Study characteristics
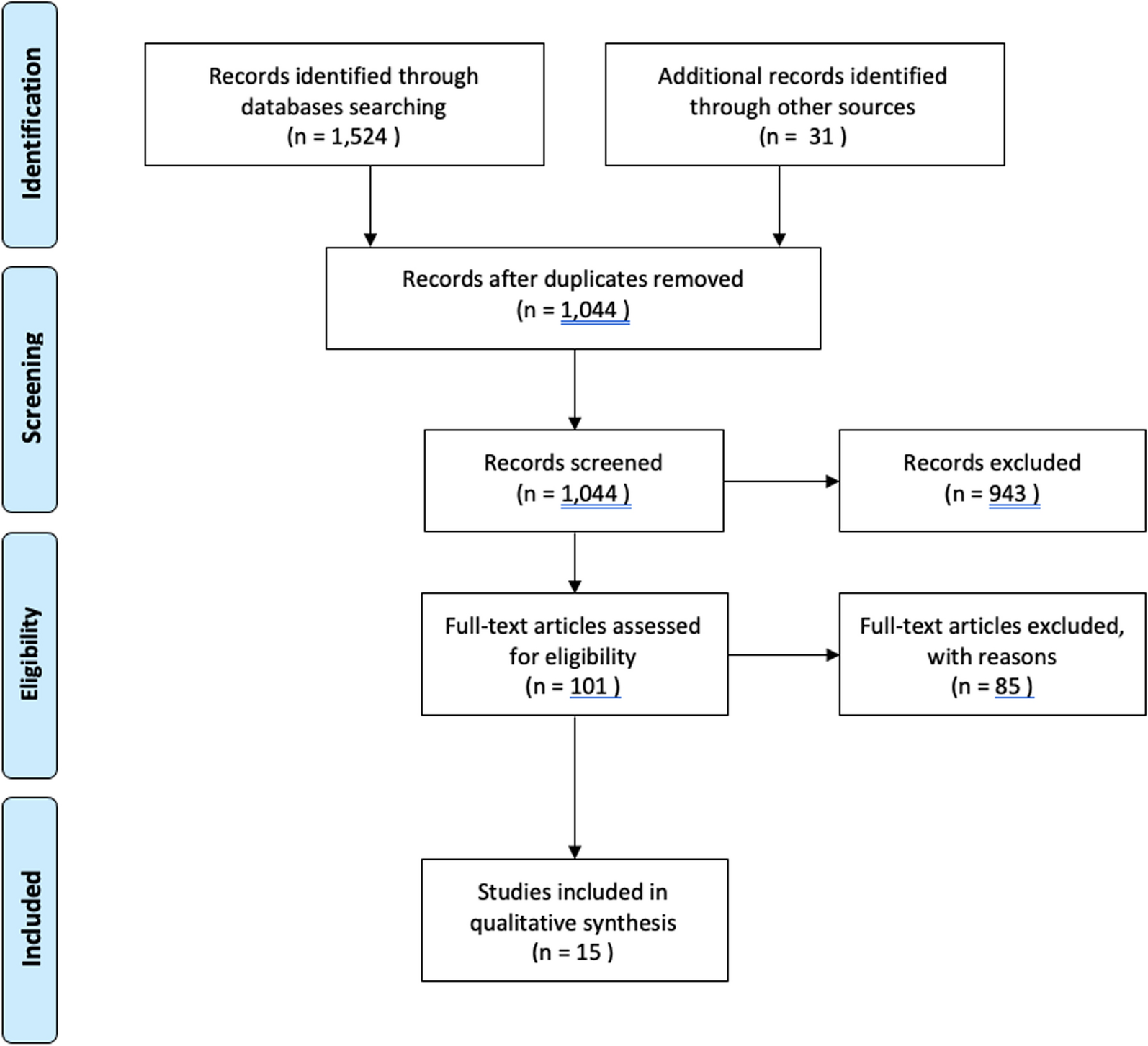
A total of 22 studies involving 800 patients with trauma fractures (median follow-up 12 months) and 5 studies involving 102 patients (median follow-up 12 months) with (impending) pathological fractures were included in the systematic review. Among them, 11 studies (497 patients, median follow-up 12 months), including three RCTs, compared CF plates with metal plates for trauma fractures (Table 1).
Table 1 Demographics of all included studies (n = 27) for trauma fractures (n = 22), of which 11 were comparative, and (impending) pathological fractures (n = 5)Study quality
The overall quality assessment score for RCTs, according to RoB 2 tool was “some concerns” for all included RCTs (n = 3; Table 2). The ROBINS-I criteria score for non-comparative studies ranged from low to moderate (n = 19; Table 3), and the mean score for case reports was 6 out of 8 (n = 5; Table 4). Following the GRADE approach, randomized trials were initially rated with a high certainty of evidence. However, due to the risk of bias of the included RCTs, scores were lowered in their certainty of evidence to moderate (Table 5). Observational studies and case reports were rated as with a low or very low certainty of evidence (Table 5). Consequently, recommendations of using CF plates for fixating fractures should be done with caution.
Table 2 Risk of Bias II (RoB 2) tool for RCTsTable 3 Risk of Bias in Nonrandomized Studies of Intervention (ROBINS-I) tool for non-RCTsTable 4 Joanna Briggs Institute Critical Appraisal Checklist for Case Reports (n = 5)Table 5 Reported complicationsReported complications after CF plate fixation for trauma fractures
In the upper extremity, seven studies evaluated CF plate fixation after traumatic proximal humerus fractures, involving a total of 391 patients [16, 26,27,28,29,30,31]. The most frequently reported complications were soft tissue complications (n = 52; 13%), including impingement between plate and acromion (n = 18), rotator cuff lesions (n = 18), adhesive capsulitis/shoulder stiffness (n = 15) and an intra-articular bicep tendon rupture (n = 1). Avascular humeral head necrosis/collapse was also frequently reported (n = 27; 7%). In addition, structural complications were frequently observed (n = 23; 6%), which consisted of secondary screw perforation (n = 12), screws backing out (n = 5), plate breakages (n = 4) and malpositioning of the plate (n = 2). Furthermore, secondary loss of reduction or resorption (> 50%) of tuberosity (n = 17; 4%), varus/valgus malalignment (n = 6; 2%), head shaft malreduction (n = 12; 3%), malreduction of the fracture (n = 3; 1%), nonunions (n = 2; 1%), secondary glenohumeral osteoarthritis (n = 2; 1%) and an infection (n = 1; < 1%) were documented as unfavourable events. Eight studies reported on traumatic distal radius fractures, with a total of 291 patients [10, 32,33,34,35,36,37,38]. Complications for this group included structural complications (n = 6; 2%), soft tissue complications (n = 5; 2%) and an infection (n = 1; < 1%).
Regarding the lower extremity, four studies assessed traumatic femur fracture fixations with CF plates, encompassing a total of 34 patients [39,40,41,42]. Complications observed in this group included one nonunion (n = 1; 3%) and one structural complication (plate breakage, n = 1; 3%). Furthermore, three studies evaluated ankle fractures treated with CF plates [43,44,45], involving 104 patients in total. The most frequently reported complications included infections (n = 4; 4%), soft tissue complication (n = 2; 2%) and one nonunion (n = 1; 1%; Table 5).
Reported complications after CF plate fixation for (impending) pathological fractures
In the upper extremity, two studies evaluated pathological fractures involving 14 humerus and 2 distal radius CF plates [46, 47]. Most frequently reported humerus complications included infections (n = 2; 14%), a structural complication (traumatic plate breakage, n = 1; 7%) and a tumour progression (n = 1; 7%) for which the plate was removed. No complications were reported for the 2 distal radius CF plates.
Regarding the lower extremity, five studies encompassing a total of 86 patients investigated femoral and/or tibial (impending) pathological fractures [46,47,48,49,50]. Complications included structural failures (n = 6; 7%), consisting of plate breakages without clear trauma (n = 2), periprosthetic fractures (n = 2), screw breakage (n = 1) and screw backing out (n = 1). Additionally, documented complications consisted of tumour progressions (n = 5; 6%), infections (n = 4; 5%), nonunion (n = 3; 4%), aseptic loosening (n = 2; 3%), paediatric complications (valgus deformations treated with eight-plates, n = 2; 3%) and a soft tissue complication (wound dehiscence after radiotherapy treatment, n = 1; 2%; Table 5).
Studies comparing CF plates with metal plates
Eleven studies have compared CF plates with metal plates, all focusing on traumatic fractures [26,27,28,29,30, 33, 36, 37, 40, 42, 44]. Among these studies, three were RCTs, and the remaining eight were prospective (n = 4) or retrospective (n = 4) comparative studies. This study hypothesized that CF plates display similar complication rates and clinical outcomes as metal plates for fracture fixation.
In the upper extremity, five studies examined CF plates compared with metal plates for humerus fractures. Firstly, Dey Hazra et al. conducted a retrospective study comparing range of motion after 2 years after fixation using CF plates (n = 30) or titanium plates (n = 35) [30]. The CF group demonstrated significantly improved forward flexion, internal rotation and abduction compared with the titanium group, with similar patient reported outcomes. Secondly, Katthagen et al. prospectively enrolled 21 CF-treated patients and matched them with 21 titanium treated patients [26]. Although functional outcomes were comparable after 12 months, the titanium group required more revisions due to screw perforations (5 versus 0; p = 0.048). Thirdly, Schliemann et al. conducted a prospective study comparing clinical and radiographic results of CF-treated patients (n = 29) to those treated with metal locking plates (n = 29) [28]. After 2 years, patients treated with CF plates achieved significantly better Constant Murley and Oxford Shoulder scores (p = 0.038 and 0.029, respectively), with fewer cases with loss of reduction or varus deformity in the CF group. Fourthly, Padolino et al. conducted a retrospective study comparing clinical and radiographic outcomes of CF-treated patients (n = 21) to those treated with titanium plates (n = 21) [27]. Shoulder mobility, clinical and pain scores were similar in both patient groups after 2 years, while cortical thinning was significantly greater in the CF group (p = 0.0003). Besides, the metal group exhibited a significantly higher rate of tuberosity resorption (p = 0.040). Lastly, Ziegler et al. performed an RCT comparing CF plates (n = 32) with titanium plates (n = 31), but reported no clinical or radiological differences after 6 month’s follow-up [29]. For distal radius fractures, three comparative studies consistently demonstrated similar clinical and radiological outcomes during follow-up evaluations spanning 2 weeks to 3 years [33, 36, 37].
In the lower extremity, two studies evaluated CF and metal plates for distal femur fractures. Mitchell et al. compared CF plates (n = 11) with stainless steel plates (n = 11), observing a trend towards better outcomes in the CF plate group, including less nonunion, less structural failures and less reoperations (9% versus 36%; 0% versus 18%; and 9% versus 36%, respectively) [42]. Byun et al. also compared CF (n = 10) with stainless steel (n = 21), noting better callus formation at 3 months, although this effect diminished at 6 months [40]. Regarding ankle fractures, Guzzini et al. compared CF plates (n = 47) with stainless steel plates (n = 41), reporting no significant differences in terms of pain, radiographic and clinical outcomes at 6-, 12- and 24-month follow-up evaluations [44] (Table 5).








Comments (0)