
記住我

Congenital factor VII (FVII) deficiency is a rare coagulation disorder characterized by low or absent levels of clotting FVII or by nonfunctional circulating FVII [1,2]. First described in 1951 [3], the disorder occurs in both men and women, and has a global prevalence of 1 per 500 000 persons [4,5].
Bleeding phenotypes associated with congenital FVII deficiency are heterogeneous in terms of both location and severity [6], but can be disabling and/or life-threatening [7]. Patients with mild congenital FVII deficiency may be asymptomatic in the absence of surgery or trauma, while those with a severe deficiency may experience spontaneous and life-threatening hemorrhages [8]. Severe bleeding typically occurs in patients with homozygous or compound heterozygous mutations in both FVII alleles, with a circulating FVII activity of 2 IU/dl or less of normal levels [9].
In the past, plasma-based therapies such as fresh frozen plasma, plasma-derived FVII concentrates or prothrombin complex concentrates were the available treatment options for patients with FVII deficiency [10]. Currently, the most commonly administered treatment option is recombinant activated FVII (rFVIIa) (NovoSeven®, Novo Nordisk A/S, Bagsværd, Denmark) [6], which is indicated in Japan for the treatment of bleeding and for the prevention of bleeding during surgery/invasive procedures in patients with congenital FVII deficiency [11].
In 2020, 122 patients with FVII deficiency were reported in Japan [12]. Despite this, the majority of published reports describing the symptoms and treatment of congenital FVII deficiency relate to patients in Europe, while only a small number of publications describing data from Asian countries are available [13]. In this prospective observational study, data for 55% of the 64 patients registered in 2011 in Japan with congenital FVII deficiency who were treated with rFVIIa for bleeding episodes and/or the prevention of bleeding during surgery were collected for analysis [14].
Materials and methods Study designThis was a multicenter, observational study to evaluate the safety and hemostatic effectiveness following rFVIIa treatment in patients with congenital FVII deficiency. This study was conducted to address regulatory requirements as part of the postmarketing commitment to the Japanese Pharmaceuticals and Medical Devices Agency (PMDA). The current observational study was designed in accordance with the mandates and approval of the PMDA. Conducted at 30 sites in Japan, patients were enrolled between 01 March 2011 and 30 June 2013. Data were collected retrospectively from the approval date of the study drug, 12 March 2010 (if applicable), and annually after patient enrolment until 30 September 2014 (NCT01312636).
Recruitment was based on the Japanese national survey 2011, which reported 64 patients with congenital FVII deficiency in Japan [14]. All registered patients with congenital FVII deficiency receiving rFVIIa during the collection period, regardless of baseline FVII activity, were eligible for inclusion and the use of concomitant medication was permitted. Exclusion criteria were septicemia and a history of hypersensitivity to any of the product components, as per the relative contraindications listed in the NovoSeven® Japanese prescribing information [11].
The study protocol was approved by the local institutional review board or independent ethics committee at each participating institution. Prior to initiation of trial-related activities, signed informed consent was obtained from the patient, next of kin or legally acceptable representative, as per protocol.
As an observational study, the frequency and timing of patient visits were performed according to accepted routine clinical practice for patients with congenital FVII deficiency. Only data recorded as part of normal standard practice were collected and as such clinicians were under no obligation to test for safety markers such as D-dimer or FVII inhibitory antibodies. Data from the enrolment visit (visit 1; 0 months) comprised baseline patient demographics, while further study data were gathered at each annual patient assessment until the final visit (4 years).
The study was conducted in accordance with the Declaration of Helsinki, Good Pharmacoepidemiology Practices [15] and Good Postmarketing Study Practice [16].
Study endpointsThe primary endpoints of the study were assessed using available clinical laboratory testing results of patient blood samples and included the presence or absence of inhibitory alloantibodies to FVII. Patients did not undergo any additional testing for the purposes of this study, with all blood sampling and clinical laboratory testing performed at the discretion of the treating physician. Any thromboembolic events were assessed in relation to rFVIIa administration: Thromboembolic events were defined as clinical signs, laboratory indications and investigations indicating arterial or venous thrombosis.
Secondary endpoints were assessed by the evaluation, where available, of measurements recorded at each visit except visit 1. These included the hemostatic effectiveness of rFVIIa for the treatment of bleeding episodes and for treatment in the surgical setting. Hemostatic assessments of treatment for bleeding episodes (each treatment modality) and minor/major surgery (first and/or second treatment modality) were evaluated in accordance with per protocol effectiveness definitions (Supplementary Table 1, https://links.lww.com/BCF/A156). Changes in laboratory parameters, which were evaluated after rFVIIa treatment, included the prothrombin time-international normalized ratio (PT-INR), activated partial thromboplastin time, FVII activity, and platelet count and fibrinogen level. The presence, type and severity of all serious adverse events (SAEs) and adverse events were evaluated, excluding thromboembolic events, which were analyzed separately as a primary endpoint.
rFVIIa treatmentIn Japan, at the time of the study, rFVIIa treatment was available in three injectable vials: 1 , 2 or 5 mg. It was anticipated that rFVIIa would be administered to treat bleeding episodes according to the Japanese package insert: 15–30 μg/kg intravenous rFVIIa every 4–6 h until hemostasis was achieved. Depending on the type and extent of bleeding, the dose and frequency of on-demand injections could be adjusted as deemed necessary by the treating clinician; however, due to a lack of clinical data in patients receiving more than one dose, further doses were to be administered with caution [11].
Data analysesDescriptive analyses of the baseline and follow-up data were presented in tabular form. Mean, standard deviation, median, maximum and minimum were also tabulated for each measurement parameter. Missing and incomplete data were excluded, while data up to discontinuation were included for discontinued patients.
The subject-level analysis data sets for the research presented in the publication are available from the corresponding author on reasonable request.
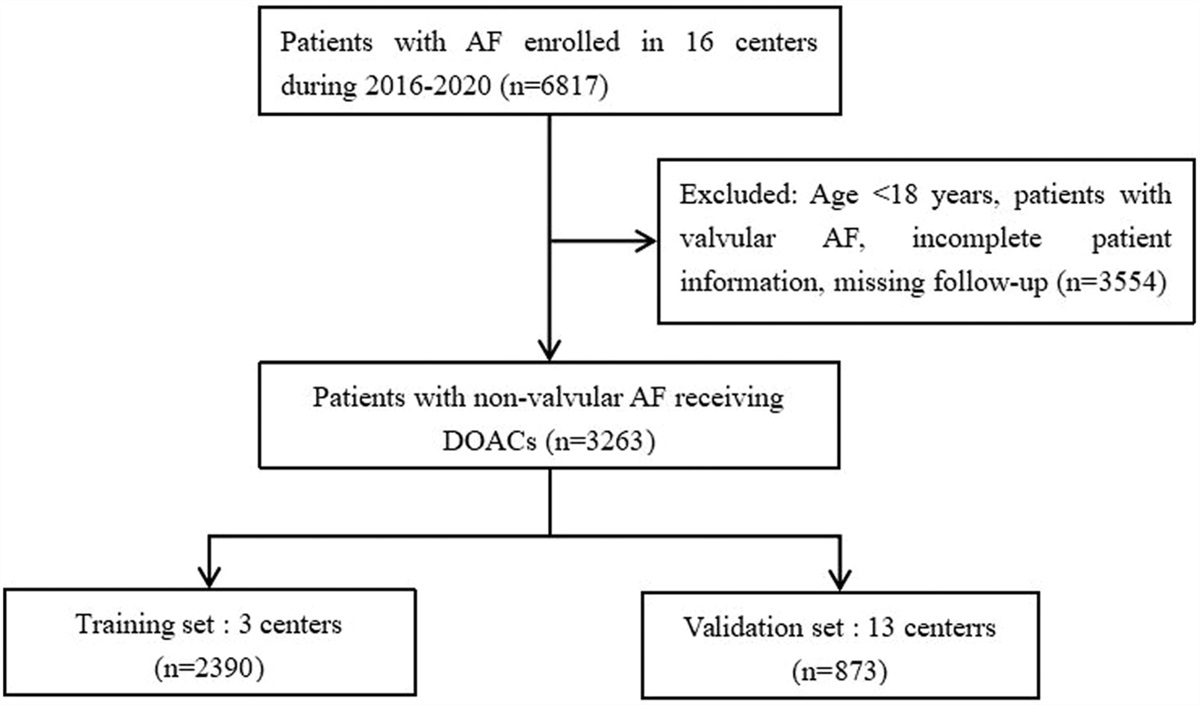
Results Patient dispositionOf the 64 patients with congenital FVII deficiency registered in 2011 in Japan [14], 36 patients were eligible for enrolment in the study. One patient was excluded, as the study site did not accept an amendment to the protocol, resulting in 35 patients, of whom 23 provided a signed informed consent form (Fig. 1). One study site declined to be involved in the analyses for this publication, resulting in a total of 20 patients included in this analysis. Patients were retrospectively analyzed, with a mean follow-up of 11 months (range 1–49 months). A full list of participating sites can be found in Supplementary Table S2, https://links.lww.com/BCF/A156.
 Fig. 1:
Fig. 1: Overall study population. All patients registered in the Japanese national survey 2011 with congenital FVII deficiency receiving rFVIIa during the collection period [from the approval date of the study drug (12 March 2010) to the end of study enrolment (30 June 2013)], regardless of baseline FVII activity, were eligible for inclusion. Bleeding episodes included intra-articular bleeding, intramuscular bleeding, epistaxis, menorrhagia and bleeding from other sites. Surgical episodes were classified as minor or major surgery and included orthopedic, oral, ocular, general, neurological and cardiac surgery. ICF, informed consent form. aOne patient was treated during both bleeding episodes and surgery.
A total of 401 bleeding episodes were recorded in eight patients who received rFVIIa at the time of bleeding. Among these eight patients, one patient, who experienced 53 bleeds, was excluded from the analyses of rFVIIa treatment duration, number of doses and total dose, because the dose and treatment duration could not be verified. These analyses therefore comprised 348 bleeding episodes in seven patients with a mean treatment duration of 2.8 days. A total of 16 surgical procedures (10 major and six minor) were conducted on 13 patients who received rFVIIa during surgery. One patient was included in both the bleeding and surgery categories.
A summary of patient disposition is presented in Table 1. There were seven male patients [two in the bleeding category and six in the surgery category (one patient was counted in both the bleeding and surgery categories)], 12 female patients (five in the bleeding and seven in the surgery category) and in one patient in the bleeding category whose sex was not recorded. Three patients underwent more than one surgical procedure, of whom one patient underwent the same intervention twice (tooth extraction). Among 20 patients, FVII activity was recorded for 18 patients at baseline (Table 1): with a FVII activity less than 10 IU/dl, at least 10–20 IU/dl and more than 20 IU/dl in nine, four and five patients, respectively.
Table 1 - Patient disposition Age Sex Body weight (kg) Baseline FVII (IU/dl) Length of time in study (months) Total number of bleeds during time in study Total number of surgeries during time in study Factor Vll activity: <10 IU/dl 11 NR 39.7 0.6 8 5 0 48 Female 48.0 1.5 49 75 0 35a Female 52.0 1.9 50 53 0 15 Female 57.3 <3.0 21 23 0 58 Female 55.0 ≤3.0 <1 0 1 59 Female 56.0 4.1 <1 1 0 78 Male 41.0 5.9 <1 0 2 55 Male 59.0 6.0 <1 0 1 24 Male 50.0 8.0 <1 0 2 Factor Vll activity: ≥10–20 IU/dl 40 Female 47.0 11.0 44 213 0 12 Male 49.0 12.0 47 15 0 52 Female 62.0 14.2 <1 0 1 32 Male 76.6 17.0 <1 0 1 Factor Vll activity: >20–50 IU/dl 42 Female 47.0 28.0 <1 0 1 69 Female 46.0 29.0 <1 0 1 80 Female 35.0 30.0 <1 0 1 25 Female 50.8 33.0 <1 0 1 14 Female 48.0 35.0 <1 0 2 Factor Vll activity: NR 51b Male 50.0 NR 35 16 1 74 Male 72.0 NR <1 0 1NR, not recorded.
aPatient was excluded from the analysis of rFVIIa treatment duration, number of doses and total dose because the dose and treatment duration could not be verified.
bOne patient was treated during both bleeding episodes and surgery.
Bleeding and surgical events by baseline FVII activity are summarized in Table 2. Among 348 bleeding episodes in seven patients, 48.9% (170/348) were intra-articular bleeding events, of which 92.9% (158/170) were in patients with a baseline factor VII activity 20 IU/dl or less; 17.8% (62/348) represented menorrhagia (occurring in three women of whom two were of reproductive age) [17], all of which were in patients with a baseline factor VII activity 20 IU/dl or less; 4.6% (16/348) were intra-muscular bleeding events, all of which were in patients with a baseline factor VII activity 20 IU/dl or less; 3.4% (12/348) represented epistaxis events, of which 75.0% (9/12) were in patients with a baseline factor VII activity 20 IU/dl or less; 25.3% (88/348) were bleeding events categorized as ‘other’, which included events involving the ovaries, abdomen, oral cavity and unknown sites, all of which were in patients with a baseline factor VII activity of 20 IU/dl or less. In the bleeding category, 16 of 348 (4.6%) events occurred in a single patient, for whom baseline FVII activity was not recorded. The majority of these [75% (12/16)] were intra-articular events.
Table 2 - Events by baseline FVII activity Factor Vll activity (IU/dl) <10 ≥10–20 >20–50 NR Bleeding episode (N = 348), n (%) Total 104 (29.9) 228 (65.5) 0 (0.0) 16 (4.6) Intra-articular 66 (19.0) 92 (26.4) 0 (0.0) 12 (3.4) Intra-muscular 4 (1.1) 12 (3.4) 0 (0.0) – Epistaxis 5 (1.4) 4 (1.1) 0 (0.0) 3 (0.9) Menorrhagiaa 21 (6.0) 41 (11.8) 0 (0.0) – Other 8 (2.3) 79 (22.7) 0 (0.0) 1 (0.3) Type of surgery (N = 16), n (%) Total 6 (37.5) 2 (12.5) 6 (37.5) 2 (12.5) Orthopedic 0 (0.0) 0 (0.0) 1 (6.25) 2 (12.5) Oral/dental 3 (18.75) 0 (0.0) 3 (18.75) 0 (0.0) General 3 (18.75) 2 (12.5) 2 (12.5) 0 (0.0)One patient was treated during both bleeding episodes and surgery.– denotes a value which was not available.NR, not reported.
aOnly assessed for women. Occurring in three out of four female patients experiencing bleeding events.
Among 16 surgical procedures in 13 patients, 18.8% (3/16) were orthopedic procedures, 37.5% (6/16) were oral/dental procedures and 43.8% (7/16) were general surgical procedures (Table 2). In 50.0% (8/16) of these surgical procedures, patients had a baseline factor VII activity of 20 IU/dl or less. In the orthopedic surgical category, a single procedure was conducted on two different patients, for whom FVII activity was not recorded.
rFVIIa treatment rFVIIa treatment for bleeding episodes in patients with congenital FVII deficiencyTable 3 shows a summary of rFVIIa treatment for bleeding episodes. The total median [interquartile range (IQR)] dose of rFVIIa in these patients was 41.7 (21.3–73.5) μg/kg per bleeding episode. The most common bleeds treated were intra-articular. Among 158 bleeds in three patients in whom the FVII activity was recorded, this category had the shortest duration of treatment with a median (IQR) of 2.0 (1.0–3.0) days (mean 2.5 days), and the lowest total dose with a median (IQR) of 41.7 (21.3–62.5) μg/kg (mean 46.3 μg/kg).
Table 3 - Dosing regimen – rFVIIa treatment for bleeding episodes One time dose (μg/kg) Number of doses Treatment duration (days) Total dose (μg/kg) Bleeding category Number of patients Number of bleeding episodes (%) Mean Median IQR Mean Median IQR Mean Median IQR Mean Median IQR Total 7 348 (100) – – – 3.0 2.0 1.0–3.0 2.8 2.0 1.0–4.0 61.7 41.7 21.3–73.5 Intra-articular 3 158 (45.4) 20.6 21.3 20.8–21.3 2.2 2.0 1.0–3.0 2.5 2.0 1.0–3.0 46.3 41.7 21.3–62.5 Intra-muscular 3 16 (4.6) 22.2 21.3 21.1–24.5 2.1 2.0 1.0–3.0 2.9 2.5 1.0–5.0 46.6 42.6 22.9–63.2 Epistaxis 2 9 (2.6) 29.7 25.2 24.5–30.2 3.9 2.0 2.0–3.0 3.9 2.0 2.0–5.0 112.5 60.5 50.4–100.8 Menorrhagia 3 62 (17.8) 19.3 21.3 17.5–21.3 6.2 7.0 3.0–8.0 4.1 4.0 3.0–5.0 123.8 127.7 52.4–170.2 Other 6 103 (29.6) – – – – – –Table does not include data from a single patient in whom the FVII activity was not reported.One time dose is defined as a single dose given on one occasion.– denotes a value which was not available.IQR, interquartile range.
Menorrhagia accounted for the second most common bleeding type. Among 62 bleeds in three of the four female patients in the bleeding category, menorrhagia had the longest treatment duration with a median (IQR) of 4.0 (3.0–5.0) days (mean 4.1 days), and the highest total dose with a median (IQR) of 127.7 (52.4–170.2) μg/kg (mean 123.8 μg/kg) (Table 3). Epistaxis account for the lowest number of bleeds treated (nine bleeds in two patients) with a median (IQR) for treatment duration, number of doses and total dose of 2.0 (2.0–5.0) days (mean 3.9 days), 2.0 (2.0–3.0) doses (mean 3.9 doses) and 60.5 (50.4–100.8) μg/kg (mean 112.5 μg/kg), respectively (Table 3).
For 85.9% (299/348) of bleeding events, rFVIIa treatment was administered at or near the labelled dose of 15–30 μg/kg (data not shown). The median (IQR) number of doses required to achieve hemostasis for intra-articular bleeds, menorrhagia and overall was 2.0 (1.0–3.0), 7.0 (3.0–8.0) and 2.0 (1.0–3.0), respectively. In patients for whom treatment intervals were recorded, interval ranges varied considerably (data not shown).
rFVIIa treatment at the time of surgery in patients with congenital FVII deficiencyTable 4 shows a summary of the rFVIIa treatment at the time of surgery in patients with congenital FVII deficiency. The total median (IQR) dose of rFVIIa in all surgical patients was 36.9 (21.5–57.0) μg/kg per procedure. Among patients whose baseline FVII activity level and exposure data were recorded, there were six minor surgeries in four patients and eight major surgeries in eight patients. Two patients without a recorded baseline FVII activity underwent one major surgery each.
Table 4 - Dosing regimen – rFVIIa treatment at the time of surgery One-time dose (μg/kg) Number of doses Treatment duration (days) Total dose (μg/kg) Baseline FVII (IU/dl) Number of patients Number of surgeries Type of surgery Mean Median IQR Mean Median IQR Mean Median IQR Mean Median IQR Totala 13 16 – – – 4.7 2.0 1.0–2.0 2.6 1.0 1.0–2.0 121.3 36.9 21.5–57.0 Major surgery 10 10 42.0 20.5 17.6–26.5 3.8 2.0 1.0–3.5 2.3 2.0 1.0–3.0 111.9 41.3 24.9–178.1 <10 3 3 Rectum: rectal amputation
留言 (0)