
Remember me
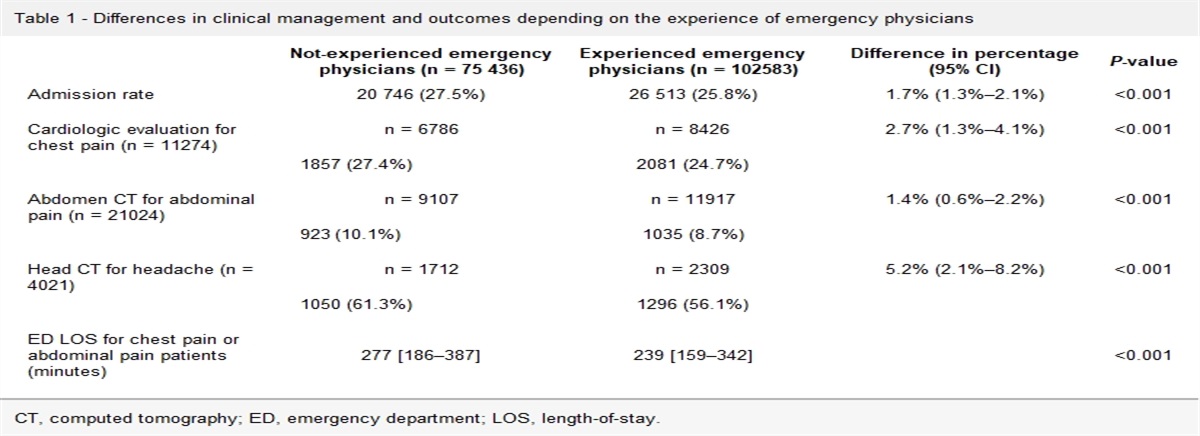
Acute heart failure (AHF) is the most common diagnosis in the emergency department (ED) leading to hospitalization [1]. A noninvasive, fast, accessible and efficient diagnosis of AHF is still challenging [2], especially in elderly individuals [3]. Some studies have reported up to 50% diagnostic [3] and treatment [1,2] errors, delays and unoptimized outcomes leading to high morbidity, mortality and costs [1]. NT-proBNP is the most commonly used diagnostic biomarker, with a class I recommendation [1,2], but has less accuracy, particularly in elderly individuals, women, obese patients and those with renal failure. Other biomarkers have been recently studied with sometimes controversial results [4]. Recent papers highlight methodological issues and the need for consistency in their use in heart failure [4]. High-sensitivity cardiac troponin-I (Hs-cTnI) is a marker of myocardial injury, and its mild elevation could support the diagnosis of AHF in the appropriate clinical setting [5]. Soluble ST2 (ST2), the soluble isoform of the ST2 gene, activates cardiomyocyte hypertrophy and cardiac fibrosis [6–8], and galectin-3, a soluble β-galactoside-binding protein, increases the proliferation of cardiac fibroblasts and stimulates collagen deposition and ventricular dysfunction; [8] ST2 and galectin-3 are recommended for risk stratification and prognosis in heart failure guidelines [1,2]. Both are increased and could be of diagnostic value in patients with AHF [6–8]. Soluble CD146 (CD146), a novel blood biomarker of cardiac congestion, seems to have better performance than NT-proBNP in AHF patients when the latter is in the ‘gray zone’ [9]. However, data concerning the diagnostic value of these biomarkers of AHF are limited, and no data exist regarding their combination. The main objective of this study was to assess the diagnostic accuracy of NT-proBNP, hs-cTnI, ST2, galectin-3, and CD146 alone and combined in diagnosing AHF in elderly patients presenting with acute dyspnea at the ED.
Methods Study design, ethics and participantsIn this prospective multicenter diagnostic study, patients were recruited from the ED of one of six French hospitals (3 university and 3 nonuniversity hospitals) between September 2016 and January 2020. The investigation complied with the Declaration of Helsinki and was approved by the following responsible French institutions: Commission Nationale de l’Informatique et des Libertés (CNIL-2207841), Comité de Protection des Personnes (CPP-Est-II-15/477), and Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM-151089B-21). The study was registered on ClinicalTrials.gov (NCT04240067). All patients provided written informed consent.
The inclusion criteria were age ≥75 years and at least two of the following acute dyspnea criteria: (1) respiratory rate ≥ 25 breaths per minute, (2) PaO2 ≤ 70 mmHg, (3) SpO2 ≤ 92% in ambient air, and (4) PaCO2 ≥ 45 mmHg and pH ≤ 7.35 or (5) oxygen therapy. The criteria for noninclusion were shock, respiratory distress (respiratory rate > 30 breaths per minute, use of accessory respiratory muscles, or SpO2 < 90% despite O2 therapy), acute coronary syndrome (based on EKG findings), other obvious cause for dyspnea (pneumothorax or clinical-radiological systematized pneumopathy), and cardiac or pulmonary therapies initiated prior to inclusion (i.e. diuretics). Patients received standard ED management, two additional heparinized plasma cryotubes were collected at admission, and transthoracic echocardiography was performed by a cardiologist within 24 h of ED admission (according to the ESC and AHA recommendations for AHF [1,2]) specifically for this research.
Biomarker analysisAccording to the Clinical and Laboratory Standards Institute (formerly NCCLS) guideline EP5-A [10], the collected tubes were delivered within 30 min to the laboratory and frozen at -80 °C (Table S1, Supplemental digital content 2, https://links.lww.com/EJEM/A398).
Data collectionData were anonymized and collected using an online case report form (e-CRF) by a local clinical research associate (Table S2, Supplemental digital content 2, https://links.lww.com/EJEM/A398).
Reference standardThe definitive diagnosis of AHF was adjudicated by two independent emergency medicine physicians based on e-CRF data (Table S2, Supplemental digital content 2, https://links.lww.com/EJEM/A398), in accordance with guidelines from the ESC and AHA [1,2]. The physicians were blinded to the biomarker data during the evaluation. If there was any disagreement between the two experts, a third expert was consulted.
Statistical methods Index testThe diagnostic performances of the 5 biomarkers were individually determined before the multimarker approach was performed.
Expression of variables and comparisons between groupsCategorical variables are expressed as numbers, proportions and percentages with their estimators. The continuous variables are expressed as the means and standard deviations for variables with Gaussian distributions and medians and interquartile for variables with non-Gaussian distributions.
Monomarker analysisThe assessment of each biomarker and comparison were performed using a receiver operating characteristic (ROC) curve and area under the curve (AUC). The diagnostic performance of each biomarker was calculated to obtain the optimal threshold maximizing Youden’s index. The comparisons between the AHF group and the non-AHF group were performed using Student’s t-test for continuous variables or the chi-square test for categorical variables.
Correlations between biomarkers 2 by 2The correlations between the different biomarkers were assessed using Spearman correlation coefficients.
Cross-sectional approachesA cross-sectional approach (using simultaneously the results of all biomarkers) was first conducted in two ways: using logistic regression, where a backward descending stepwise selection of variables up to the P < 0.05 threshold was performed (Table S3, Supplemental digital content 2, https://links.lww.com/EJEM/A398) and then using ‘Bell’s combinations’ [11], namely, counting all positive combinations between the 5 biomarkers as follows: biomarker 1 AND biomarker 2, biomarker 1 OR biomarker 2, biomarker 1 AND biomarker 2 OR biomarker 3, etc. All Bell combinations (for 5 biomarkers B5 = 52) [11] were defined and explored (Table S4, Supplemental digital content 2, https://links.lww.com/EJEM/A398).
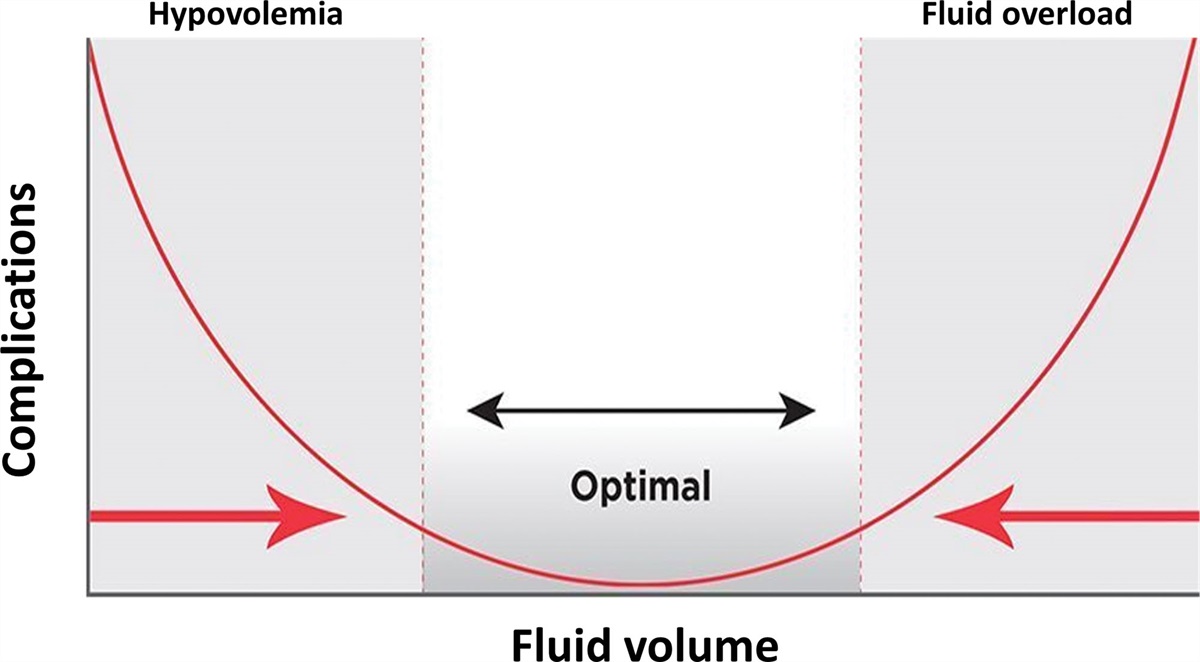
Sequential approachA sequential approach was adopted to assess the diagnostic value of the addition of a biomarker according to the results of a previous biomarker in patients who could not be classified by the latter. Each biomarker had a lower and an upper threshold and a gray zone instead of a positive/negative cutoff [12,13]. Patients with a biomarker value lower than the lower threshold were considered to have a negative test; when the value of the biomarker was higher than the upper threshold, the test was considered positive. Values between the upper and lower thresholds were considered in the gray zone. This method called ‘gray zone optimizations’ included successive combinations considering the inconclusive gray zones defined above. The determination of the thresholds included a lower threshold (rule-out) with a sensitivity ≥80% and an upper threshold (rule-in) with a specificity ≥80%, thereby maximizing sensitivity and specificity, respectively (Fig. 1) [12]. Every step-by-step sequential biomarker combination was determined. The first biomarker was the one with the best accuracy in the monomarker analysis. For each biomarker, several upper ‘rule-in’ (patients with AHF) thresholds (maximizing specificity, between 80 and 100%) and several lower ‘rule-out’ (patients without AHF) thresholds (maximizing sensitivity, between 80 and 100%) were tested. Patients ruled-in or ruled-out were considered classified. Between these thresholds was an ‘interval’ representing the inconclusive gray zone of nonclassified patients. The latter was assessed with the other biomarkers. A ROC analysis was conducted, and the AUC of all remaining biomarkers was determined. When the AUC was ≥0.6 and the confidence intervals (CIs) did not contain 0.5, the same steps were repeated, creating several ‘paths’ from a gray zone to the next one. When the AUCs of the remaining biomarkers were all <0.6 or their CIs contained 0.5, the previous step was considered the last. The last step of each path was always conducted with a unique threshold, allowing a binary response (positive or negative) [12,13]. The following diagnostic performance indices were assessed: diagnostic accuracy, sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, negative likelihood ratio, and their associated 95% CI. Then, an assessment of the diagnostic performance of each complete path was performed.
 Fig. 1:
Fig. 1: Description of the ‘gray zone optimization’ approach in READ-MA. AUC, area under the curve; BM, biomarker; TEST+, positive test; TEST−, negative test.
Statistical data managementThe main characteristic that was analyzed to assess diagnostic performance in diagnosing AHF was accuracy. ‘Standard for Reporting Diagnostic accuracy studies’ guidelines were used [14]. The clinical information and reference standard results were not available to the primary investigator conducting the index test. The statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA) and MedCalc 4.16 g (Frank Schoonjans, Ostende, Belgium). A 2-sided P-value <0.05 was considered statistically significant. Patients who did not meet the sample criteria or had missing biomarker data were excluded.
Sample sizeThe sample size was determined according to an expected incidence of AHF of 0.45, an expected accuracy of 0.81 and an absolute uncertainty of 0.05% for a 95% CI [15]. The calculated sample size was 237. Applying a rate of 10% for missing data, a sample size of 260 patients was retained.
Results ParticipantsIn total, 271 patients were included (Fig. 2), and 238 were analyzed. Among them, 110 (46%) of these patients were diagnosed with AHF by the adjudication committee. The baseline characteristics of the participants are presented in Table 1 and Table S5, Supplemental digital content 2, https://links.lww.com/EJEM/A398. The median NT-proBNP, Hs-cTnI, ST2, galectin-3, and CD146 concentrations were higher in the patients with AHF than in those with no AHF. The distribution of the reference standard compared to alternative diagnoses is presented in Table S6, Supplemental digital content 2, https://links.lww.com/EJEM/A398. Among the 128 patients with no AHF diagnosis, the main diagnoses were pneumonia (n = 87 [68%]), exacerbation of chronic obstructive pulmonary disease (n = 50 [39%]), acute pulmonary embolism (n = 11 [8.5%]), asthma (n = 4 [3%]), other causes (n = 29 [22%]) and sepsis (n = 24 [18%]).
Table 1 - Baseline characteristics of the READ-MA patients Variablea Acute heart failure N = 110 No acute heart failure N = 128 All patients N = 238 P valueb Age in years 86.9 (9.3) 84.2 (8.5) 85 (8.8) 0.01 Female 45 (40.9) 62 (48) 107 (44.9) 0.24 Body mass index (kg/m2) 25.8 (5.3) 25.3 (6.4) 25.5 (6.4) 0.91 History of COPD 23 (20.9) 32 (25.0) 55 (23.1) 0.45 Heart failure 68 (61.8) 33 (25.7) 101 (42.8) <0.001 Coronary artery disease 33 (30.0) 22 (17.1) 55 (23.1) <0.02 Chronic kidney disease 20 (18.1) 14 (10.9) 34 (14.3) 0.11 High blood pressure 84 (76.3) 87 (67.9) 171 (71.8) 0.15 Diabetes 35 (31.8) 31 (24.2) 66 (27.7) 0.19 Atrial fibrillation 17 (15.4) 28 (21.8) 45 (18.9) <0.05 Clinical findings at presentation Heart rate (bpm) 84 (25) 91 (28) 88 (27) <0.01 Respiratory rate (bpm) 28 (5) 27 (68) 27 (6) 0.41 Temperature (°C) 36.8 (0.8) 37.4 (1.3) 37 (1.3) <0.001 SBP (mmHg) 138 (30) 133 (32.5) 136 (31) 0.62 DBP (mmHg) 74 (20) 73.5 (24.2) 74 (22) 0.12 Saturation before oxygen therapy (%) 95 (4.5) 94 (5) 90 (5) 0.11 Rales 82 (74.5) 64 (50.0) 146 (61.3) <0.001 Sibilant rales 39 (35.4) 29 (22.6) 68 (28.5) 0.03 Lower-extremity edema 62 (56.3) 40 (31.1) 102 (42.8) <0.001 Laboratory data at presentation Serum urea nitrogen (mg/L) 10 (7.3) 8.3 (6) 8.8 (6.9) 0.43 Serum creatinine (µmol/L) 93.6 (54.2) 85.4 (50.3) 90.1 (53.5) 0.42 Serum sodium (mmol/L) 140 (5) 138 (4) 139 (4) 0.19 Serum potassium (mmol/L) 4.2 (0.7) 4.3 (0.7) 4.3 (0.7) 0.34 Procalcitonin (ng/mL) 0.28 (0.37) 0.28 (0.95) 0.26 (0.76) 0.71 D-dimers (ng/mL) 1588 (1432) 1050 (1315) 1215 (1700) 0.67 READ-MA biomarkers at presentation NT-proBNP (ng/L) 5321 (10 007) 1422 (2369) 2396 (5383) <0.001 HS-cTnI (ng/L) 37.5 (63.0) 26.4 (44.0) 31.6 (54.1) 0.08 Soluble ST2 (ng/mL) 75.2 (87.9) 79.3 (81.2) 78.1 (82.5) 0.59 Galectin-3 (ng/mL) 23.4 (12.2) 20.9 (11.0) 22.2 (12.2) 0.25 Soluble CD146 (ng/mL) 428 (185.2) 367.0 (142.0) 386.5 (167.7) <0.001 Echocardiography data obtained within 24 hc Left ventricular ejection fraction (%) 53 (19) 61 (7) 60 (15) <0.001 HFrEFd, n (%) 23 (20.9) 4 (3.1) 27 (11.3) <0.001DBP, diastolic blood pressure; HS-cTnI, high-sensitivity cardiac troponin-I; SBP, systolic blood pressure.
aThe data are presented as the median (interquartile range) or n (%) unless otherwise indicated.
bBetween the acute heart failure and no acute heart failure groups, a Chi-square, a Student’s t-test, or a one-way ANOVA (nonparametric Kruskal-Wallis) were performed.
dHeart failure with a reduced ejection fraction.
 Fig. 2:
Fig. 2: Flowchart of the selection of READ-MA patients. AHF, acute heart failure; Hs-cTnI, high-sensitivity cardiac troponin-I.
Biomarker characteristicsThe ROC curves and diagnostic performance indices are presented in Fig. 3. The AUCs ranged from 0.52 (95% CI 0.45–0.59) for ST2 to 0.79 (95% CI 0.73–0.84) for NT-proBNP, and the accuracy ranged from 0.51 (95% CI 0.45–0.57) for ST2 to 0.72 (95% CI 0.66–0.77) for NT-proBNP (Fig. 3). The correlation coefficients are presented in Table S7, Supplemental digital content 2, https://links.lww.com/EJEM/A398.
 Fig. 3:
Fig. 3: Monomarker analysis: ROC curves (a) and diagnostic performances (b) of the 5 biomarkers in the READ-MA study (N = 238). AUC, area under the curve; CI, confidence interval; Hs-cTnI, high-sensitivity cardiac troponin-I; LR−, negative likelihood ratio; LR+, positive likelihood ratio; NPV, negative predictive value; PPV, positive predictive value; Se, sensitivity; Sp, specificity; ST2, galectin-3 and CD146: ng/ml; Thresholds, NT-proBNP and high-sensitivity cardiac troponin-I: ng/L.
Multimarker analysisThe multimarker approaches are presented and compared with each other and with NT-proBNP in Table 2. Regarding logistic regression, none of the seven statistically significant combinations had a significantly higher accuracy than NT-proBNP alone (Table S8, Supplemental digital content 2, https://links.lww.com/EJEM/A398). The highest accuracy according to the logistic regression (0.73, 95% CI 0.67–0.78) was comparable to that of NT-proBNP. The highest accuracy with Bell’s combinations among the 52 combinations of the 5 biomarkers (treated as categorical variables, Table S9, Supplemental digital content 2, https://links.lww.com/EJEM/A398) was identical to that of NT-proBNP (0.72, 95% CI 0.66–0.77). Regarding the gray zone optimizations, none of the 110 combinations optimizing the gray zone step-by-step of each biomarker had a significantly higher accuracy than NT-proBNP alone (Table S10, Supplemental digital content 2, https://links.lww.com/EJEM/A398). The highest accuracy (0.71, 95% CI 0.65–0.76) was comparable to that of NT-proBNP (Table 2).
Table 2 - Comparison of the 3 best combinations from the multimarker approaches (N = 238) Approach AUC (95% CI) Sensitivity (95% CI) Specificity (95% CI) PPV NPV LR+ LR− Accuracy (95% CI) NT-proBNP continuous 0.79 (0.73–0.84) 0.85 (0.80–0.89) 0.62 50.55–0.68) 0.65 0.83 2.21 0.25 0.72 (0.66–0.77) NT-proBNP categoricala 0.72 (0.67–0.77) 0.85 (0.80–0.89) 0.61 (0.54–0.67) 0.65 0.82 2.16 0.25 0.72 (0.66–0.77) Logistic regressionb 0.79 (0.73–0.84) 0.84 (0.79–0.88) 0.64 (0.58–0.70) 0.67 0.82 2.33 0.25 0.73 (0.67–0.78) Bell’s combinationsc 0.79 (0.72–0.84) 0.79 (0.74–0.84) 0.66 (0.60–0.72) 0.67 0.78 2.35 0.31 0.72 (0.66–0.77) Gray zone optimizationd 0.71 (0.66–0.76) 0.82 (0.77–0.87) 0.61 (0.55–0.67) 0.64 0.80 2.09 0.30 0.71 (0.65–0.76)NT-proBNP continuous: continuous variable; NT-proBNP categorical: categorical variable.
AUC, area under the curve; CI, confidence interval; LR−, negative likelihood ratio; LR+, positive likelihood ratio; NPV, negative predictive value; PPV, positive predictive value; Se, sensitivity; Sp, specificity.
aThreshold of 1805 ng/L.
bCombination 1.1.
cCombination 2.21.
In this prospective cohort study that included 238 patients, several biomarkers (NT-proBNP, hs-cTnI, ST2, galectin-3 and CD146) were tested alone or in combination to assess their diagnostic performances for AHF. Regardless of the approach used and how the 5 biomarkers were combined, the diagnostic accuracy of AHF in elderly patients presenting with acute dyspnea at the ED did not differ from that of NT-proBNP alone. The prevalence of patients with AHF was comparable to that in the literature in the same population and setting [3,16], although mostly with heart failure with preserved ejection fraction (HFpEF). Diseases other than AHF were also comparable to those in the literature [3]. The proportion of the final diagnosis was comparable to that in other studies [3]. The present study was performed in various centers, university and nonuniversity hospitals, limiting extrapolation bias. Therefore, the source population is representative of the target population (elderly patients presenting with acute dyspnea to the EDs). The reference standard assessment was based on international guidelines. None of the 5 biomarkers were a part of the reference standard, avoiding incorporation bias. The two double-blind experts’ reference standard assessments were concordant, limiting unsatisfactory tests (none required a third assessment). The blood test collection, storage, transport and assay procedures were standardized and followed the guidelines. Several complementary multimarker approaches were performed to assess a comprehensive combination set of the 5 biomarkers. No work-up bias was identified, and the reference standard was performed for every patient regardless of the biological results. (Central Illustration, Supplemental digital content 3, https://links.lww.com/EJEM/A399).
Monomarker analysisAlthough less efficient in elderly individuals, NT-proBNP levels have a reasonably high diagnostic accuracy for AHF and improve the diagnostic accuracy of clinical judgment in the ED [3,16–25]. The rule-in threshold is based on the patient’s age and is higher in elderly individuals, and the gray zone is wider in elderly individuals [20,25]. In our study, the AUC and accuracy of NT-proBNP were good. The monomarker analysis using a 1805 ng/L threshold showed diagnostic performance comparable to that in the literature at the 1800 ng/L threshold.7 In our population, age, renal function and especially HFpEF could explain the lower specificity and positive predictive value compared to those in larger trials and are comparable to the literature involving elderly individuals [15–18,20,24,26]. Therefore, NT-proBNP alone is a valuable biomarker for the diagnosis of AHF in elderly patients presenting with acute dyspnea to the EDs. Hs-cTnI showed moderate diagnostic performance, with low sensitivity and negative predictive value. Several studies have demonstrated an increase in the Hs-cTnI concentration in AHF of up to 57%, particularly in severe AHF, and an increased ventricular preload causing myocardial strain has been speculated [5,22]. In our study, the hs-cTnI levels and left ventricular wall strain were not higher in the AHF patients. Our best threshold was comparable to that in the literature in similar settings [22]. It could be useful to rule out AHF if negative, but its diagnostic value is limited. ST2 is not significantly influenced by age [27] or comorbidities, such as renal dysfunction, which remain major biases in the interpretation of NT-proBNP [14]. AbouEzzeddine et al. [28] studied a cohort of HFpEF patients and showed that ST2 levels were associated with proinflammatory comorbidities, right ventricular pressure overload and dysfunction, and systemic congestion but not with left ventricular geometry or function. ST2 may be a marker of systemic inflammation in HFpEF and potentially of extracardiac origin. In our study, the AUC and accuracy of ST2 were low. Regarding the 32 ng/ml threshold, high sensitivity and NPV were associated with very low specificity and low accuracy and positive predictive value, which is consistent with the findings reported in similar studies [7,8]. ST2 levels were low in this study, and its diagnostic performance was also low. The very low specificity of ST2 could be explained by its increased plasma concentrations in patients with alternative diagnoses such as pneumonia, COPD, or sepsis [23], who were frequent co or alternative diagnoses in our population. Thus, ST2 alone is not a valuable biomarker for the diagnosis of AHF in elderly patients. Galectin-3 showed moderate diagnostic performance and was comparable to that reported in the literature [8,29]. Van Kimmenade et al. [29] assessed galectin-3 plasma levels in 599 patients presenting with dyspnea at the ED, of whom 209 (35%) had AHF. The specificity was comparable (0.52), but the sensitivity was higher (0.80) in this younger population. Several studies have also assessed the diagnostic value of galectin-3 for AHF in an ED setting [4,8,29]. However, its diagnostic value and disease specificity are limited, and it is not a valuable biomarker for the diagnosis of AHF in elderly patients. CD146 correlates with the radiological severity of pulmonary congestion in the early phase of acute coronary syndrome [9] and, in contrast to BNP, is not affected by the amount of myocardial cell necrosis. It showed moderate diagnostic performance, which contradicts the results reported by Gayat et al. [9], who showed that CD146 has a high diagnostic value and performance. Despite elevated CD146 levels in patients with HFpEF, the diagnostic value of CD146 alone for the diagnosis of AHF in elderly patients seems limited. The correlation between the five biomarkers suggested that no diagnostic threshold effect existed and that the biomarkers were not highly associated; therefore, an improvement by a combination was theoretically possible.
Multimarker analysisNeither the cross-sectional n
Comments (0)