
Remember me
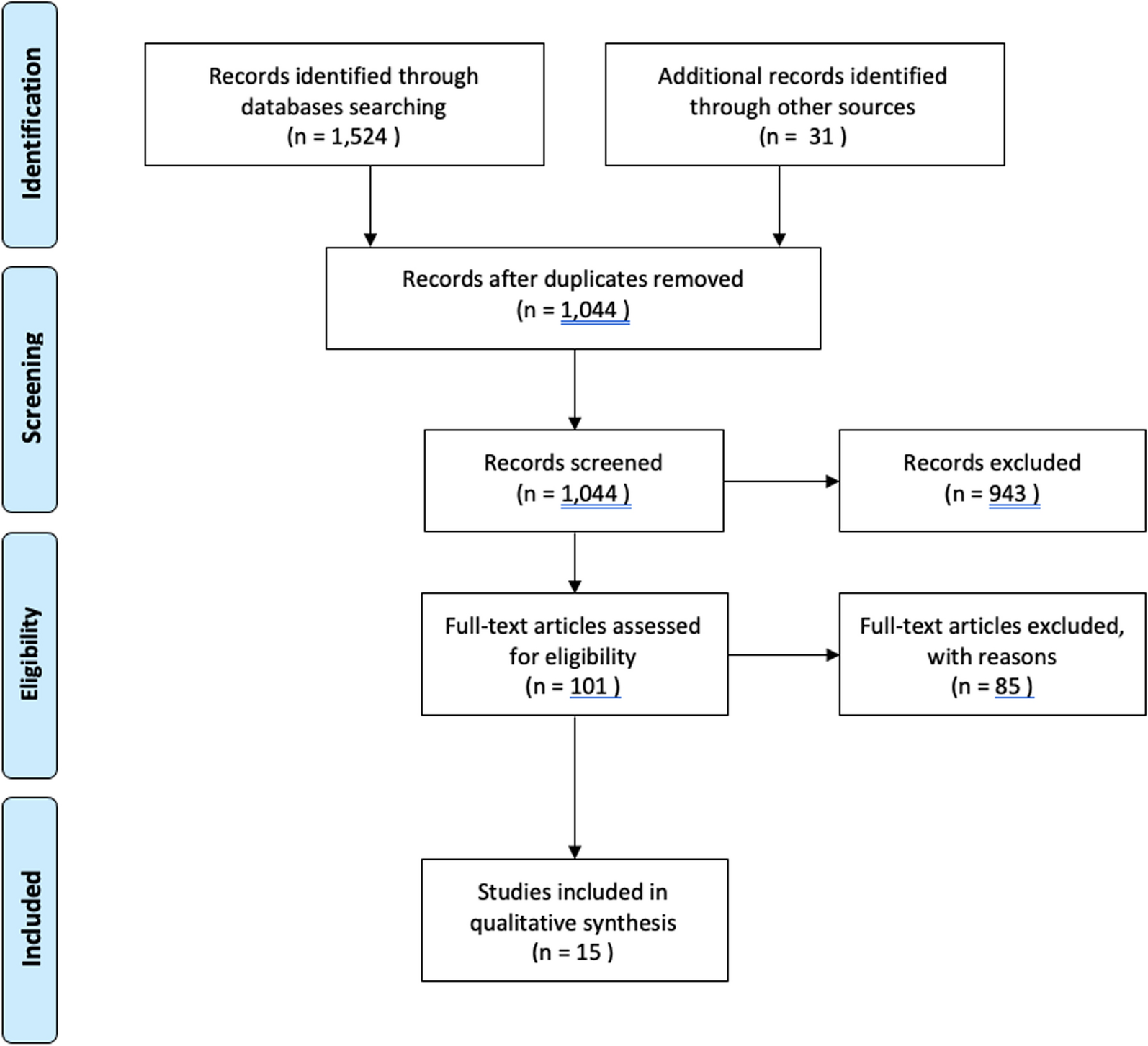







A total of 607 articles were identified via database searching and cross-referencing. After duplicate removal, 435 articles were screened by title and abstract, leaving 56 full texts to be assessed for eligibility. Thirty-five articles were excluded because of the following reasons: mixed surgical techniques (n = 17); anterograde drilling (n = 7); population not of interest (n = 6); case report (n = 4); letter to the editor (n = 1). Twenty-one studies fulfilled the inclusion criteria and were included in the qualitative synthesis. The PRISMA flowchart showing the selection process is presented in Fig. 1.
Fig. 1
PRISMA flowchart showing the study selection process
Assessment of risk of bias and quality of recommendationThe quality assessment of the included studies, conducted through the ROBINS-I tool for non-randomized studies, is reported in Table 2. Due to the considerable amount of retrospective case series (17 articles, 81%), there was a high likelihood of selection bias. The study's overall risk of bias score was low–moderate, indicating a moderate to good level of methodological quality.
Table 2 Risk of bias (ROBINS-I) for the case seriesSince most of the included articles were observational case series investigating only patients exposed to the intervention, the quality of evidence was rated as low to very low according to the GRADE framework (Table 3).
Table 3 Summary of selected studiesStudy characteristics and results of individual studiesThe literature concerning RD was mostly constituted by retrospective case series (17 articles, 81%) [6, 8, 12,13,14,15,16,17,18,19,20,21,22,23,24,25,26], classified as LOE IV. The remaining articles were equally divided into retrospective comparative studies (two articles, 10%) [7, 27] and prospective observational studies (two articles, 10%) [28, 29], both classified as LOE III (Table 3). The majority of the included studies were published in the last 20 years.
A total of 266 patients (271 ankles) were included in this review. When reported, the sex distribution was 99 (54%) males and 83 (46%) females. Mean age at surgery was available in all articles but one [7], and was found to be 28.2 years (range, 9–69). Final follow-up was on average 33 months, and was reported in all articles but four [7, 13, 20, 23].
Most of the osteochondral lesions were in the talus; only Takao et al. included lesions on both the talus and distal tibia [29]. Concerning the osteochondral lesions of the talus, a more detailed localization was provided in 16 articles as follows: 83% (144/174) medial, 15% (27/174) lateral, 2% (3/174) central. Antero-posterior localization was not considered when performing this calculation; therefore, lesions described as posteromedial or anterolateral were counted as medial and lateral, respectively.
Seven articles reported the mean size of the lesions, but in different ways [6, 8, 12, 16, 17, 28, 29]. To compare most of the articles, only the mean length of the lesions was considered; it was found to be 11.4 mm (Table 3).
Synthesis of resultsAmong the clinical and radiological parameters used in assessing surgical indication, 15 authors agreed that intact cartilage must be present to make patients eligible for RD [7, 8, 12, 14, 16,17,18,19,20,21,22,23,24,25,26,27].
The Berndt and Harty classification [30] was considered in four articles: two authors recommended surgical treatment in grades I–III [13, 17], whereas Masquijo and Geerling restricted the indication to only grades I and II [18, 25]. Regarding lesion size, only two authors set a threshold value to consider surgery, which ranged from 100 mm2 to 125 mm2 [7, 28]. Faldini et al. also extended surgical indication to wide osteochondral lesions with, theoretically, no size limit [8].
Osteochondral lesions were classified by applying different grading systems based on the available radiological imaging. The Berndt and Harty classification on a plain radiograph was used in six studies, with an average grade of 2.2 out of 4 [6, 14, 18, 19, 21, 23]. The Pritsch classification on arthroscopic imaging was used in five studies, with a mean grade of 1.6 [14, 17, 26,27,28]. Other less common grading systems applied are reported in Table 4.
Table 4 Indications and surgical procedureVarious evolutions of the original surgical procedures have been described by authors. RD was performed by inserting K-wires retrogradely under different navigation systems. Fluoroscopy was the most extensively used method (13 articles) [7, 8, 12, 15, 17,18,19,20,21, 24, 26, 27]. In terms of fluoro-free surgeries, magnetic resonance imaging (MRI) was used in one article [6], and computer-assisted navigation was used by three authors [13, 23, 25]. Finally, Microvector was used by Beck et al. [28].
Different adjuvants were employed after RD. Cancellous bone grafting was utilized to plug the bone defect by four authors [7, 17, 21, 29]. Saxena et al. also injected platelet-rich plasma onto the bone graft [7]. Faldini et al. retrogradely positioned a hyaluronan scaffold soaked in bone marrow aspirate concentrate and, in addition, filled the talar tunnel with cancellous bone graft [8]. Other injectable solutions were applied alone in a retrograde fashion: Grafton™ gel by Berlet et al. [24] and PRO-DENSE® by Beck et al. [28] (Table 4).
In order to compare the clinical outcomes, 12 articles (195 ankles) preoperatively recorded the AOFAS score, and 12 articles (198 ankles) recorded it postoperatively. The mean preoperative value was 64.2 (range, 0–87), which increased postoperatively to 88.8 (range, 48–100) [7, 13, 15,16,17,18, 21, 24, 25, 27,28,29].
Pain assessment was conducted through VAS by six authors (78 ankles), and the results were on average 6.9 and 2.2 before and after surgery, respective
Comments (0)