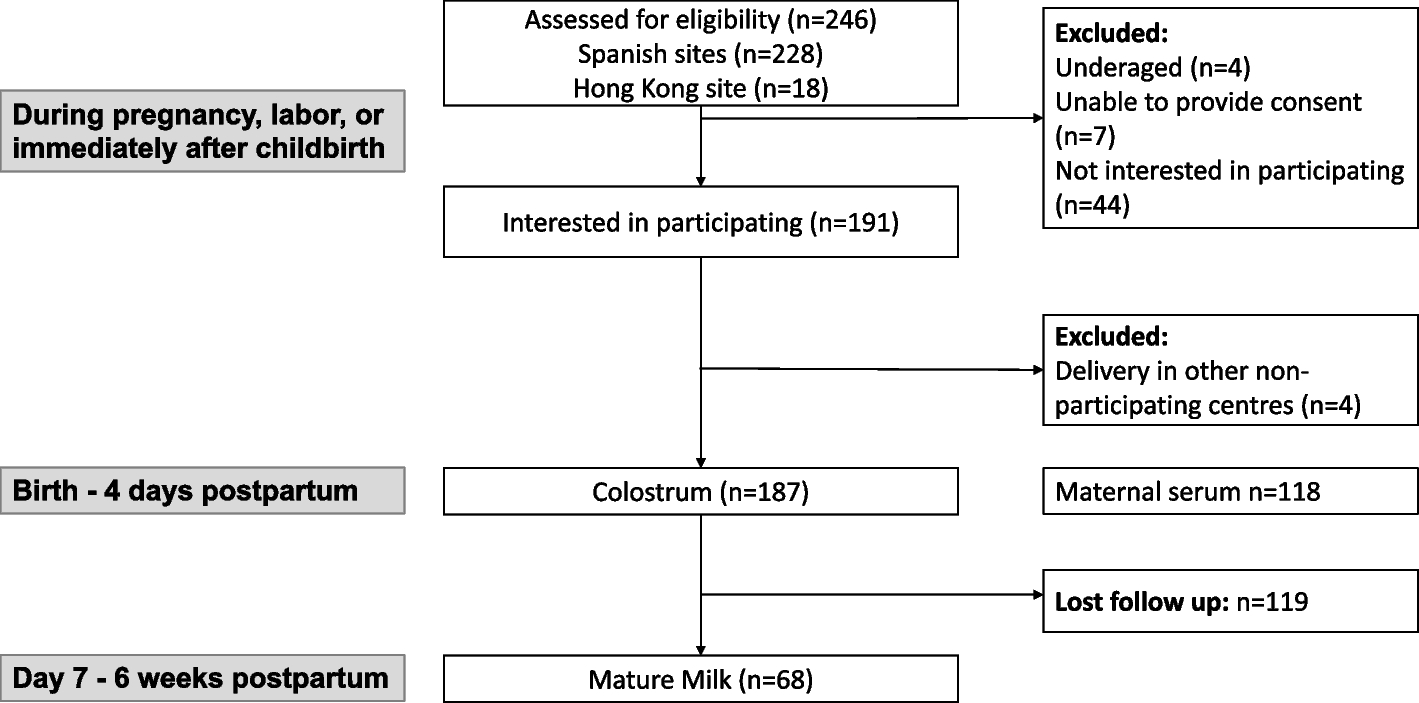
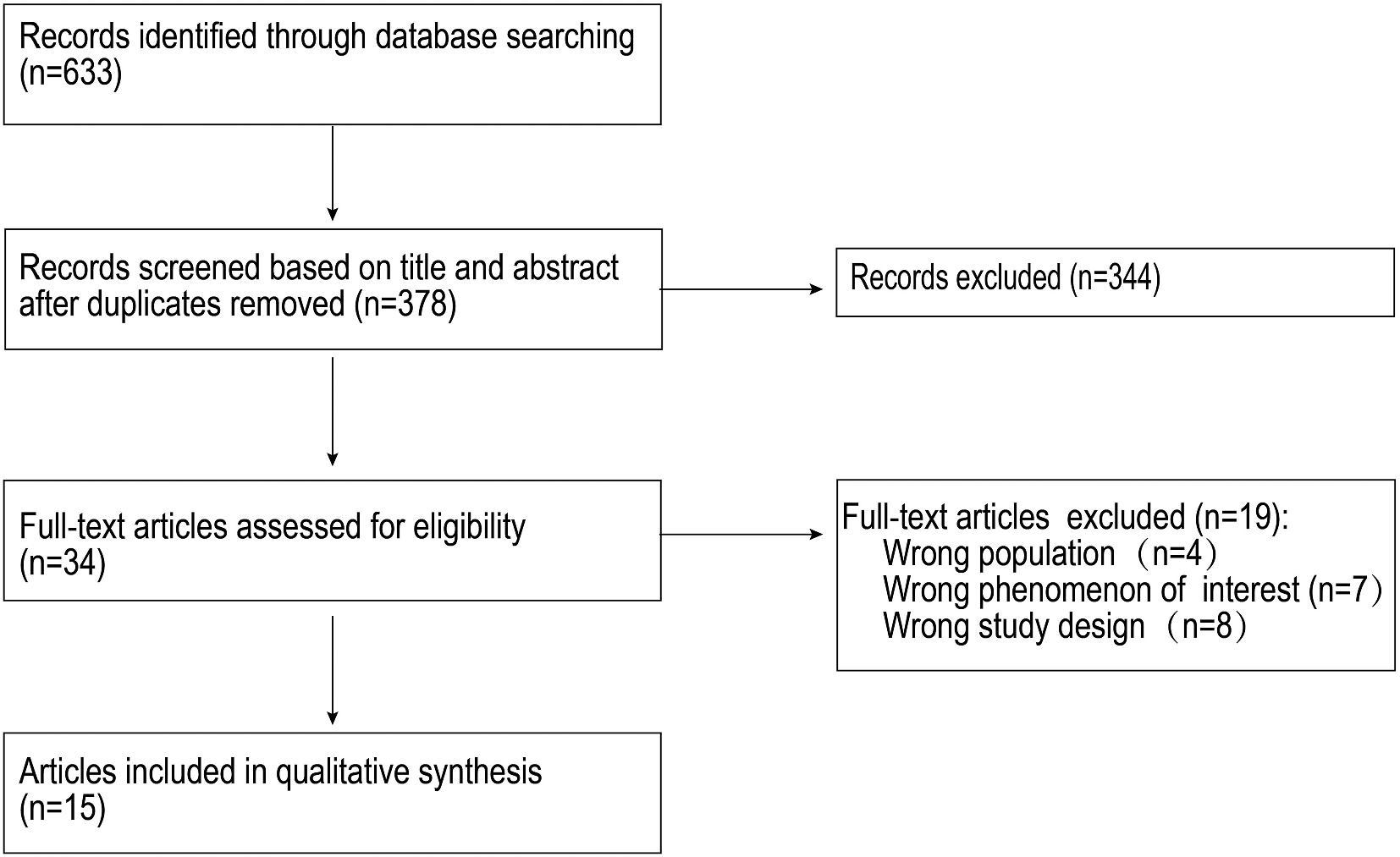
The study included 13 mothers of preterm infants (median age 32 years, range 26–44 years). Ten mothers had cesarean deliveries, while three had spontaneous delivery. Most (n = 7) mothers were interviewed two weeks after discharge, while others (n = 3) were interviewed between three to four weeks and one to two months after discharge. Feeding modes of mothers included mixed breastfeeding (n = 7) and exclusive breastfeeding (n = 6). Table 1 lists the demographic characteristics of the participants.
Table 1 Participant characteristics (n = 13)
Eleven subthemes were identified based on the data in the context during the analysis. Then, the findings were deductively mapped to higher-level domains of the BCW and lower-level domains of the TDF, resulting in five themes: (1) capability; (2) physical opportunity; (3) social opportunity; (4) reflective motivation; and (5) automatic motivation (Table 2).
Table 2 Overview demands to enhance breastfeeding behaviour and their corresponding COM-B component and TDF domain
Theme 1: capability
Capability refers to the relevant knowledge and skills to perform breastfeeding successfully.
TDF domain: memory, attention and decision processUnderstanding infants’ cues and identifying problems
Most mothers thought it was important to recognize when the baby is hungry or full in case of insufficient intake or unnecessary spitting up. Without the capability of reading infants’ cues, mothers were often uncertain while breastfeeding at home, which led to anxiety. Mothers stated that they desired a specific answer as to whether their breastfeeding was effective or not.
“He is so little and weak. A normal baby can eat himself enough. However, my baby requires more time because I feel the suction is weak. I cannot tell if he is full or tired when he stops eating. It causes me great concern.” (M3, multipara, 340/7weeks, 7 days of separation).
“The nurse instructed me to feed her as soon as she became hungry, but how can I swiftly determine if she is hungry? I was uncertain what she was saying to me when crying. It may be that her diaper is full, she does not feel safe, or a startle reflex comes up. I need assistance interpreting my infant’s cues.” (M2, unipara, 330/7weeks, 5 days of separation).
Moreover, they are eager to know whether their baby is continuing to be healthy after discharge. If the baby is becoming unwell, they desired to have the ability to recognize it as soon as possible.
“I would like a list that specifies the normal amount of human milk and urine, and the normal appearance of human stool. It does not need to be precise, but at least let me know when to become alert.” (M11, multipara, 340/7weeks, 14 days of separation).
“When he sucks, his face easily turns red with body twisted, and he will spit up a little. I often worry that he is uncomfortable and become sick again.” (M9, unipara, 306/7weeks, 43 days of separation).
In summary, most mothers wished to develop the ability to read infant cues and identify problems to breastfeed properly, confidently, and react promptly when problems arise.
TDF domain: knowledge; skillsBreastfeeding knowledge accumulation and skills training
All the mothers encountered challenges in breastfeeding. Interviews unveiled 16 categories of knowledge and skills that mothers aspired to learn in order to cope with difficulties (Table 3).
The majority of mothers consistently perceived insufficient breast milk production, which in turn influencing their beliefs about their own breastfeeding capabilities. Thus, lactation guidance and breast pump selection were frequently cited as participants’ primary request.
“I am nervous. My baby is so fragile, but I have insufficient breast milk (sigh). It would be great if there is any guidance to promote lactation.” (M3, multipara, 340/7weeks, 7 days of separation).
“I’m producing less and less breast milk these days. (…) While my baby was hospitalized, I had to rely on a breast pump. But the breast pump I randomly chose always caused discomfort and a tearing pain in my nipple when I used it. If only I had received some guidance on selecting a breast pump, I might have pumped more often.” (M6, unipara, 320/4weeks, 14 days of separation).
Most mothers emphasized that face-to-face guidance before discharge could give instant feedback on whether their breastfeeding technique was correct. Some also believed that a standardized set of courses by a trained nurse was better than ad hoc instruction.
“They can guide me (how to breastfeed) at discharge so that my wrong steps or postures can be corrected. If not, I have no idea whether I did it right or wrong when I returned home. It harms my baby and my breastfeeding confidence.” (M1, unipara, 350/7weeks, 5 days of separation).
“When I was hospitalized in the maternity ward, the nurse would not give formal and systematic training because she was too busy. She only gave guidance when she occasionally came in and felt that the new parents were clumsy. (…) Sometimes I wanted to ask for their instruction, but I was always unsure if it would interfere with their daily work. It would nice if there were a special nurse in charge of teaching.” (M11, multipara, 340/7weeks, 14 days of separation).
Mothers also agreed that a straightforward and fun course was more accessible to as they lacked medical background.
“I hope the class can be fun. Maybe you can teach us using models.” (M2, unipara, 330/7weeks, 5 days of separation).
Most participants stated that there was too much information to grasp fully and worried they would forget or make mistakes, leading to bad outcomes. Thus, many wanted a database containing relevant information about knowledge or skills that could be referred to as they liked. Several mothers believed written materials with images could be effective, while others preferred video.
“My husband was taught how to collect, store, and transfer human milk in the hospital, but he could not remember everything when he got home. Later, he took home written material and reviewed it periodically. It serves as a reminder and is convenient to annotate. (M8, unipara, 325/7weeks, 35 days of separation)
“My time is fragmented as mother. Nowadays, short-form videos are very popular, and I think this will suit me well.” (M4, unipara, 354/7weeks, 10 days of separation).
“Some skills or techniques are more intuitive through video demonstrations, while text or pictures sometimes cause misunderstandings.” (M7, unipara, 282/7weeks, 73 days of separation).
Overall, mothers were willing to learn relevant knowledge and skills, especially on lactation education and breast pump selection guidance. They hoped the course mode could be face-to-face, systematic, staffed and easy to understand. Additionally, they required an educational resource that integrated text, image, and video modes.
Theme 2: physical opportunity
Physical opportunity refers to environment that makes breastfeeding physically accessible and affordable in terms of resources, locations, time and triggers [25].
TDF domain: environmental context and resourceCleanliness and quietness in the household environment
Keeping the home clean and hygienic was a need identified by some mothers because preterm infants were more susceptible to infection. Some participants expressed concerns regarding the potential for increased risk of infections and elevated noise levels due to visits from relatives who came to give their congratulations.
“After the baby was discharged from the hospital, many elders came to visit and congratulate me at home, but each time I felt like I was facing the enemy. They hugged and kissed the baby. Even when I breastfed, female elders did not shy away. It was uncomfortable and stressful. (M2, unipara, 330/7weeks, 5 days of separation)
“I have stringent rules at home. If someone wishes to touch my baby, he must wash his hands first and is not allowed to enter the baby’s room. But some people cannot understand. They will think, ‘Is it necessary to make such a fuss about caring for a preterm baby?’” (M5, multipara, 336/7weeks, 46 days of separation).
In brief, mothers desired a clean and quiet home environment conductive to breastfeeding.
Breastfeeding support in workplaces
Women have multiple social roles and after their postpartum recovery they gradually returned to spaces outside of their home. Women wishing to continue breastfeeding hoped that society would strengthen their resolve by providing more breastfeeding resources to support their breastfeeding behavior.
“I have some friends who actively and passively weaned their babies when they returned to work. (…) As far as I know, my workplace does not provide a refrigerator for human milk storage, let alone a lactation room.” (M8, unipara, 325/7weeks, 35 days of separation).
“My superior does not value breastfeeding. After all, there are not many people who have this demand, so I think it is unrealistic to expect them to provide a lactation room especially for us. But at least there should be a private area where I can pump my milk freely.” (M1, unipara, 350/7weeks, 5 days of separation).
“Once I return to work, time can be pretty tight. I need to wake up at 6am every day to catch the subway for work. (…) It just feels like juggling work and breastfeeding will be tough.” (M3, multipara, 340/7weeks, 7 days of separation).
Overall, tools for breast milk storage, privacy spaces, and flexible schedule for lactation are what mothers need in workplaces.
Breastfeeding support in hospitals
After preterm infants were discharged from the hospital, they required regular follow-up, so the hospital environment and facilities were frequently mentioned as needing improvement.
“Initially, I thought the nursing room might be similar to that in the mall, but later I noticed it was at the end of the aisle with a small table and sofa, even without a door. The hospital was extremely crowded. Despite my embarrassment, I had to breastfeed my hungry baby.” (M9, unipara, 306/7weeks, 43 days of separation).
“I had cytomegalovirus in my breast milk. When I brought my baby for follow-up, I have to take a bottle of frozen human milk with me for pasteurization. However, no milk heater was available. I had to breastfeed him directly. (…) Hospitals should be equipped with enough breastfeeding facilities and aids. For example, we need nursing rooms, changing tables, sofas, milk heaters, water dispensers, sinks, sanitizers, trash cans and refrigerators.” (M11, multipara, 340/7weeks, 14 days of separation).
In short, they hoped there would be private spaces and tools for milk expression and storage in hospitals, which could make breastfeeding more convenient and dignified.
Theme 3: social opportunity
Social opportunity refers to environment that makes breastfeeding socially acceptable, including interpersonal influences and cultural norms.
TDF domain: social influencesPartner and family support
Participants shared a common problem: despite not fully recovering from the post-natal state, they had become the primary caregivers for their babies. Several mothers reported that they were not resting at home at all but working another way. The household chores and childcare tasks kept them busy and tired, distracting them from breastfeeding. Mothers agreed that breastfeeding was their own duty, but other baby care was the shared responsibility of the whole family.
“Caring for her is not as simple as it seems because it takes me a lot of time and energy. (…) I gave birth and breastfed her, but caring for her is not solely my duty. I need assistance from my husband and my mother-in-law. (M2, unipara, 330/7weeks, 5 days of separation)
“My husband offers me little help. Most of the time, he wants to help, but he does poorly. Luckily, my mother helps a lot. She can provide me with a nutritious diet and help with a diaper change, allowing me to focus on breastfeeding. However, sometimes views are diverse between old and new generations, and we will have disagreements in which neither of us can convince the other. (…) I hope all my family can be educated so there will be less disagreement and more integrated care.” (M11, multipara, 340/7weeks, 14 days of separation).
In summary, mothers considered shared responsibility and close collaboration important for infant care in their family. They needed family support to have more energy and time to breastfeed.
Peer support
Peer support, along with family support, was a critical component of social resources. A sense of disconnection with medical staff or a lack of breastfeeding experience increased peer communication requirements.
“ Communication between mothers is cordial. Perhaps similar people are more empathetic. (…) Medical staff may only communicate with you about the baby’s condition, but mothers can converse freely. Breastfeeding postures, recipes to promote lactation, and comfortable milk pumps are all meaningful topics.” (M2, unipara, 330/7weeks, 5 days of separation).
“I think the hospital can give chances for mothers to meet and interact so that we can learn and discuss with each other. (…) I am inexperienced, so if my baby behaves unusually, like a milk disc in the stool or refusing to eat, I will be worried about whether I should take him to the hospital or keep him under observation at home. However, if I know that other children have behaved like this before, and their mothers have feasible solutions, then my anxiety will dissipate.” (M7, unipara, 282/7weeks, 73 days of separation).
In contrast, several mothers exhibited less need for peer support. One mother said:
“I prefer quietness and I do not desire to talk to others. It is sufficient to have my family and doctors helping by my side.” (M5, multipara, 336/7weeks, 46 days of separation).
Overall, mothers who lacked breastfeeding experience, family support, and professional support were more inclined to seek peer support.
Authoritative support from healthcare providers
Some mothers believed that in addition to educating mothers, a particular ‘function’ of healthcare workers was advocating for mothers when their voices were barely heard within their family.
“Most people respect doctors naturally. When I complained of my depression and exhaustion, my family took me with a grain of salt, doubting if I was trying to be lazy. However, when doctors discussed postpartum depression and advocated for family corporation, they were more likely to believe and act.” (M2, unipara, 330/7weeks, 5 days of separation).
“What I said did not work. My mother tended to feed my baby water after each meal. I knew it was wrong but she insisted. The doctor was about to provide feeding instructions during a follow-up visit. Then I said, ‘hold on, please, I would like my mother to come in and learn together.’ (…) My mother never fed the baby extra water again after that. As a preterm mother, I hope the medical staff can instruct mothers and family members.” (M11, multipara, 340/7weeks, 14 days of separation).
In brief, healthcare workers were expected to provide authoritative support when mothers were not listened to.
Theme 4: reflective motivation
Reflective motivation refers to motivation that arises through reflection process, which involves plans (self-conscious intentions) and evaluations (beliefs about what is good and bad) [25].
TDF domain: beliefs about consequencesInformation about the health impacts of breastfeeding
Several primiparas recalled that their healthcare providers did not mention the need to pump breast milk early and regularly after delivery. They were initially unaware of the consequences of not doing it.
“I did not realize the importance of lactation on time until cuirushi (unlicensed layperson who helps a mother lactation by massaged her breasts) in the confinement center instructed me to lactate every 3 hours. Why did no one inform me of this while I was hospitalized? I am now worried about insufficient lactation.” (M8, unipara, 325/7weeks, 35 days of separation).
There was also a common perception among mothers that breastfeeding was better than formula feeding. Still, most of them did not know about the health impacts of breastfeeding, weakening their determination and motivation. Some mothers even doubted themselves, believed that formula was superior, and worried breastfeeding might lead to negative outcomes.
“Almost everyone tells me that human milk is more nutritious, but I know that formula-fed infants grow faster than breastfed babies. The confusion discourages me and makes me want to quit.” (M9, unipara, 306/7weeks, 43 days of separation).
Several mothers noted that babies should not be the only focus of breastfeeding, and that the benefits of breastfeeding for mothers should also be widely publicized.
“Not all mothers can stick to breastfeeding because it may cause nipple pain, poor sleep quality, and being out of shape. You should put yourself into mothers’ shoes and make them realize that the benefits of breastfeeding do not lay only in babies.” (M2, unipara, 330/7weeks, 5 days of separation).
In summary, information on the health impacts of breastfeeding was needed, and including why breastfeeding is better and how it impacts both mothers and infants, thereby strengthening their determination to continue breastfeeding.
Theme 5: automatic motivation
Automatic motivation refers to motivation aroused by emotional reactions like desires, impulses, inhibitions and reflex responses [25].
TDF domain: emotionMaternal-infant bonding
Most mothers described their contact with babies as happiness, peace and harmony, making them feel like “moms”.
“When I held him, even though he could not speak, his eyes gazed at me. It was like a secret spiritual communication, and I enjoyed the breastfeeding moment. (…) Sometimes they (babies) cried, and no one could successfully comfort them except me.” (M5, multipara, 336/7weeks, 46 days of separation).
“I remember the first time I breastfed, she lay on me, and it was a subtle, little cry-for-joy moment. I realized I had become a mother. Before that, I pumped my milk and sent it to NICU to find myself like a milk machine.” (M2, unipara, 330/7weeks, 5 days of separation).
All participants discussed that they couldn’t forget how much they missed their babies when hospitalized. Different views emerged regarding how they wished medical staff to help support bonding with their babies. Some participants wanted to view photos and videos of their babies, and a few mothers wanted to come to the NICU and stay together with their infants.
“I missed him extremely. I wanted him to return soon! (…) You can send us videos or photos or something similar.” (M1, unipara, 350/7weeks, 5 days of separation).
“The confinement center I lived hired pediatric professors from hospitals for weekly rounds. I wondered why the hospital did not have its own parent-child unit in the NICU, where the baby can receive treatment while staying with me, and it’s also more convenient for breastfeeding.” (M5, multipara, 336/7weeks, 46 days of separation).
In contrast, others believed that the scene of a baby living in an incubator with injections and probably tubes would increase their anxiety and heartbreak. Thus, they proposed a compromise:
“I will be satisfied if I can get the most fundamental information about him, such as milk volume, temperature, and weight. A one-minute phone call after rounds could put my mind at ease.” (M3, multipara, 340/7weeks, 7 days of separation).
“The baby’s daily treatment information or progress could be posted on the hospital’s website so that the doctors and nurses do not have to spend time on feedback and we can access it ourselves. additionally, the written records can be checked repeatedly in case of noise or misunderstanding on the phone.” (M10, unipara, 342/7weeks, 11 days of separation).
In short, most participants expressed that mother-infant contact and bonding could motivate breastfeeding. Mothers were in great need of information about their infants when they were apart. They felt that sending photos or videos was a straightforward way to provide information, while providing basic information via phone call or the internet was also important.
Free of aversive stimulus
A common sentiment among mothers was that they were not as valued as they were prior to the birth, with the baby receiving most of the family’s attention. It led to an awkward situation where some family members pressured mothers to eat and breastfeed for the baby’s benefit. This was uncomfortable and upsetting to some mothers.
“My mother-in-law gives me plenty of pressure. Initially, I planned to breastfeed, but after my babies returned home from NICU, I have to take care of two children. I felt tired and had inadequate breast milk. She ignored the fact and continued to emphasize the importance of breastfeeding. It made me nervous, upset, and resist breastfeeding for a while.” (M5, multipara, 336/7weeks, 46 days of separation).
“(…) I once cried in front of my husband. I could not control my emotions. I felt like my husband no longer respected and paid attention to me. He only cared about whether or not the baby was full. The only attention I got was, ‘why do you lactate less? Why do you eat less? The baby will be malnourished.’ This makes me feel like I am no mother but a cow.” (M2, unipara, 330/7weeks, 5 days of separation).
Overall, aversive stimuli could suppress mothers’ motivation to breastfeed. Mothers needed respect and comfort when faced with difficulties rather than questioning and pushing.

留言 (0)