
記住我





A cross-sectional study utilized a designed questionnaire that was given to mothers to collect data from March to May 2021. One core member of the research team in each city was responsible for supervising data collection. Each core member then trained and supervised all data collectors and routinely checked all completed maternal questionnaires. Data collectors at each site were responsible for distributing questionnaires to eligible mothers and collecting completed questionnaires.
Study settingVietnam is the third most populous country in Southeast Asia with over 97 million people in 2020, with nearly one-third of that population living in rural areas. In 2019, there were 24.9 million women of reproductive age (15–49 years) and approximately 1.6 million live births. At that time, the mortality rate for children under the age of 5 was 20 per 1000 live births, the infant mortality rate was 16 per 1000 live births, and the neonatal mortality was 10 per 1000 live births [23].
This study was conducted in two cities in Central and North Vietnam. The first city, Da Nang, is one of the most important port cities in Central Vietnam with a population of over 1.1 million in 2020. The city has a total natural land area of around 1283 km2, of which 241 km2 are urban districts and it has the highest urbanization ratio among provinces in Vietnam, with nearly 90% of the population living in urban areas. The neonatal mortality in Da Nang was 4 per 1000 live births. The second study city, Thai Nguyen City, is located in the centre of the Northern region which is close to Ha Noi, the capital city. Thai Nguyen City has a natural land area of about 223 km2 and a population of approximately 340,000 in 2019. In total, there are 32 CHCs in Thai Nguyen City and 56 CHCs in Da Nang City.
There were eight selected sites (CHC) in Thai Nguyen City. Four of the selected CHCs were located in communities categorized as urban areas and four CHCs were in areas categorized as semi-urban (ward) areas. In Da Nang City, ten CHCs were selected and were located in the urban areas and six CHCs were located in the surrounding semi-urban communities. Our sampling method was based on our ability to get data collection approval from the CHCs as the study was conducted during the COVID-19 pandemic.
ParticipantsMothers whose infants were aged greater than 6 months to 30 months who presented to the CHCs for routine vaccination were invited to join the study. In Vietnam, the national Expanded Programme on Immunization is integrated into the services of CHCs. All children in Vietnam are required to be fully immunized according to the Expanded Programme on Immunization. The pediatric vaccination participation rate is greater than 95% in the country. Only mothers of singletons were included. After maternal verbal informed consent was given to participate in the study, each mother received a self-administered questionnaire.
Questionnaire and data collectionOur study questionnaire was based both on a literature review of breastfeeding patterns [16, 24,25,26,27] and from consulting with maternal-infant clinical specialists who have experience in infant breastfeeding and EENC practices. The full questionnaire consisted of 39 self-administered questions to each mother and the questions asked were to help determine potential factors associated with breastfeeding in the first six months of the infants life including: (1) maternal socio-demographic information (age, education level); (2) place of residence; (3) parity; (4) age of infant when mother returned to work after maternity leave; (5) complications during pregnancy and at delivery; (6) infant characteristics (sex, birth weight, mode of delivery, hospital of birth, complication at birth); (7) skin-to-skin contact practice after birth (no, < 15 min, 15–90 min, > 90 min); (8) having first breastfeed during skin-to-skin contact; (9) breastfeeding methods (direct or mixed between direct and expressed breast milk); (10) breastfeeding difficulties; 11) level of exposure to infant formula advertising during pregnancy (“often”, “sometimes”, “seldom”); 12) receiving breastfeeding counselling; 13) intention of feeding pattern during pregnancy; 14) knowledge on definition and duration of exclusive breastfeeding; and 15) breastfeeding support in the workplace. These variables were chosen based on the review of existing publications and current practice on EENC in Vietnam [13, 21, 25,26,27]. Our study questionnaire has not been previously utilized or published.
The cut-off values of the duration of skin-to-skin contact were based on the dividing values to assess how long after birth the baby received first breastfeeding in the WHO checklist used to interview postpartum mothers [28]. A draft questionnaire was sent to ten mothers to test for confusion about any questions and were then asked for any suggestions or changes to the draft questionnaire. After receiving feedback from the initial pilot testing, the questionnaire was revised, and questions were rearranged for better clarity when being answered.
The primary outcome of interest was the prevalence of exclusive infant breastfeeding for the first six months of life. As defined by the WHO, exclusive infant breastfeeding is an infant being fed only breast milk as the sole source of nutrition. No other liquids, solids, or water is consumed by the infants, except vitamins, minerals, and medicines [29]. Exclusive infant breastfeeding can either be direct breastfeeding or expressed breast milk feeding. In our study, we asked mothers what their infant’s primary source of nutrition was when they were under six months of age with the options including breast milk (yes / no), infant formula (yes / no), colostrum milk powder (yes / no). Other supplements were also asked about including water (yes / no), vitamin / medicine (yes / no), fruit juice / honey (yes / no), and complementary foods (yes / no). Exclusive breastfeeding was identified based on the answer “yes” for the breast milk and “no” for infant formula, colostrum milk powder, water, fruit juice / honey, and complementary foods.
Printed questionnaires were distributed to eligible mothers while at the CHCs. For mothers who were holding their infants and required help, the data collectors read the questionnaire and recorded their answers. The collectors sat down in the same direction as the mothers so that they could still view the questionnaire. Our study followed A Consensus-Based Checklist for Reporting of Survey Studies (CROSS) [30].
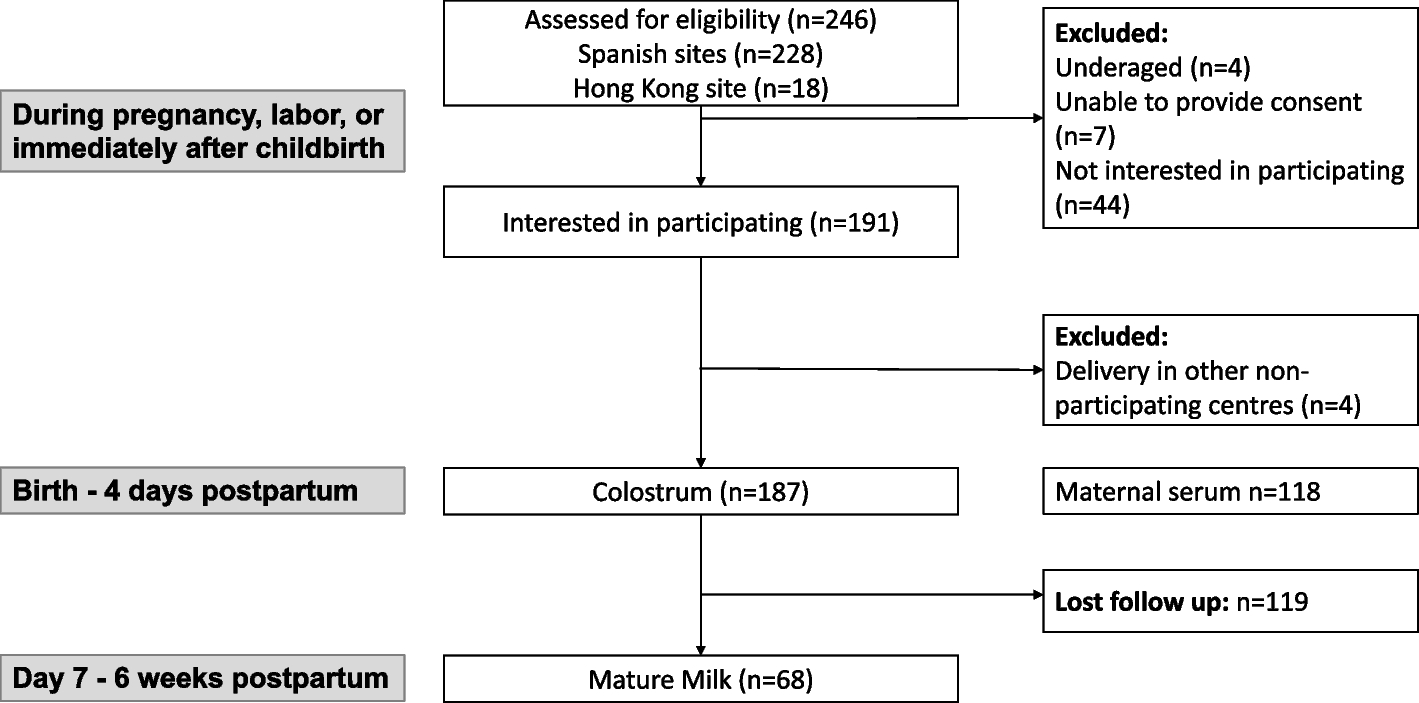
Sampling technique and sample size determinationThe sample size was calculated by using the formula of estimating prevalence with the following assumptions: Prevalence of exclusive breastfeeding was 19.6% which was taken from the National Institute of Nutrition [31], with 95% confidence interval, precision error of 2.5%, and 5% non-response rate. The required sample size was 1018 participants. Finally, a total of 1072 mothers were included in the analysis. The detailed sampling procedure is described in Fig. 1.
Fig. 1
Sampling procedure and study participants
Data quality control and data analysisAll completed questionnaires were carefully checked before entering data in EpiData version 3.1. Data entry forms were designed to minimize missing and incorrect data such as value ranges and dropdown lists.
Descriptive analysis was done for all variables in the study. Categorical variables were presented with frequency and percentage. Continuous variables were presented with mean and standard deviation (SD) or median and interquartile range (IQR). The prevalence of exclusive breastfeeding for the first six months is defined as percentage of infants who were fed exclusively with breast milk when they were less than six months as reported by mothers.
Binary logistic regression analysis was used to estimate the crude odds ratio (OR) and 95% confidence interval (CI) between the outcome (exclusive breastfeeding) and independent variables. Multivariable logistic regression was used to explore factors associated with the outcome and reported using adjusted OR (aOR) and 95% CI. A P-value of < 0.05 was considered statistically significant. All analyses were done using R version 3.6.1.
Ethics approval and informed consentThe study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of The University of Medicine and Pharmacy at Ho Chi Minh City according to Decision No. 990 / HĐĐĐ-ĐHYD date 11 / 01 / 2020. The surveys were anonymous to protect the identities of both the mother and infant.
留言 (0)