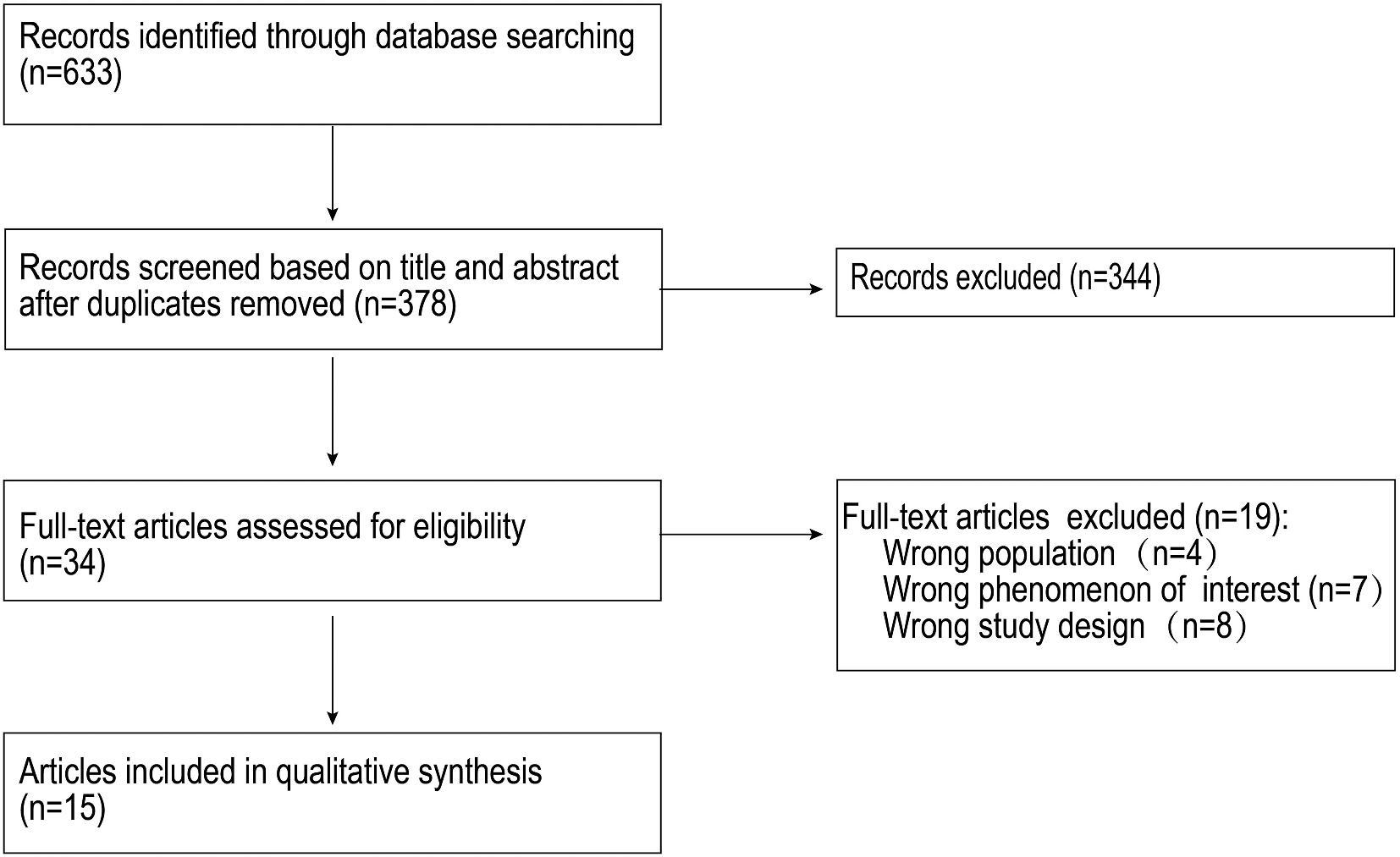
We conducted a total of 46 in-depth interviews with caregivers of children aged 6–23 months. Table 1 presents the characteristics of mother-child pairs in rural and urban Central Java, Indonesia. The mean age of the rural and urban mothers was 29.7 and 29.4 years, respectively. Most rural mothers completed junior high school (87.4%), while half of the urban mothers completed senior high school (50.0%). Around six per cent of rural mothers worked outside the house, whereas one-third of urban mothers were employed. Approximately 56% of children in both settings were female, with the mean age of children being 13 months in rural areas and 14 months in urban areas.
Table 1 Characteristics of mothers and children aged 6–23 months in rural and urban areas of Central Java, Indonesia
The main themes that emerged in this study included facilitators and barriers to sustaining breastfeeding beyond six months and factors of formula feeding. Table 2 describes the themes, sub-themes, and illustrative quotes of our study participants.
Table 2 Themes and sub-themes related to breastfeeding continuation at the individual and setting levels in rural and urban Central Java, Indonesia
Theme 1: facilitators of breastfeeding continuation
All rural mothers still practised breastfeeding on the interview date. In the urban setting, around half of the mothers maintained breastfeeding (n = 16). Among rural and urban mothers who continued breastfeeding, we identified several factors that positively influenced its sustainability, such as breastfeeding attitude, breastfeeding knowledge, previous breastfeeding experience, and problem-solving strategies to extend breastfeeding duration.
Attitudes toward breastfeeding
Generally, mothers regarded breast milk as the best nourishment for infants and young children. They often compared its superiority over formula milk. For example, a mother said, “Breastmilk is the best (food) for a child.” (an urban mother aged 38 years). Similarly, an urban grandmother said, “Breastmilk is the number one priority for babies” (an urban grandmother). Some rural mothers also viewed breastfeeding as the child’s right to provide for at least two years as stated by a mother, “Because breastfeeding is an obligation of a mother. It is the child’s right.” (a rural mother aged 26 years).
Breastfeeding knowledge
Most mothers were well-informed about breastfeeding benefits for their children. They agreed that breastmilk could prevent infections and optimise growth and brain development in both settings. A rural mother summarised, “To be healthy, not getting sick easily…” (a rural mother aged 21 years). Nonetheless, we also found that some rural mothers were unsure about other breastfeeding advantages by stating “I don’t understand”, “What else?”, “What is it?”, “Is that correct?”. Meanwhile, urban mothers generally be more specific when describing breastfeeding benefits. For example, “Breastmilk can improve her immune system and for her cognitive development.“ (an urban mother aged 31 years).
We noted that rural mothers considered an economic benefit of breastfeeding that we did not find in the urban setting. For example, a mother said, “I breastfeed my child so that she can grow healthy and normal… and reduce our (financial) burden. It (the information) is from the midwife and the primary health centre’s staff. I think the advice was correct.” (a rural mother aged 37 years).
Most urban mothers and some rural mothers believed that breastfeeding should continue for two years. For example, a mother said, “(I will breastfeed him) Maybe for two years. At two years, breastfeeding will be stopped.” (an urban mother aged 20 years). However, breastfeeding should last as long as the child wants it for a few rural mothers. For example, a mother explained, “Just like her sister (who was breastfed until three years), I will breastfeed her as long as she wants… I will not force weaning her.” (a rural mother aged 31 years).
Previous breastfeeding experience
Rural and urban mothers reflected on the positive breastfeeding experience of them or their peers, making them feel confident about sustaining breastfeeding. A mother said, “Just like my first child. I produced breastmilk immediately after birth. Now he is still breastfed. No formula, but breast milk. (I will breastfeed him) Maybe for two years. At two years, breastfeeding will be stopped. His brother was (breastfed) for more than two years.” (an urban mother aged 20 years). Yet a rural mother who planned to breastfeed for more than two years described her experience with her first child, “I weaned her sister after three years. After she reached 2.5 years, I breastfed her rarely.” (a rural mother aged 31 years).
Mothers might learn not only breastfeeding practices based on positive experiences but also negative ones. Urban mothers’ regretful feelings in the past encouraged them not to repeat such experiences. A mother said, “It was my first child that I gave him formula milk… When I was thinking about him, I felt pity for him. For my second child, she is breastfed.” (an urban mother aged 26 years).
Problem-solving strategies to continue breastfeeding
Both rural and urban mothers who sustained breastfeeding took several actions when faced with breastfeeding challenges. For instance, some urban and rural mothers consumed green vegetables and fish, increased their meal portion size, and used galactagogues to boost milk production. One mother said, “I took the capsule and herbal drink because the milk production was not smooth… I meant I could not produce much.” (an urban mother aged 24 years).
Another effort used by mothers was to quit their job. One rural and one urban mother decided to leave their work for breastfeeding for up to two years. A rural mother who used to be a labourer described how her husband’s persuasion convinced her to decide: “When I was still working, my husband encouraged me to quit. I should only work after my daughter aged two years old.” (a rural mother aged 27 years).
Breastfeeding education
Both rural and urban mothers mostly received breastfeeding education from health providers. In rural, the village midwife was a highly respected health professional working who delivered infant and young child nutrition, including breastfeeding. A mother explained her adherence to breastfeeding recommendations: “I followed the suggestion from the midwife. It is better to provide breastmilk than formula milk. It is healthier.” (a rural mother aged 39 years).
A rural midwife explained about community education groups held in her working areas:
“Mothers practised appropriate breastfeeding because they had joined Pregnant Women and Toddler Classes. During these classes, there was information about breastfeeding, so they knew about breastfeeding importance. (I told them that) Breast milk is more convenient, cheaper, and more hygienic than formula.” (a rural midwife).
In urban areas, we found more varied resources for breastfeeding education, including nutritionists, local midwives, general practitioners, and university students who conducted community services.
“I received breastfeeding information since I was pregnant. It was during my antenatal visit to the primary health centre. There is also information from Posyandu. In Posyandu, the educators are kader and the midwife.” (an urban mother aged 27 years).
“Health staff from the primary health centre gave routine education on child nutrition. That included breastfeeding. There were also many university students who gave education on breastfeeding.“ (an urban kader).
Theme 2: barriers to breastfeeding continuation
All of our rural participants continued to breastfeed their children until the interview date. In contrast, nearly half of the urban mothers had stopped breastfeeding their young children, which mainly occurred below twelve months. There was a range of explanations for breastfeeding discontinuation among urban mothers. At the maternal factors, these barriers included perceptions of inadequate milk supply and perceptions of child hunger. Child factors were child biting and breastmilk rejection. Maternal employment also influenced mothers to terminate breastfeeding.
Since all rural mothers were breastfeeding until the interview date, the following are barriers to sustaining breastfeeding among urban mothers:
Perceptions of inadequate milk supply and child hunger
The most common reason for breastfeeding cessation in urban settings was maternal perception of milk supply. Urban mothers interpreted child fussiness and high appetite as hunger cues because breastmilk could no longer satisfy their children.
“My breastmilk was decreased a lot. So, it is like she was always fussy when she drank less.” (an urban mother aged 30 years).
“…(My) breast milk was not sufficient. He (my son) kept crying. When I pumped, I was very stressed. At first, I gave him both breastmilk and formula because he drank a lot. Well, now only formula milk since… twelve months.” (an urban mother aged 31 years).
“Many mothers also complained about breast pain… and that their breast milk did not come out anymore.” (an urban kader).
Child biting and rejection
A few urban mothers reported that they stopped breastfeeding because they could not endure the pain caused by child biting, making their nipples sore and cracked. For example, a mother explained, “He has so many teeth already. He suckled until my nipples ripped. It hurt, so I didn’t breastfeed him. At the same time, I weaned him.” (an urban mother aged 24 years).
Many mothers also mentioned breast milk refusal by their children. While some were unsure about the underlying factor, some perceived that breast milk rejection might be caused by low milk production, child hunger, illness, and bottle-feeding preference. They narrated:
“She refused… refused by herself. She did not like direct breastfeeding but asked for a bottle (feeding). I produced breastmilk little by little. I only produced from the left side, and the right side was not coming out. Later, the breast milk did not come out at all.” (an urban mother aged 23 years).
Community views on breastfeeding up to two years
Following the previous national recommendation, it was a general knowledge among rural and urban communities and health workers that breastfeeding should be up to two years, not beyond. This view might lead to reduced breastfeeding duration for two years only. A mother said, “I know that breastfeeding should be up to two years.“ (an urban mother aged 29 years). However, since our participants were mothers with children aged 6–23 months, we could not explore breastfeeding continuation beyond this period.
During the data collection, health workers still delivered breastfeeding for up to two years messages to the community.
“For infants above six months, we always encourage mothers to continue breastfeeding them until two years.“ (an urban nutritionist).
“Previously, many mothers provided breast milk until their children grew up, such as the above two years… even until their children entered a kindergarten school. But new young mothers were already educated. We educated them during Toddler and Pregnant Women Class, so they do not practice it now. They only offered breast milk for two years.” (a rural midwife).
Maternal employment
One-third of urban mothers were employed. Some supplemented breastfeeding with formula feeding, while others gave up breastfeeding altogether. Few working mothers expressed and stored breastmilk, but only one succeeded in breastfeeding continuation up to the interview date. A mother who eventually discontinued breastfeeding narrated:
“I used to store my breast milk in the freezer. Then, I could not because it was hard to squeeze (breast milk hand expression). If I squeezed, it (breast milk) was only a little. I had the pumping tool, Maam… but the milk did not come out. But if she suckled, the milk supply became a lot. I also ate a lot, not a little. Maybe it is because I breastfed her every day in the past. Now I do not breastfeed her during the day.” (an urban mother aged 28 years).
“The inhibiting factor was maternal employment because they left their children at home while they were working, although some mothers pumped their breasts.” (an urban kader).
Conversely, most rural mothers were housewives. Some of them related being with their children at home make breastfeeding possible. For example, a mother said, “I do not work outside, so I do not give formula milk, but breast milk.” (a rural mother aged 31 years). However, we did not ask specifically how the workload outside and inside the home might affect the mother’s flexibility in breastfeeding.
Theme 3: factors influencing formula feeding
We found that formula feeding in rural areas was not as common as in urban areas. Even though few rural mothers had provided formula milk during early infancy before their breast milk came out or due to low breastmilk supply, they quit it because their milk supply was abundant, formula milk rejection by the children, or not suggested by health workers.
“I had bought formula, but I did not use it. He (my son) did not like it, and if I forced him, he would vomit.” (a rural mother aged 36 years).
“My husband advised me to give formula milk so that her (my daughter’s) body weight increased. But, when she was sick and we brought her to the clinic, the doctor said that her body weight was fine. So, I didn’t give her formula (anymore).“ (a rural mother aged 29 years).
“I followed the suggestion from the midwife. It is better to provide breastmilk than formula milk. It is healthier.” (a rural mother aged 39 years).
We did not ask specifically about formula milk advertisements. However, the rural midwife described that the newest regulation did not allow health workers to promote breastmilk substitutes. On some occasions (e.g., when the children were severely malnourished), the midwife and village kader would visit mothers at their houses to check their feeding practices. The midwife said that some mothers would hide the formula milk when they visited. These findings suggested that rural health workers did not encourage formula milk and that rural mothers knew formula feeding was not advisable.
Only one rural mother offered formula milk as breastmilk supplementation due to the perceived low milk supply and working outside the house. Conversely, formula feeding was a widespread practice among urban mothers. While few urban mothers had started to introduce bottle feeding before six months, more mothers provided formula milk as the child grew older. For all mothers who provided their children with formula milk, we asked the reasons behind such practices. The influencing factors were perceptions of low breast milk supply, perceived formula milk benefits, and maternal employment.
Perceptions of inadequate milk supply
Maternal perception of breast milk insufficiency was the most reported reason to offer formula feeding, either to supplement or substitute breast milk. Some of these mothers had started to offer formula milk before six months.
“My breastmilk is only a little, so I also give him formula. Previously, I told my mother that my breastmilk is lacking and asked her opinion about formula feeding. She just agreed.“ (a rural mother aged 26 years).
“She was not satisfied because my breastmilk didn’t come out. (She) Always cried… then I gave her formula.” (an urban mother aged 23 years).
“As far as I know, some mothers already provided their babies with formula milk before six months… it’s because they thought their breast milk is inadequate, then their babies are less satisfied.“ (a rural kader).
“I am sure that all of the mothers here wanted to breastfeed their babies fully. Some mothers had issues like their breastmilk did not come out at all. But, mostly… the problem was low breastmilk supply. So, they gave formula milk to their babies.“ (an urban kader).
Perceived formula milk benefits
Some urban mothers offered formula feeding to their children because they thought formula milk had several benefits linked to their children’s growth and development. For some mothers, they decided to give formula milk by themselves, while others were supported by their husbands or mother.
“My husband advised me to give formula milk so that her (my daughter’s) body weight increased. But, when she was sick and we brought her to the clinic, the doctor said that her body weight was fine. So, I didn’t give her formula (anymore).“ (a rural mother aged 29 years).
“If I only gave her breast milk, I would feel pity for her. Her body weight often did not increase but kept decreasing. So, I gave her the formula to not look too weak like that. Her development might also be slowed (if she only consumed breast milk).” (an urban mother aged 47 years).
“His mother gave him formula milk when he was three months old. I just followed her. It was when his body weight did not increase, so she gave her formula milk. Then, his body weight increased 100 grams… little by little.“ (an urban grandmother).
Maternal employment
All urban mothers who discontinued breastfeeding altogether provided their children with formula milk. Most mothers who still maintained breastfeeding also offered formula feeding as a supplement. They managed the feeding schedule based on their daily routine.
“My son consumes formula milk, especially when I am working outside.“ (a rural mother aged 26 years).
“When her mother works, like today… her mother has morning shift, so he is with me… I give him formula milk. He will get breastmilk when his mother comes home.“ (a rural grandmother).
“I breastfed him since he was born, but now I also give him formula milk because I left him for work. It (Formula feeding) was started when he was four months. I tried to store my milk, but I felt pity for his grandmother. His grandmother was already busy with (managing) her retail shop, while at the same time caring for my child… But, when I am home, I fully breastfeed him.“ (an urban mother aged 27 years).
“Now still breastmilk. At day, she had formula milk… at night, she had breastmilk.” (an urban grandmother).

留言 (0)