticeThis phase was implemented from 16 October to 6 December 2021. Our team used relational leadership theory to promote positive outcomes in the nursing workforce and with respect to other related organizational issues. This was done by presenting the results of the preimplementation baseline audit to the ward staff, thereby revolutionizing their experience of the work they do. A previous study had found that in Chinese society, using relational leadership styles in teams may improve team performance and foster nurses’ innovation capacity.22 Relationship-oriented leadership emphasizes making people feel part of the team and highlights the shared values of the people in an organization. When using this leadership style, supervisors are concerned about the emotions and reactions of their subordinates and therefore offer more support and assistance than they might otherwise.23 In our project, implementing relational leadership theory involved two steps. The first was to provide an opportunity to work with the healthcare team and educators to learn bladder management strategies while building relationships within their practice environment, which supports individual learning and group resilience. In the second step, the supervisor had to identify any barriers that hindered the nurses’ compliance with best practices. Afterward, the team worked together to achieve its shared vision and goals. The key barrier identified was a lack of formal education among the nurses regarding assessment tools for bladder management and the lack of educational materials for patients.
A training workshop was conducted to address these barriers. Team members had fortnightly discussions regarding the analysis of the baseline data, identification of obstacles and factors of resistance, formulation of the GRiP strategy, development of audit tools and checklists, and the design of feasible strategies for overcoming the obstacles. The GRiP strategy was implemented for 7 weeks.
Phase 6: Re-assessment of practice through a follow-up auditThe project included two follow-up audits, using the same evidence-based audit criteria that were used in the baseline audit. The first audit after implementation was conducted from 7 December 2021 to 31 January 2022. The second follow-up audit was conducted from 1 February 2022 to 31 March 2022, and each follow-up audit involved 30 women and 18 nurses. Data were collected by two members of the project team.
Phase 7: Consider sustainability of the projectBecause there was a wide range in the level of experience of the nurses, all team members decided that the time frame for the repeated audits after changes should be conducted every 6 months. This would allow prompt follow-up and taking corrective action based on audit findings.
Results Baseline auditThe highest levels of compliance were for criteria 1 (37%; “During the intrapartum period, the woman receives information regarding bladder management”), 2 (50%; “Postpartum, the woman receives information regarding bladder management”), and 8 (50%; “After birth, the woman has two spontaneous voids, with normal bladder sensation and a volume of 200 ml or more.”) (Fig. 1). The medical records revealed that the nursing staff exhibited low compliance with seven audit criteria: 3 (“Previous history of urinary incontinence, bladder injury, or urinary retention is documented”) (0%); 4 (“During the intrapartum period, the woman is encouraged to void regularly, usually every 3 hours”) (7%); 5 (“During the intrapartum period, fluid intake and output are documented”) (0%); 6 (“During the intrapartum period, the woman is assessed for urinary retention if unable to pass urine within 6 hours, and appropriate treatment is initiated”) (28%); 7 (“After birth, the woman attempts to void every 3 to 4 hours, even if she has lost the sensation to void”) (0%); 9 (“After birth and where the woman has not voided for 4 to 6 hours, conservative bladder management is provided, including advice on fluid intake, how to empty the bladder, double bladder emptying, and adherence to a strict fluid input and output chart”) (17%); and 10 (“After birth and where the woman has not passed urine within 6 hours, she is assessed for urinary retention and dehydration”) (0%). In addition, the nurse examination revealed that the nurses exhibited low compliance with audit criteria 6, 9, and 10. None of the nurses had been formally trained in assessing patients for urinary retention.
 Figure 1:
Figure 1: Baseline audit compliance rates (%)
Getting Research into Practice strategiesThree barriers that prevented compliance with best practices were identified (Table 2). The first and second barriers were the absence of routine guidelines for bladder care during labor and postpartum, and the lack of formal education about bladder assessment (e.g., bladder distension and signs of dehydration). To address these issues, a course workshop was conducted. All the nursing staff at the birth center had to undergo this training. The two faculty members on the project team developed this program, which included educational materials on the prevention of urinary retention and working procedures for bladder care. The head nurse encouraged the ward staff to practice the skills together and used the teach-back method throughout the process. Finally, the nurse midwife determined the completion rate of the educational goals in the training program. The third barrier was a lack of detailed written evidence-based educational materials at the birth center to share with both the nurses and the patients during the intrapartum stage; the information provided to the women was thus inconsistent, informal, and dependent on what each individual nurse had to offer. There was therefore an urgent need to produce an evidence-based educational handout for intrapartum and postpartum women (Appendix II, Supplemental Digital Content, https://links.lww.com/IJEBH/A114).
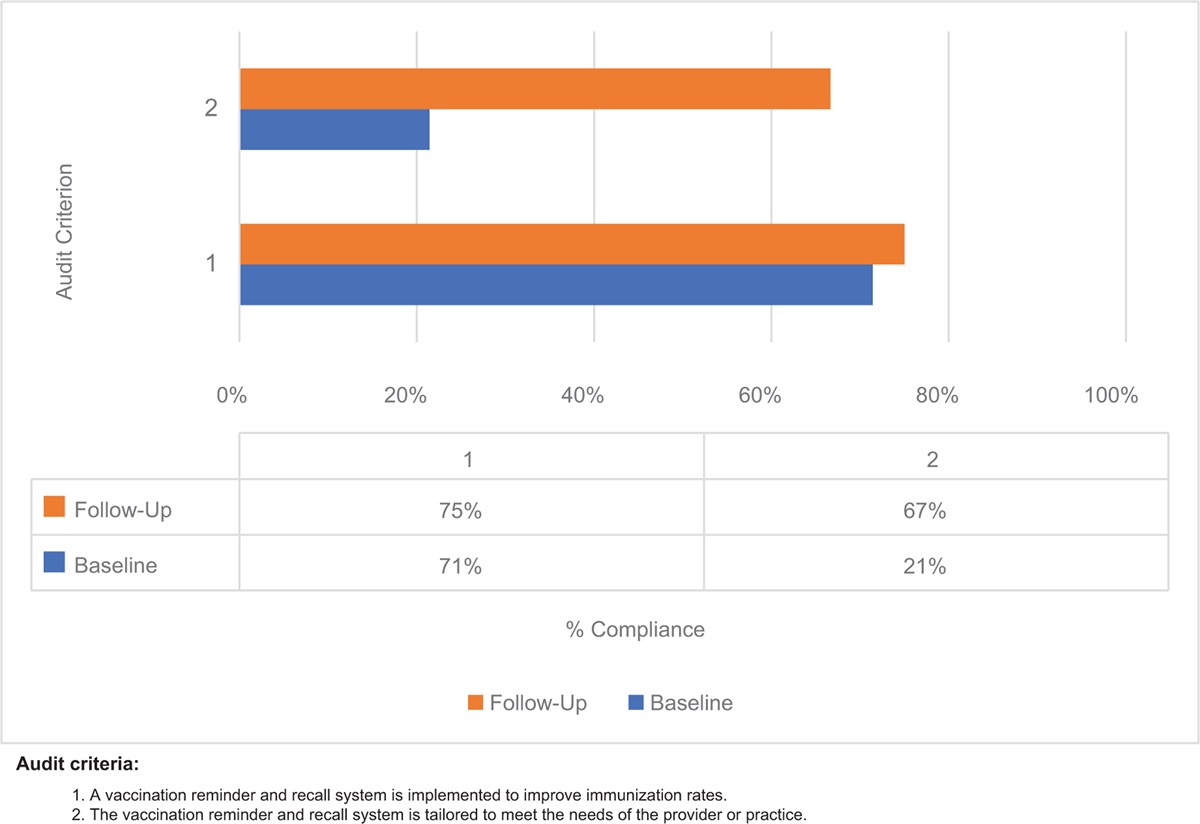
Table 2 - Getting Research into Practice (GRiP) analysis of the barriers to practice, the strategies and resources used to overcome these barriers, and the outcomes observed Barriers Strategy Resources Outcomes Lack of specialized education teams, workflow, and training provided to the nurses on bladder assessment • Used PowerPoint slides to educate nurses on bladder assessmentIn the postimplementation audit, the 18 nurses exhibited better compliance with recommended practice. The results of the first follow-up implementation audit were compared with those of the baseline audit (Fig. 2). Based on criteria 1 and 2, patients were educated about bladder care protocols, and the audit revealed 90% and 93% compliance rates, respectively. This was a huge improvement from the initial 37% and 50% compliance rates, respectively. Compliance for criteria 3, 4, 5, 7, and 8, which pertained to initial and ongoing bladder care, was 100%, 100%, 90%, 100%, and 97%, respectively, revealing good ongoing compliance. Compliance for criteria 6, 9, and 10, which pertained to bladder assessment and management, increased to 100%.
 Figure 2:
Figure 2: Compliance with best practice audit criteria in follow-up audits 1 and 2 compared with the baseline audit (%)
The nurses started using working procedures to improve their adherence to the evidence-based standards for bladder management. As a result, the time to first postpartum voiding and between the first and the second voiding decreased from 5.51 and 4.01 h to 4.75 and 3.44 h, respectively. However, the incidence of postpartum urinary retention increased from 9.09% to 15.91%. In addition, the frequency of intrapartum intermittent catheterization during labor increased from 53.44% to 61.36% (Table 3). The patients received intrapartum intermittent catheterization more frequently than at the baseline audit. Further analysis revealed that the frequency of catheterization increased with nurses who had less than 2 years of experience. Thus, using bedside-teaching methods and repeating the training on how to assess urinary retention may be useful, and the teach-back method can be used to confirm what the nurses have learned.
Table 3 - Compliance rates at the baseline and follow-up audits Baseline audit Follow-up audit 1 Follow-up audit 2 Postpartum urinary retention 9.09% 15.91% 8.51% Intrapartum intermittent catheterization rate 53.44% 61.36% 38.30% Postpartum time to first void for patients with NVD 5.51 h 4.75 h 2.32 h Postpartum time to second void for patients with NVD 4.01 h 3.44 h 2.29 h Postpartum time to first void for CS patients 4.01 h 2.74 h 2.86 h Postpartum time to second void for CS patients 3.82 h 3.15 h 2.65 hCS, cesarean section; NVD, normal vaginal delivery.
The second follow-up audit aimed to determine whether the positive outcomes achieved in the first follow-up audit were maintained. The compliance rates for all the criteria were over 97%, similarly to the first follow-up audit (Fig. 2). Further, the intrapartum intermittent catheterization rate dropped to 38.30% and the incidence of postpartum urinary retention decreased to 8.51% and these results were well documented in the medical records for assessment and care. This indicated that the nurses had become familiar with and competent in implementing the working procedures for improving compliance with the evidence-based guidelines for bladder management.
DiscussionAccording to the main objective of this project, we analyzed the compliance of the nursing staff at a maternity hospital with evidence-based practice recommendations concerning bladder management in intrapartum and postpartum women. The baseline audit revealed a gap between the hospital's existing care practices and the best practices recommended based on available evidence. After the barriers to practice had been identified, three strategies for improvement were implemented. First, a bladder assessment and care education package was developed and implemented. Second, specific working procedures were compiled and documented. Third, an educational manual on bladder care was created for the staff and patients. The second follow-up audit revealed substantial improvements in compliance with best practice.
The strategies used, which were based on relational leadership theory, contributed to the success of this implementation project. First, in the baseline audit, barriers were identified based on observations, medical records, and a review of ward routines, guidelines, and health education leaflets. In addition to establishing the bladder care manual and workflow according to the hospital attributes and ward characteristics, we identified the common need of the nursing staff for role fulfillment. The supervisor and the head nurse emphasized the partnership between management and staff and clearly explained the clinical problems encountered after analyzing the situation. Positive peer influence was thus used to enable sustained implementation. The goal for team leaders was to encourage the professional growth of the staff through current evidence-based implementation procedures and to help the organization to achieve a common goal.
The second success of this project was the improvement in the nurses’ knowledge of and skill in the assessment of urinary retention. The nursing staff attended training and education workshops to learn about perinatal bladder care. The course lecturer was a nurse midwife with more than 10 years of experience who had completed the JBI Evidence-Based Clinical Fellowship Program. The course was conducted face-to-face, and a course DVD was also produced, which the staff could watch at their convenience. Further, a work team was formed to assist with answering questions while the program was in progress. Of the 18 staff members, 6 had <2 years of nursing experience, and of these, 4 had <1 year of experience. The knowledge and technical competence of novice nurses are often insufficient to prepare them for the transition to clinical situations.24 As the first follow-up audit revealed, patients cared for by the less experienced staff members had higher frequencies of catheterization during the intrapartum period than those attended by the more experienced nurses. On recognizing this, the head nurse responded by first positively recognizing the efforts of these nurses in striving to provide the best care possible based on the guidelines and their personal assessments of the patients. Later, the team discussed this issue and decided to repeat the training on bladder assessment for novice nurses, using bedside teaching methods.
The third success of this project was the creation of the educational handout on bladder care. In addition to the printed handout, the patients were provided with an electronic QR code and offered individualized postpartum virtual consulting services. In this way, they could obtain information on bladder care at any time, helping to avoid urinary retention. Price and Reichert 25 conducted a comparative study of care modalities and found that relative to task-centered care, continuous primary care until 2 weeks after hospital discharge resulted in higher care satisfaction rates and reduced the incidence of postpartum urinary retention. This continuous bladder care strategy assists perinatal women to practice preventive methods that require a prolonged implementation period. Finally, ward events were conducted to share a focused message with clinicians and hospital directors regarding the bladder management care guidelines and the need for a bladder scanner, and positive peer influence was used to encourage sustained implementation.
Sustainable relational leadership provides an ongoing process of reflective practice and collective meaning-making among team members.26 This project considered challenges in perinatal bladder care from a nursing perspective, and helped intrapartum and postpartum women to reduce their incidence of urinary disorders and hospitals to improve their compliance with the evidence-based criteria for bladder management. In addition, it may have helped nurses to reduce their workload relating to urinary problems in perinatal women and give birth center staff a sense of achievement. All the team members decided to conduct follow-up audits every 6 months and continue to improve the quality of care they provided, based on the audit results.
To ensure practical feasibility, this project was conducted over a limited timeframe, with a limited sample size, and in only one hospital. The project concerned only the period when the patients were hospitalized during their perinatal phase, so its effect on the rate of infection and associated comorbidities that arise later is unknown. A future direction for this project is to conduct additional follow-up audits with cross-departmental collaboration to improve these strategies and examine how these changes can be sustained over time.
ConclusionOur findings show that compliance increased after we implemented the evidence-based practice guidelines concerning bladder management for intrapartum and postpartum women. This was achieved via educational strategies to improve the assessment of bladder management and improvements in electronic workflow. This project resulted in reductions in the rate of urinary retention, frequency of catheterization, and time to voiding after delivery. Continued monitoring and audits can ensure the sustainability of this change in perinatal care practice to ensure that it benefits postpartum women. The use of a relational leadership framework to enhance the knowledge and skills of the nursing staff was critical to this project's success.
AcknowledgmentsWe would like to thank the women who participated in this study. We are extremely grateful to the monthly journal club discussions held by the Taiwan Evidence-Based Practice Center and the Taiwan Holistic Care Evidence Implementation Center, a JBI Affiliated Center, for their support during data processing.
Funding: This study was supported by the Ministry of Science and Technology, Taiwan (grant nos.: MOST 110-2314-B-227-002-MY2 and 111-2314-B-227-002-MY2). The funding bodies played no role in designing the study; collecting, analyzing, and interpreting the data; or writing the manuscript.
Availability of data and material: All data pertaining to this study are included in this article and its supplementary information files.
Author contributions: Study design: L.L.C, M.L.G., and W.L.P. Data collection: L.L.C. and C.H.W. Data analysis: M.L.G., C.H.W., and W.L.P. Manuscript writing and revisions for important intellectual content: L.L.C, M.L.G., W.L.P., S.F.T., and P.F.M.
Conflicts of interestThere are no conflicts of interest.
References 1. Kekre AN, Vijayanand S, Dasgupta R, Kekre N. Postpartum urinary retention after vaginal delivery. Int J Gynaecol Obstet 2011; 112:112–115. 2. Stanley AY, Conner BT. Implementing a clinical practice guideline to manage postpartum urinary retention. J Nurs Care Qual 2015; 30:175–180. 3. Lin S-Y, Gau M-L. Postpartum voiding dysfunction and urinary retention. J Midwifery (Taiwan) 2018; 60:1–11. 4. Li Q, Zhu S, Xiao X. The risk factors of postpartum urinary retention after vaginal delivery: a systematic review. Int J Nurs Sci 2020; 7:484–492. 5. Gyhagen M, Åkervall S, Milsom I. Clustering of pelvic floor disorders 20 years after one vaginal or one cesarean birth. Int Urogynecol J 2015; 26:1115–1121. 6. Ain QU, Shetty N, Supriya K. Postpartum urinary retention and its associated obstetric risk factors among women undergoing vaginal delivery in tertiary care hospital. J Gynecol Obstet Hum Reprod 2021; 50:101837. 7. Barba M, Frigerio M, Manodoro S, Bernasconi DP, Cola A, Palmieri S, et al. Postpartum urinary retention: absolute risk prediction model. Low Urin Tract Symptoms 2021; 13:257–263. 8. Avondstondt AM, Hidalgo RJ, Salamon CG. Intrapartum risk factors for postpartum urinary retention: a case-control study. Int Urogynecol J 2020; 31:2395–2398. 9. Li M, Xing X, Yao L, Wang X, He W, Wang M, et al. The effect of bladder catheterization on the incidence of urinary tract infection in laboring women with epidural analgesia: a meta-analysis of randomized controlled trials. Int Urogynecol J 2019; 30:1419–1427. 10. Mulder FEM, Hakvoort RA, de Bruin JP, van der Post JAM, Roovers J-PWR. Comparison of clean intermittent and transurethral indwelling catheterization for the treatment of overt urinary retention after vaginal delivery: a multicentre randomized controlled clinical trial. Int Urogynecol J 2018; 29:1281–1287. 12. Mohr S, Raio L, Gobrecht-Keller U, Imboden S, Mueller MD, Kuhn A. Postpartum urinary retention: what are the sequelae? A long-term study and review of the literature. Int Urogynecol J 2022; 33:1601–1608. 13. Rantell A, Veit-Rubin N, Giarenis I, Khullar V, Abrams P, Cardozo L. Recommendations and future research initiative to optimize bladder management in pregnancy and childbirth International Consultation on Incontinence – Research Society 2018. Neurourol Urodyn 2019; 38 (S5):S104–S110. 14. Miller S, Abalos E, Chamillard M, Ciapponi A, Colaci D, Comandé D, et al. Beyond too little, too late and too much, too soon: a pathway towards evidence-based, respectful maternity care worldwide. Lancet 2016; 388:2176–2192. 15. Wong CA, Cummings GG, Ducharme L. The relationship between nursing leadership and patient outcomes: a systematic review update. J Nurs Manage 2013; 21:709–724. 16. Cummings GG, Tate K, Lee S, Wong CA, Paananen T, Micaroni SPM, et al. Leadership styles and outcome patterns for the nursing workforce and work environment: a systematic review. Int J Nurs Stud 2018; 85:19–60. 17. Routledge, Clarke N. Relational leadership: theory, practice and development. 2018. 18. Wiley-Blackwell, Middleton R, Cardiff S, Manley K, Dewar B. Manley K, Wilson V, Øye C. Leadership relationships. International practice development in health an
Comments (0)