
Remember me
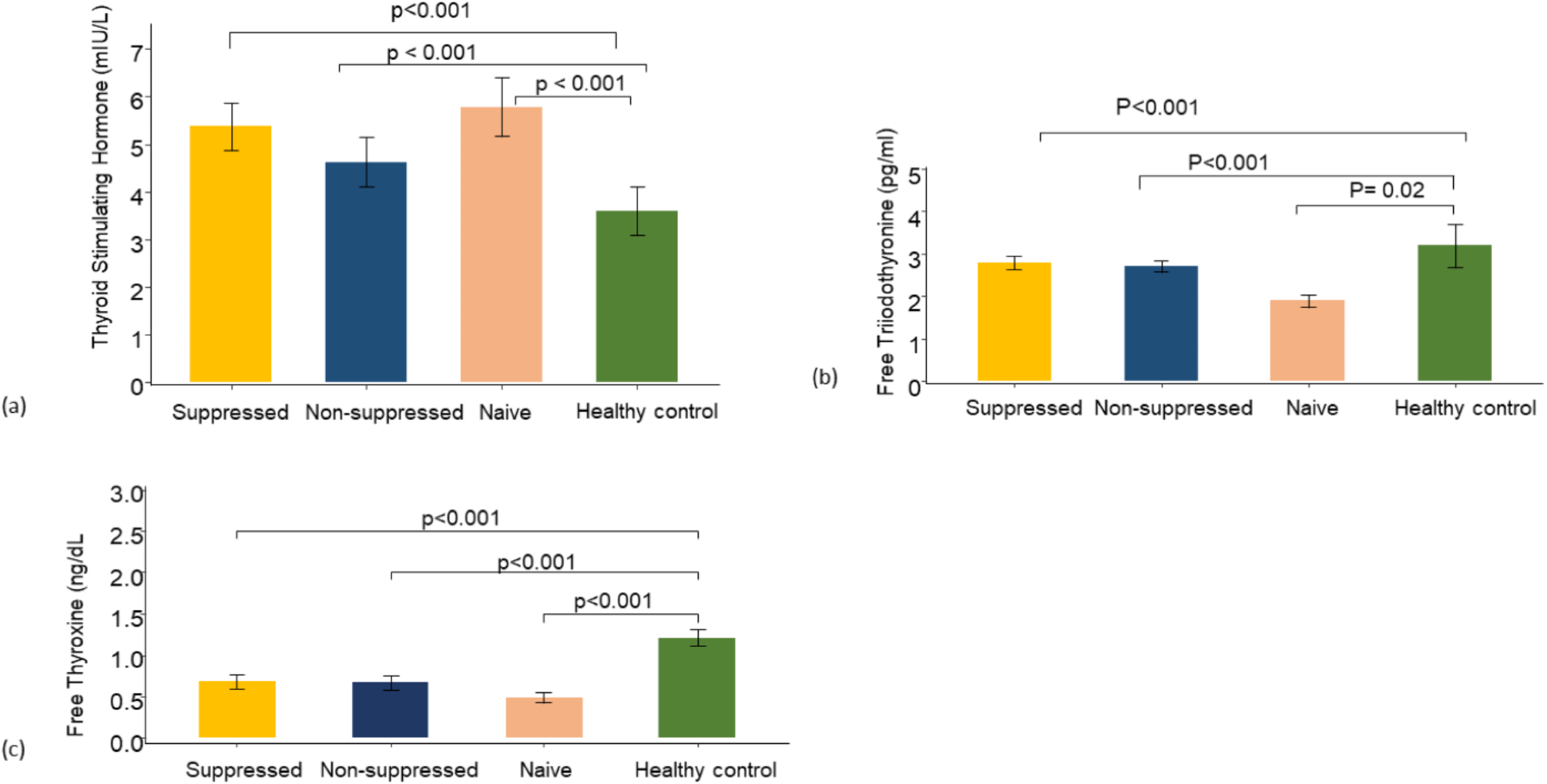
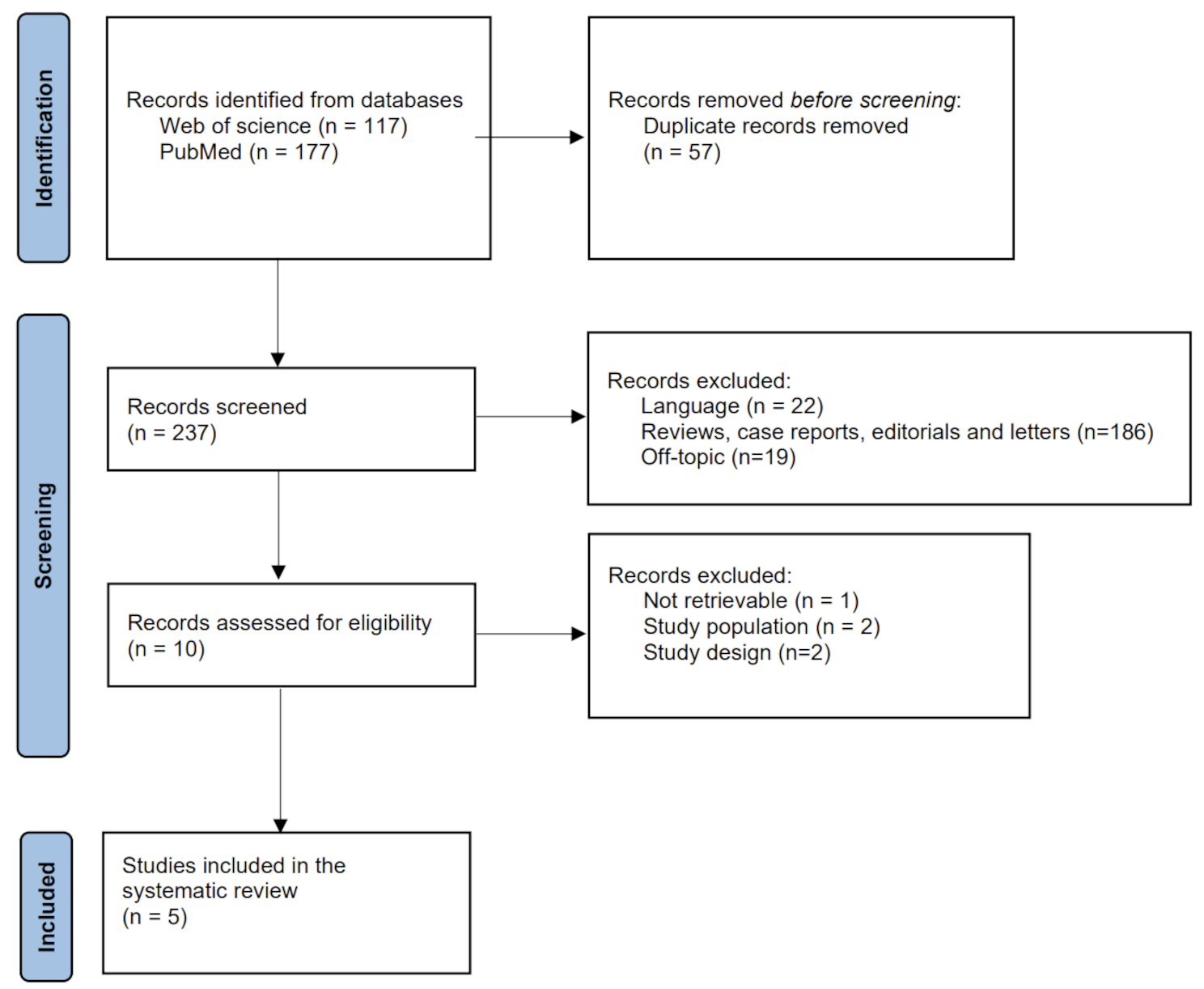
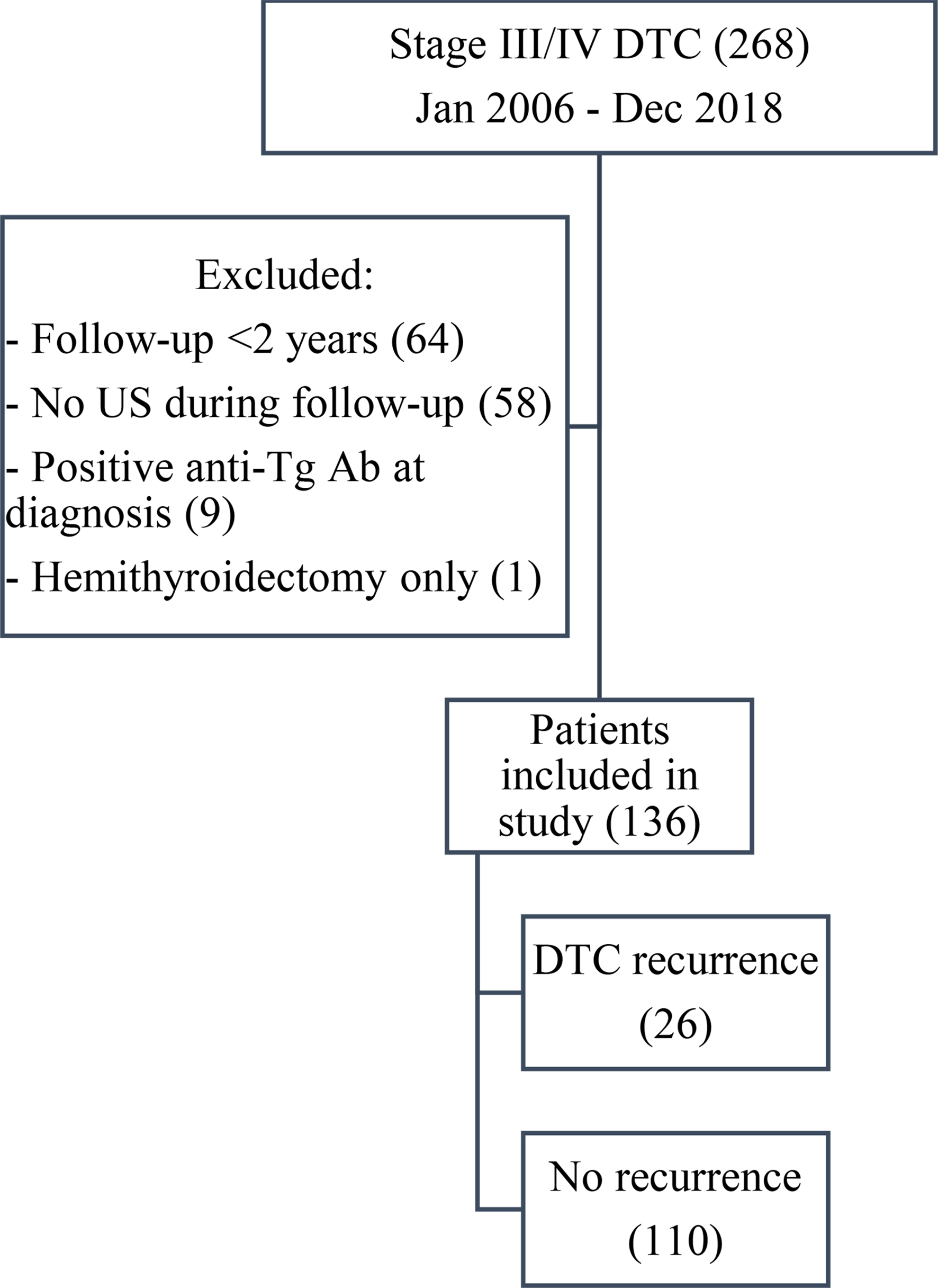
Fifty-one nonconsecutive AIS patients were consented for this study, six met exclusion criteria (Fig. 1), and forty-five were included in the study. This study was approved by the local institutional review board. We evaluated thyroid function in a longitudinal fashion, collecting serum TSH, fT3, and fT4 in the hyper-acute (within 24 h of patient’s last known well), acute (2–5 days after admission), and chronic (3–6 months) stages of ischemic stroke. As previous studies indicated that metabolic markers altered in ischemic stroke reach normal levels by 90 days, chronic stage values may represent baseline thyroid function [9, 10]. TSH was measured by immunoradiometric assay and fT3, fT4 were measured by radioimmunoassay in the local laboratory. Normal ranges are as follows: TSH (0.35—4.94 μIU/mL); fT3 (1.71–3.71 pg/ml); fT4 (0.7–1.5 ng/dL).
Fig. 1
Diagram of study enrollment from 2016 to 2018
Study was performed from 2016 to 2018 at Comprehensive Stroke Center, each patient presented as “stroke alert”, a process in which acute stroke patients are evaluated for thrombolysis and endovascular thrombectomy, and initiated within 24 h of time last known well. Hyper-acute and acute stage blood samples were collected during inpatient stay, while chronic stage samples were collected during follow-up clinic visit. We collected patients demographic (age, gender, ethnicity), and clinical (hypertension, hyperlipidemia, diabetes mellitus, smoking, previous history of AIS, atrial fibrillation, IV thrombolysis, and endovascular thrombectomy status) information. For ischemic stroke definition, patients underwent diffusion brain MRI within 48 h of hospital admission. All patients received computed tomography angiogram. We used the National Institutes of Health Stroke Scale (NIHSS; 0–42 points reflecting none and the most severe neurological deficit) to assess stroke severity at presentation [11]. During follow-up visit, we also reviewed patients’ charts to assess for recurrent stroke.
We excluded patients with: (1) hemorrhagic conversion of ischemic stroke and formation of parenchymal hematoma defined by Heidelberg bleeding classification [12]; (2) systemic infection at presentation or during admission with fever > 38.0 °C, elevated white blood cells, diagnosis of pneumonia, or urinary tract infection; (3) recurrent stroke in chronic stage; and (4) chronic thyroid problems, including patients receiving thyroid hormone supplementation, antithyroid medications, corticosteroids, lithium, metformin and amiodarone.
Statistical analysisThe clinical and demographic variables were summarized using means for continuous variables, while the numbers and percentages were reported for categorical variables. We used mixed regression model to evaluate change in thyroid function (TSH, fT3, fT4) from hyper-acute, to acute and chronic stages of ischemic stroke. In addition to age, ethnicity, hypertension, diabetes, smoking and body mass index (BMI), we used presenting NIHSS as a covariate to evaluate whether stroke severity is associated with change of TSH, fT3, and fT4. Average values of TSH, fT3, fT4 and NIHSS are reported with standard error. All analyses were performed using SAS version 9.4 M5. Statistical significance was assessed with a p-value of 0.05.
Comments (0)