Study population
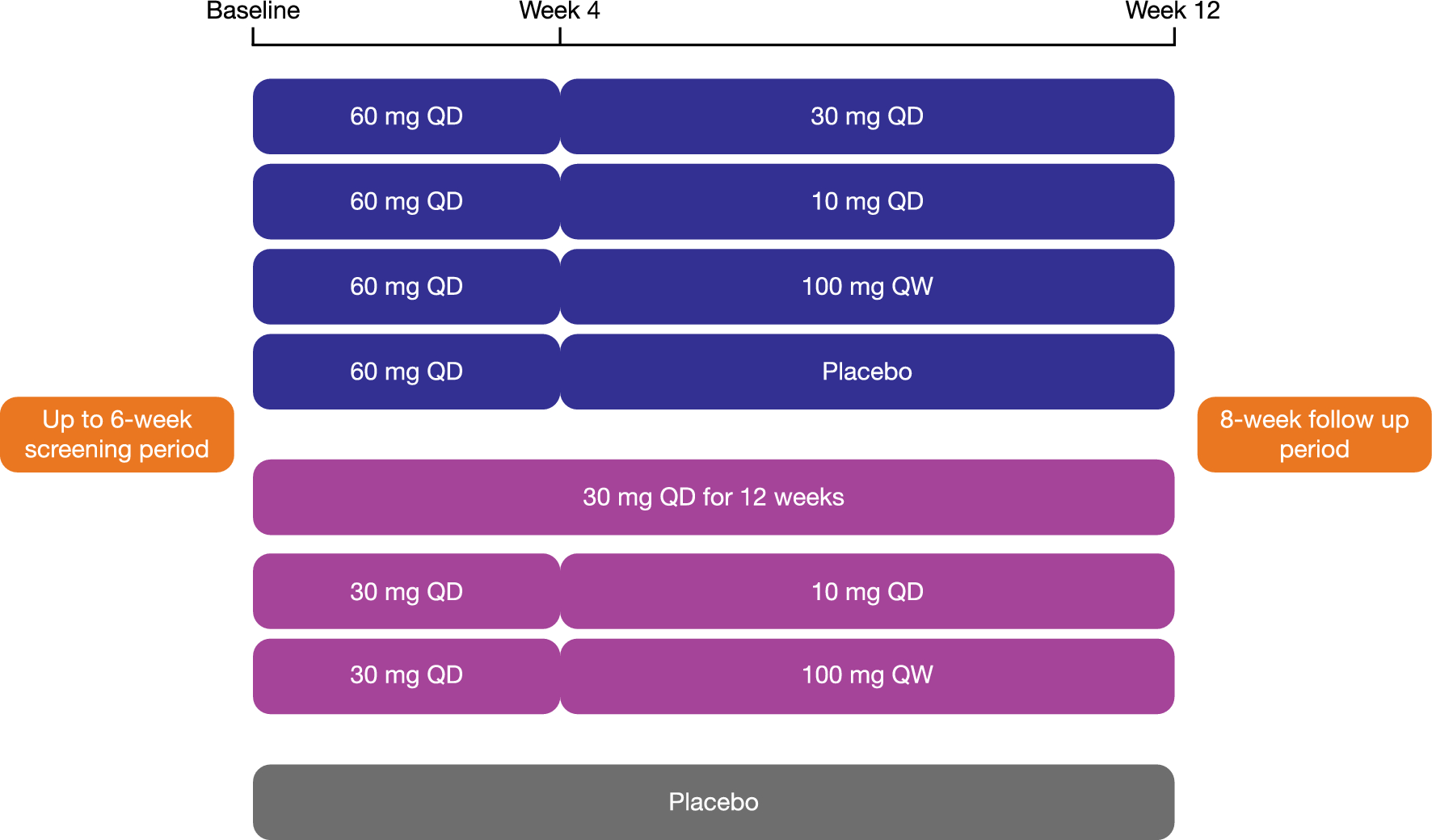
This PopPK analysis was based on data from three clinical trials (NCT01898364 [Phase 1][19], NCT02032524 [Phase 1/2][20] and NCT02782741 [Phase 3]) [12] in adolescent (only 1) and adult patients with LOPD with an addition of an open label, phase 2 trial (NCT03019406) in pediatric patients with IOPD (< 18 years), showing clinical decline and suboptimal clinical response to alglucosidase alfa (Table 1). In the phase 2 trial (25 week), patients received ascending doses of either intravenous (IV) AVAL (20 mg/kg [n = 6]; 40 mg/kg [n = 10]) q2w, or previously received stable dose of alglucosidase alfa (20 mg/kg q2w to 40 mg/kg every week [n = 6]). The four clinical studies included in the PopPK analysis are described in terms of size, dose, duration, and sampling timepoints in Table 1. All studies were conducted in accordance with Good Clinical Practice (GCP) guidelines and the ethical principles that have their origin in the Declaration of Helsinki. The protocols were approved by the ethics committee or institutional review board at each site, and all participants provided written informed consent.
Table 1 Studies included in the population pharmacokinetic analysis
Bioanalysis
The plasma concentrations of free AVAL were quantified by using validated fluorometric enzyme activity assay as described previously [18]. The assay was validated between 0.012 and 0.0125 (lower limit of quantitation, LLOQ) and 3.0 µg/mL. The antidrug-antibody (ADA) assay methods were developed according to the current standards for ADA investigation with the implementation of a three-tiered approach, i.e., a first testing method, a confirmatory assay and a final assay to determine ADA titers [18].
Population pharmacokinetic analysisSoftware
The PopPK analysis was performed using a nonlinear mixed effect modelling (NONMEM) software (version 7.4.1, Icon Development Solutions, Ellicott City, MD, USA) [21]. Statistical and graphical outputs were generated using the R programming and statistical language (version 3.6.3).
Model development, allometric scaling, and covariate screening
Model parameters were estimated using the first-order conditional estimation (FOCE) algorithm with interaction option as implemented in NONMEM [21]. Total PopPK dataset was obtained by supplementing the LOPD (adolescent and adult) dataset described in previous analysis [18] by IOPD (pediatric) dataset. The pharmacostatistical model (PSM) developed in the previous study [18] was used as an initial model for the present analysis by re-optimizing the parameters. The concentration versus time curves were described by a concatenated three-compartment model, with drug back redistribution from the third compartment to the central compartment. The elimination process was characterized by linear and non-linear kinetics in the central compartment. Log-normal inter-individual variability of the parameters was used.
Considering that the dataset included both adult and pediatric patients, time-varying bodyweight dependent allometric scaling of the PSM was tested before the covariate selection process by including the weight on clearance [CL] and distribution volume(s) [V] parameters using following equation:
$$TV(parameter) = \theta (parameter) \times }}} \right)^}$$
A sensitivity analysis was performed by optimizing or fixing the allometric scaling factor parameter θ(x) ([CL] = 0.75 and [V] = 1).
Potential PK covariates were then selected based on physiological and clinical relevance and included: age (years), gender, bodyweight (kg), renal function (measured by creatinine clearance normalized by body size or surface area, CLCRN), albumin (g/L), alanine amino transferase (IU/L), aspartate amino transferase (IU/L), alkaline phosphatase (IU/L), total bilirubin (µmol/L) and creatine kinase (IU/L). The baseline information was used for each covariate except for age and bodyweight for which both baseline and time varying values were considered. The occurrence of ADA, the disease type (LOPD versus IOPD) as well as previous treatment with alglucosidase alfa status were also investigated. Potential covariates were examined using stepwise selection, including the forward inclusion (alpha risk: 5%) and backward elimination (alpha risk: 0.1%) process.
Model verification and qualification
The robustness of the final PopPK model was qualified by goodness-of-fit (GOF) plots, quality criteria [bias, precision, or Absolute Average Fold Error (AAFE)], bootstrap analysis and visual predictive checks (VPCs) to ascertain the predictive power, model stability, and uncertainty in the parameter estimates. For the graphical assessment of the predictive ability of the model, 1000 simulated replicates of the observed dataset were generated, and the results were presented as time after the end of the doses (TAD) using prediction corrected VPC (pcVPC) and as baseline bodyweight using VPC method.
For the bootstrap analysis, 1000 replicate datasets were generated from the original dataset and the model was fit to each of these replicated datasets. Medians and corresponding non-parametric 95% confidence interval (CI) (2.5th to 97.5th percentiles) were assessed for each parameter based on the successfully minimized runs and compared to the parameter estimates of the final model.
Evaluation of individual exposures
After qualification, the model was used to calculate the individual exposures [maximal concentration (Cmax) and area under the curve in the 2-week dosing interval (AUC2W)] for each patient treated with AVAL (20 mg/kg or 40 mg/kg q2w) after a single dose over 2 weeks i.e., 336 h (virtual sampling every 0.1 h). The infusion rate was administered stepwise: 1 mg/kg/h for 30 min, 3 mg/kg/h for 30 min, and 5 mg/kg/h for 30 min and then 7 mg/kg/h to deliver the planned amount of the drug. The total infusion duration for 20 mg/kg and 40 mg/kg was 3.71 and 6.57 h, respectively. Bodyweight at the time the patients received their last dose (20 or 40 mg/kg) was considered for IOPD patients whereas baseline bodyweight was considered for LOPD patients. Descriptive statistics on exposure parameters were reported by dose, and variables such as age, bodyweight, gender, race, disease type, and previous treatment with alglucosidase alfa.
Virtual patient simulation analysis for alternative dosing regimen
Exposure parameters of AVAL (Cmax and AUC2W) were simulated with the final PopPK model to propose bodyweight dosing adjustments in pediatric patients. As limited number of patients were available for < 18 years, exposures were simulated by gender for selected staggered age (years) within each virtual population category. The equations, parameters, and variance-covariance matrix of the PopPK model was calculated through their corresponding bodyweight (kg) with the lowest and highest bodyweight set to the 5th and 95th percentiles as per Centre for Disease Control and Prevention (CDC) growth charts [22]. The virtual populations were generated using truncnorm package [23]. The simulations were performed using the mrgsolve package [24].
Simulations with different bodyweight cut-off (25, 30, 35 and 40 kg) were performed so as to identify the appropriate bodyweight cut-off achieving similar exposure of AVAL in adult patients across all groups. A total of 4018 virtual pediatric patients (1 to < 2 years, n = 1002; 2 to < 6 years, n = 1000; 6 to < 12 years, n = 1008; 12 to < 18 years, n = 1008) were generated for each cut-off simulation. Corresponding simulated exposure distributions were generated for ≥ 18 years (n = 1000, virtual patients) from the available adult patient data. Individual exposure parameters were computed after a single dose of 20 mg/kg for all virtual adult patients. Virtual pediatric patients were simulated at a single dose of 40 mg/kg (bodyweight <cut-off) and a single dose of 20 mg/kg (bodyweight ≥cut-off).



留言 (0)