
Remember me

Liver transplantation is the most effective treatment for end-stage liver disease, hepatocellular carcinoma, and fulminant hepatic failure. The survival rate of liver transplant recipients has improved with advances in immunosuppressive therapy and surgical techniques (Serper et al., 2022). In 2021, the 1-year and 5-year rates of survival for liver transplant recipients in Korea were 86.9% and 77.1%, respectively (Korean Network for Organ Sharing, 2022). Unlike in Europe and the United States, where deceased donor liver transplantations are widespread, living donor liver transplantations from family members are often practiced in South Korea (Ryu et al., 2019). In 2021, living donor liver transplants accounted for 76.4% of all liver transplants in Korea, with 98.9% of these originating from family donations. Of these family donations, 69.0% were from children or grandchildren, 11.9% were from spouses, and 9.6% were from siblings (Korean Network for Organ Sharing, 2022). In the family-oriented culture prevalent in Asian countries such as Korea, living organ donation to family members is instinctively natural because of familial attachments (Rela & Rammohan, 2021).
Liver transplant recipients often experience a variety of symptoms, including immunosuppressive side effects, rejection, complications, and sleep disturbances, with the latter particularly common (Bhat et al., 2015; Serper et al., 2022). Sleep disturbance induces fatigue in liver transplant recipients, reducing daytime concentration and physical activity (Demir & Saritas, 2022; Lin et al., 2017). In addition, sleep disturbances are associated with noncompliance with prescribed immunosuppressants (Burkhalter et al., 2014). Furthermore, liver transplant recipients with poor sleep quality have been shown to have a significantly lower physical and mental quality of life compared with recipients with favorable sleep quality (Akahoshi et al., 2014; Burkhalter et al., 2017). Despite the seriousness of poor sleep quality, sleeping difficulties are generally underdiagnosed and not managed effectively (Reilly-Spong et al., 2013). It has been estimated, based on the Pittsburgh Sleep Quality Index scores, that 33% (Burkhalter et al., 2017) to 71% (Mendes et al., 2014) of liver transplant recipients are affected by sleep disturbances.
After liver transplantation, recipients must take immunosuppressants for the rest of their lives to reduce the rate of rejection graft loss and improve survival. However, the use of long-term immunosuppressants causes complications such as infections, hyperglycemia, hypertension, and nephrotoxicity (Herzer et al., 2020). In addition, recipients experience subjective symptoms from immunosuppressants such as pain, itching, tremors, mood swings, fatigue, nausea, and vomiting (Gunn et al., 2021), which influence sleep quality in recipients. For example, pain was shown to triple the risk in recipients of inadequate total sleep time, as measured by objective actigraphy (Reilly-Spong et al., 2013). Furthermore, weight gain, a typical symptom experienced by immunosuppressants such as steroids, has been shown to negatively affect total sleep time, sleep efficiency, and sleep onset latency in transplant recipients (Reilly-Spong et al., 2013).
Depression, which causes persistent sadness and loss of interest, is a common psychiatric disorder arising after liver transplantation. Heo et al. (2018) reported depression as the most frequently reported psychiatric comorbidity in the post-liver-transplant period, affecting 37.5% of participants. In addition, previous studies have reported a strong relationship between depressive symptoms and sleep quality in transplant recipients (Burkhalter et al., 2017; Zhu et al., 2020). Cordoza et al. (2021) found depression to be a significant factor associated with poor sleep quality in patients with solid organ transplantation.
Social support is important for patients, and especially for those experiencing stress. Social support, including emotional, instrumental, informational, and appraisal, may be provided by a patient's family members, friends, healthcare providers, or others (Swanson et al., 2018). Among the types of social support, family support plays an important role in providing transplant recipients with emotional, physical, and financial support (Golfieri et al., 2019), helping them find solutions and recover from illness and alleviating psychological problems such as stress and depression. In addition, family support increases adherence to treatments, which has a positive effect on the rate of survival in recipients (Golfieri et al., 2019). Furthermore, family support not only provides emotional and economic support but also improves self-management efficacy in facets such as sleep (H. Kim et al., 2015; Zhang et al., 2022). Therefore, family support may help improve sleep quality in Korean liver transplant recipients.
The conceptual framework used in this study was based on the theory of unpleasant symptoms (TOUS) and was designed to provide useful information for developing effective interventions to prevent, manage, and improve unpleasant symptoms (Lenz et al., 1997). This framework includes three main components: unpleasant symptoms, the affecting factors that precede these symptoms, and performance outcomes. The three categories of affecting factors, including physiological, psychological, and situational, affect the abovementioned unpleasant symptoms. In this study, on the basis of a review of the literature, unpleasant symptoms refer to low sleep quality, physiological factors refer to symptom experience, psychological factors refer to depression, and situational factors refer to family support.
In prior studies of factors affecting sleep quality in transplant recipients, the main influencing demographic factor identified was gender, with female liver transplant recipients experiencing longer sleep latency and greater sleep disturbances than male recipients (Bhat et al., 2015; Mendes et al., 2014). In terms of clinical variables in liver transplant recipients, body mass index has been associated with low sleep quality (Reilly-Spong et al., 2013), whereas restless leg syndrome and minimal hepatic encephalopathy have been identified as factors influencing sleep problems (Akahoshi et al., 2014). In terms of psychological factors, recipients with high levels of anxiety, stress, and depression have been shown to be affected by poorer sleep quality (Burkhalter et al., 2017; Demir & Saritas, 2022; Mendes et al., 2014). However, these prior studies have focused solely on either physiological or psychological factors, which has precluded the identification of overall factors. Few studies have investigated the relationships between physiological, psychological, and situational factors and sleep quality in liver transplant recipients. In addition, few studies have been conducted on quality of sleep in liver transplant recipients in Korea, where living donor liver transplantation has been widely performed.
Therefore, this study was developed to assess the prevalence of sleep difficulties and to identify, using the TOUS, the influence of symptom experience (physiological factors), depression (psychological factors), and family support (situational factors) on sleep quality in Korean liver transplant recipients.
Methods Research DesignIn this study, a correlational, cross-sectional design was used to evaluate the influence of symptom experience, depression, and family support on sleep quality in Korean liver transplant recipients.
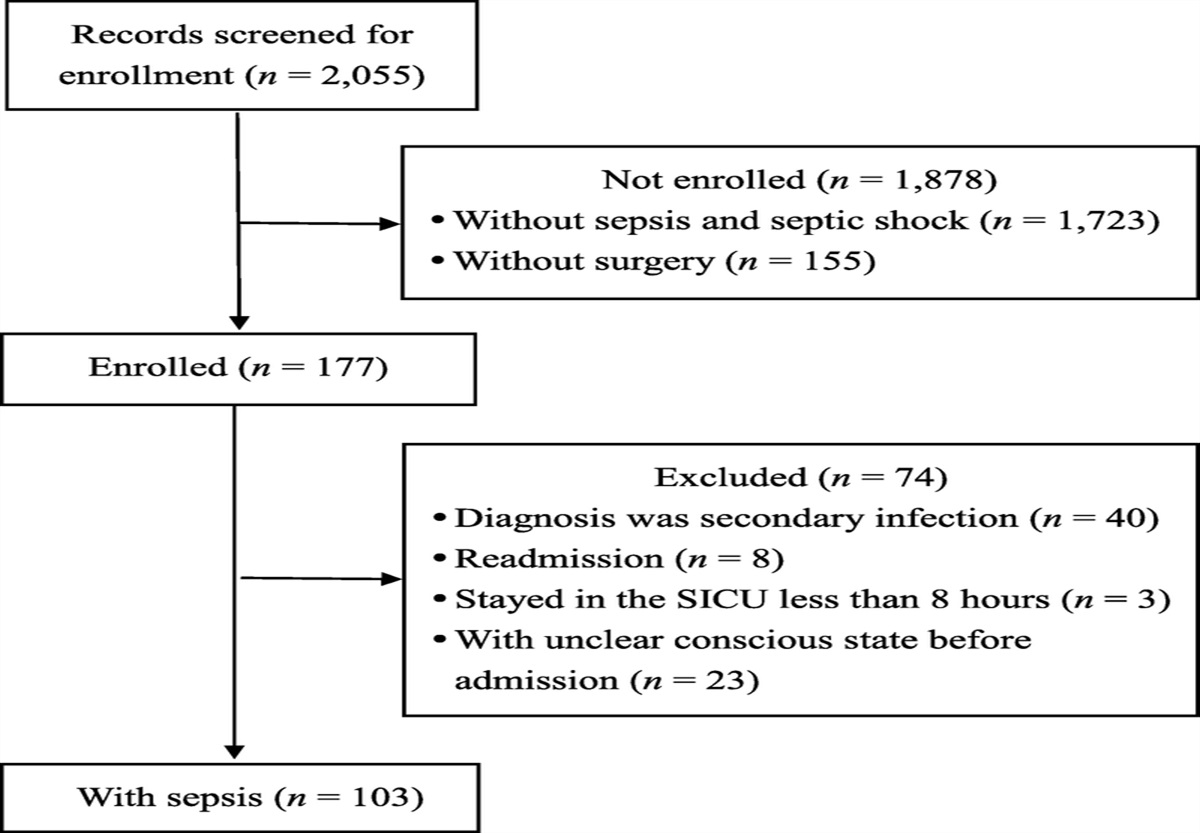
Setting and SampleOne hundred forty-nine adult liver transplant recipients were recruited to participate in this study from the outpatient transplant clinic of a Korean tertiary hospital from September to November 2019. Eligibility criteria included (a) being at least 18 years old, (b) at least 1 month after liver transplantation, (c) able to read and understand the Korean language, and (d) agreeing to participate and provide informed consent. Those who required emergency treatment for serious diseases such as sepsis and active lung disease were excluded.
The sample size was calculated using G*Power 3.1.9.2 (Faul et al., 2009). For a multiple linear regression with 14 expected independent variables, a medium effect size (Cohen's f2 = 0.15), a significance level of .05, and a power of 0.80 were established. The result of the power analysis indicated the study should be performed with at least 135 participants. Therefore, 149 participants were recruited, considering an attrition rate of 10%.
MeasurementA questionnaire covering demographic and clinical characteristics, sleep quality, symptom experience, depression, and family support was used to collect the data for this study.
Demographic and clinical characteristicsThe demographic characteristic data collected from participants included age, gender, educational level, marital status, living arrangements, main caregiver, religion, employment, smoking and alcohol use, coffee intake, monthly household income, and use of medications for sleep. The clinical characteristic data collected on participants included donor type, cause of liver transplantation, years since liver transplantation, comorbidities, number of immunosuppressants taken, use of psychiatric medications, and body mass index and were obtained using electronic medical records.
Sleep qualityThe 19-item Korean version of the Pittsburgh Sleep Quality Index (PSQI-K; Sohn et al., 2012) was used to assess the sleep quality of the participants during the previous month in seven components, including sleep quality, latency, disturbances, duration, habitual sleep efficiency, use of sleeping medication, and daytime dysfunction. The participants were asked to rate each component using a 4-point Likert scale, ranging from 0 to 3 points with a maximum overall score of 21 points. In line with prior research, scores greater than 5 were associated with poor sleep quality (Buysse et al., 1989). The Cronbach's α of the PSQI-K was .84 in a prior study (Sohn et al., 2012) and .77 in this study.
Symptom experienceThe 59-item Modified Transplant Symptom Occurrence and Symptom Distress Scale (MTSOSD-59R; Dobbels et al., 2008) was used to assess symptom experience with regard to the side effects of immunosuppressive regimens administered during the previous month. In this scale, each item represents a symptom, which is scored in terms of both symptom occurrence and symptom distress. In this study, the total score for symptom distress was used to assess symptom experience. The items used a 5-point Likert scale, ranging from 0 (not distressing at all) to 4 (extremely distressing) for symptom experience. The total possible score, calculated as the sum of the symptom distress item responses, ranges from 0 to 236 points, with higher scores indicating greater symptom experience. In addition, the frequency of symptom distress was identified to determine the symptoms that most distressed the participants. For each MTSOSD-59R item, those participants who recorded responses of zero were identified with no symptom distress and categorized as “zeros,” whereas those who recorded a score greater than zero were categorized as “nonzeros.” Frequency of symptom distress was defined as the number of “nonzeros” in the sample. For example, if 79 of 149 participants gave a nonzero score for “fatigue symptoms,” then 53.0% of the participants would be recorded as reporting “fatigue” as a distressing symptom. Because the items of the MTSOSD-59R were deliberately composed of various contents and not homogeneous, Cronbach's α is not a useful test of validity. The content validity for all of the 59 items was ≥ .8 (Moons et al., 2001).
DepressionThe 20-item Korean version of the Center for Epidemiologic Studies Depression Scale-Revised (CESD-R; Lee et al., 2016) was used in this study to assess depression during the previous 2 weeks. Each item of the CESD-R uses a 5-point Likert scale scoring system, ranging from 0 (not at all or less than 1 day) to 4 (nearly daily for 2 weeks). The total possible scores for this scale range from 0 to 80, with higher scores indicating higher levels of depression. The Cronbach's α of the CESD-R was .98 in Lee et al. (2016) and was .91 in this study.
Family supportThe 12-item Family Support Scale (O. S. Kim, 1993) was originally developed for hemodialysis patients and has been used in Korea to measure level of family support for liver transplant patients (H. Kim et al., 2015). This instrument measures family support provided to patients in the facets of informational, emotional, medication, and financial support; esteem; and social network. Each item is scored using a 5-point Likert scale that ranges from 1 (not true at all) to 5 (completely true). The total possible score, calculated by summing the individual item responses, ranges between 12 and 60 points, with higher scores indicating a higher level of family support. The Cronbach's α of the Family Support Scale was .94 in O. S. Kim (1993) and .94 in this study.
Data CollectionThe researcher explained the purpose and procedure of this study to eligible participants in the outpatient transplant clinic. The data were collected using self-report questionnaires from those who volunteered to participate. The participants required an average of 30 minutes to complete the questionnaire. After the participants completed the questionnaire, the researcher checked that all items had been answered and asked the participants to fill in any missing items to reduce the amount of missing data.
During the process of assessing depression in the participants, the professor of transplant surgery, one of the researchers involved in this study, was informed that psychiatric treatment was necessary for 28 of the participants with suicidal thoughts, as indicated by their responses to the questionnaire items: “I wish I were dead” or “I have wanted to hurt myself.”
Ethical ConsiderationsThis study was approved by the institutional review board (Approval No. SMC 2019-08-138-003) of the study hospital. Before data collection, the participants were informed of the purpose, risks, and benefits of research participation, and written consent was obtained. The participants were assured that participation was voluntary, that data collected in this study would not be used for any purpose outside this study, and that they could end their participation at any time. The signed consent forms and completed questionnaires were sealed and collected. The personal information of the participants was coded, and the data were managed using serial numbers to ensure anonymity and confidentiality.
Data AnalysisFor the descriptive statistics, all of the data were summarized as either mean and standard deviation or frequency and percentage. For the inferential statistics, independent t test and one-way analysis of variance were performed to compare differences within characteristics, and the Scheffé's post hoc test was performed. Pearson correlation coefficient analysis was conducted to determine the correlations between sleep quality and, respectively, symptom experience, depression, and family support. Finally, multiple linear regression analysis was conducted to identify the factors affecting sleep quality. In all of the analyses, statistical significance was set at p < .05, with two tails. All data were analyzed using IBM SPSS Statistics Version 25.0 (IBM Inc., Armonk, NY, USA).
Results Characteristics of ParticipantsThe demographic and clinical characteristics of the participants are shown in Table 1. One hundred forty-nine post-liver-transplantation participants (105 male and 44 female) were included in the analysis. The age range of the participants was 22–76 years (M = 58.19 years, SD = 8.76 years), most had received living donor liver transplantation (81.9%), and almost half were cases in which children had donated to their parents (49.7%). The posttransplant period ranged from 1 to 231 months (M = 6.17 years, SD = 5.25 years), with 55.0% of the participants having received their liver transplantation at least 5 years before participation and 17.4% having received their liver transplantation less than 1 year before participation.
Table 1 - Demographic and Clinical Characteristics of the Participants (N = 149) Variable n % Sleep Quality t or F p Mean SD Age (years; M and SD) 58.19 8.76 1.46 .147 a < 65 122 81.9 7.39 4.30 ≥ 65 27 18.1 6.11 3.32 Gender −2.55 .013 a Male 105 70.5 6.57 3.84 Female 44 29.5 8.57 4.57 Educational level 1.96 .144 b ≤ Middle school 31 20.8 6.87 3.91 High school 51 34.2 8.08 4.74 ≥ College 67 45.0 6.60 3.71 Marital status −0.88 .378 a Married 128 85.9 7.04 4.16 Unmarried 21 14.1 7.90 4.12 Living arrangement −0.68 .497 a Living with others 134 89.9 7.24 4.24 Living alone 15 10.1 6.47 3.38 Main caregiver −0.58 .564 a Spouse 124 83.2 7.07 4.21 Others 25 16.8 7.60 3.91 Religion −0.51 .612 a Yes 80 53.7 7.00 3.83 No 69 46.3 7.35 4.52 Employment −1.74 .084 a Yes 79 53.0 6.61 4.20 No 70 47.0 7.79 4.04 Smoking 0.36 .697 b Nonsmoker 95 63.8 7.37 4.14 Ex-smoker 45 30.2 6.87 4.43 Current smoker 9 6.0 6.44 2.92 Alcohol use 0.67 .515 b Nondrinker 70 47.0 7.36 3.99 Ex-drinker 64 43.0 7.22 4.44 Current drinker 15 10.0 6.00 3.72 Coffee intake 1.35 .263 b Never 32 21.5 7.19 4.04 1–2 cups per day 93 62.4 7.47 4.15 ≥ 3 cups per day 24 16.1 5.92 4.27 Household income (10,000 KRW/month) 0.34 .713 b < 200 42 28.2 7.26 4.03 200–399 52 34.9 6.79 3.78 ≥ 400 55 36.9 7.44 4.61 Donor of liver transplantation 0.40 .879 b Children 74 49.7 7.01 4.32 Spouse 15 10.1 8.13 4.17 Siblings 14 9.4 7.71 4.08 Relatives 13 8.7 6.08 3.17 Parents 2 1.3 9.00 8.49 Others 4 2.7 7.00 4.83 Deceased 27 18.1 7.15 4.06 Cause of liver transplantation 0.97 .411 b HCC 27 18.1 7.22 3.49 LC 58 38.9 7.24 4.44 HCC + LC 56 37.6 6.73 4.09 Fulminant hepatic failure 8 5.4 9.38 4.50 Years since LT (M and SD) 6.17 5.25 2.50 .086 b < 1 26 17.4 8.19 3.86 1 to < 5 41 27.6 7.85 4.39 ≥ 5 82 55.0 6.49 4.05 Comorbidities 0.70 .553 b DM 38 25.5 7.16 4.25 HTN 27 18.1 7.81 4.91 DM + HTN 3 2.0 4.33 2.08 None 81 54.4 7.05 3.90 Number of immunosuppressants taken 2.65 .074 b 1 11 7.4 6.91 3.08 2 97 65.1 6.66 4.18 ≥ 3 41 27.5 8.41 4.16 Use of psychiatric medications −0.90 .371 a Yes 5 3.4 8.80 4.60
Comments (0)