
記住我


Female genital schistosomiasis (FGS) was first described in 1899 in Egypt but was largely only reported as incidental findings till the 1990s.1Female genital schistosomiasis has been found to be almost as common as urinary schistosomiasis within the female populations of Schistosoma haematobium-endemic areas.2–4 Furthermore, in some schistosomiasis-endemic communities, it may be the most common gynecological morbidity.4 Despite its prevalence, World Health Organization (WHO) data for 2017 show that only 46.3% of the 220.8 million people requiring treatment for schistosomiasis have been reached.5
Female genital schistosomiasis is a poverty-related neglected tropical disease caused by the S. haematobium parasite, which is transmitted by contact with infested fresh water.4 It is known to be endemic in areas of sub-Saharan Africa where lakes, rivers, and dams are used for domestic and recreational purposes.6Female genital schistosomiasis may cause bloodstained and foul-smelling discharge, dyspareunia, contact bleeding, burning sensations in the genitals, decreased fertility, spontaneous abortions, and increased susceptibility to HIV and human papillomavirus (HPV), as well as possibly cervical cancer.4,7,8 The S. haematobium parasites inhabit blood vessels surrounding the female genital tract and the urinary bladder.4 There they lay eggs, which are then propagated toward the adjacent organs, creating the aforementioned morbidities. The morbidity seen in FGS is attributed to chronic inflammation in the cervical and vaginal mucosa, and lesions involve both dead and viable parasite eggs.9
Female genital schistosomiasis is a differential diagnosis to some sexually transmitted infections (STIs), causing vaginal discharge and ulcers.10 Furthermore, it has also been hypothesized that FGS may make women susceptible to HPV infection and other STIs.11,12
In this study, we aim to explore the relationship between lower genital tract FGS and reproductive tract infections in an adolescent female population and establish the relative prevalences of these infections in a rural S. haematobium-endemic area.
METHODSThe study was approved by the Biomedical Research Ethics Administration (BREC), University of KwaZulu-Natal, South Africa (Ref BF09/07) and the Department of Health, Pietermaritzburg, South Africa (Ref HRKM010–08). Ethical clearance was also granted from the regional committee of Medical and Health Research Ethics (REC), South Eastern Norway (Ref 469-07066a1.2007.535) and renewed in 2011. Written informed consent was obtained from all subjects, a legal surrogate, and the parents or legal guardians for minor subjects. To maintain confidentiality, legal guardians and parents were not given information acquired from the young women during the consent procedure or investigations. Permissions were also granted by the Departments of Health and Education, KwaZulu-Natal. The STI and FGS testing and results were described in the consent form. At the end of the questionnaire, the participants were asked if, and how, they wished to be contacted, should tests show disease for which they needed treatment or referral. All participants with positive laboratory results were approached and were either given treatment by a registered nurse (tablets) or offered transport to a local clinic for management.
Study DesignIt has been shown that schistosomiasis is endemic in the lower altitudes KwaZulu-Natal Province of South Africa.13 Therefore, randomly selected rural secondary schools below the altitude of 400 m and with a urinary schistosomiasis prevalence greater than 20% were invited to take part in the study. For practical purposes and due to financial constraints, we only invited schools with 300 or more pupils. To reach as many positive cases as possible, schools were excluded if they had been classified as urban (and therefore less likely to be using infested water sources) by the Department of Education. From 2011 to 2013, nested in a prospective study on the prevention of FGS, the study included sexually active, school-attending women aged 16–22 years, usually in grades 10–12, who consented to a gynecological examination and were willing to be tested for STIs.14
CLINICAL EXAMINATION AND QUESTIONNAIREParticipants underwent a gynecological examination performed by female doctors trained by the same expert in recognizing FGS on the cervix and vaginal walls. Clinical manifestations of FGS were documented by photocolposcopy (Olympus OCS 500 [Olympus, Tokyo, Japan] colposcope with a mounted Olympus E 420 [Olympus, Tokyo, Japan] 10-MP single lens reflex device, or a Leisegang colposcope [Leisegang, Berlin, Germany] with a Canon EOS 40D [Canon, Tokyo, Japan] 10-MP single lens reflex).15 In average biweekly, an FGS expert would investigate patients together with the clinician to ascertain uniform diagnosis; furthermore, images were reviewed as quality control by 1 expert (E.F.K.). Grainy sandy patches were defined as lesions with grains measuring approximately 0.05 × 0.2 mm and shaped like minuscule rice grains, deeply or superficially situated within the mucosa.10 Homogenous yellow patches were defined as yellow areas with no distinct grains. The chronological aspects of FGS have not yet been determined, although 2 recent articles suggest that homogenous yellow patches seem to represent old lesions, whereas grainy sandy patches and rubbery papules represent more recent deposition of S. haematobium ova in the tissues.16,17 Rubbery papules were defined as beige to yellow papules with a firm (rubbery) protrusion into the intravaginal lumen. All the FGS lesions may be accompanied by characteristic abnormal blood vessels seen as pathological convoluted, uneven calibered, reticular, circular, branched, or corkscrew patterns.18 Patients were only investigated by 1 clinician.
Trained female staff interviewed study participants in isiZulu (the local language) using a questionnaire that covered demographic information, current reproductive health complaints, obstetric history, sexual behavior, water contact, and their approaches to the health services for genital symptoms. Those who said they had not commenced sexual activity were not invited for clinical examination.
LABORATORY TESTINGFor the diagnosis of urinary schistosomiasis, a urine sample was collected between 10 a.m. and 2 p.m., which is the peak daily egg excretion time.19 Urine was centrifuged, the sediment deposited on 2 slides, and read by 2 independent laboratory technicians.
Urine was considered schistosomiasis-positive if at least 1 S. haematobium ovum was seen under microscopy. Samples of cervicovaginal lavage were collected by spraying 10 mL of saline on the cervical surface and withdrawing it back into the syringe. Herpes simplex virus type 2 (HSV-2) antibodies were detected in serum using ELISA Ridascreen HSV-2 IgG (Davies Diagnostics, Randburg, South Africa) and in ELISA HerpeSelect, IgG assay (Focus Diagnostics, Germany). Herpes simplex (Cape Town, South Africa) virus type 2 polymerase chain reaction (PCR) test was only done in a subsample of participants due to financial and practical constraints. Likewise, HPV was done in a subsample and detected by GP5+/6+ HPV PCR test, followed by an enzyme immunoassay method using a cocktail mix of high-risk HPV (hr-HPV) probes (Whitehead Scientific, Cape Town, South Africa).20 For genotyping, individual probes were used. Individual probes for the most common hr-HPV genotypes in cervical cancer were selected: hr-HPV types 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73. and 82. Fourteen of these were identified individually from specimens using EIA test, and HPV 26 and 53 as well as HPV 73 and 82 were tested in combination. The cut-off value for hr-HPV genotype was calculated following the formula of the mean optical density plus 3 times the standard deviation (SD) of all samples in the plate. After exclusion of outliers, the final mean + 3SD was recorded and used as the cut-off. This genotyping assay precludes detection of previously unknown genotypes. Cervical swabs were analyzed using ProbeTec CT/GC and AC strand displacement PCR assay for Chlamydia trachomatis and Neisseria gonorrhea (Becton Dickinson Microbiology Systems, Franklin Lakes, NJ).21 In-house validated PCR assays were done using the primer set SarR and SarF specific for Trichomonas vaginalis and HSV in the Laboratory of Infection, Prevention, and Control at the University of KwaZulu-Natal, Durban, South Africa.22 Syphilis was detected in thawed serum samples using Macro Vue test 110/112 (BD, Becton Dickinson Microbiology Systems) for a rapid plasma reagin test and Immutrep for Treponema pallidum hemagglutination assay (Omega Diagnostics Group PLC, Alva, United Kingdom). The Nugent scoring criteria was used for the diagnosis of bacterial vaginosis. Candidiasis was diagnosed using the Gram staining technique under light microscopy and severity scored (1–5) in accordance to the number of spores seen.23
STATISTICAL ANALYSISTo be able to detect a 10% difference in an STI's prevalence between the FGS-positive and negative groups with a confidence level of 0.05 and power of 0.8, sample size calculations indicated that we would need 200 FGS-positive patients and 600 FGS-negative patients. Chi-square or Fisher exact tests were used to evaluate the hypothesis. Age was included in the multivariable logistic regression regardless of significance level. Other variables were included if the association between the sandy patches and the STIs had a p value lower than 0.2. Comparison of mean age between the FGS-positive and negative groups was done using the Student t test. An α level of 0.05 was used for all statistical tests. Analyses were performed using IBM SPSS Statistics Version 25 (IBM Corp, Armonk, NY).
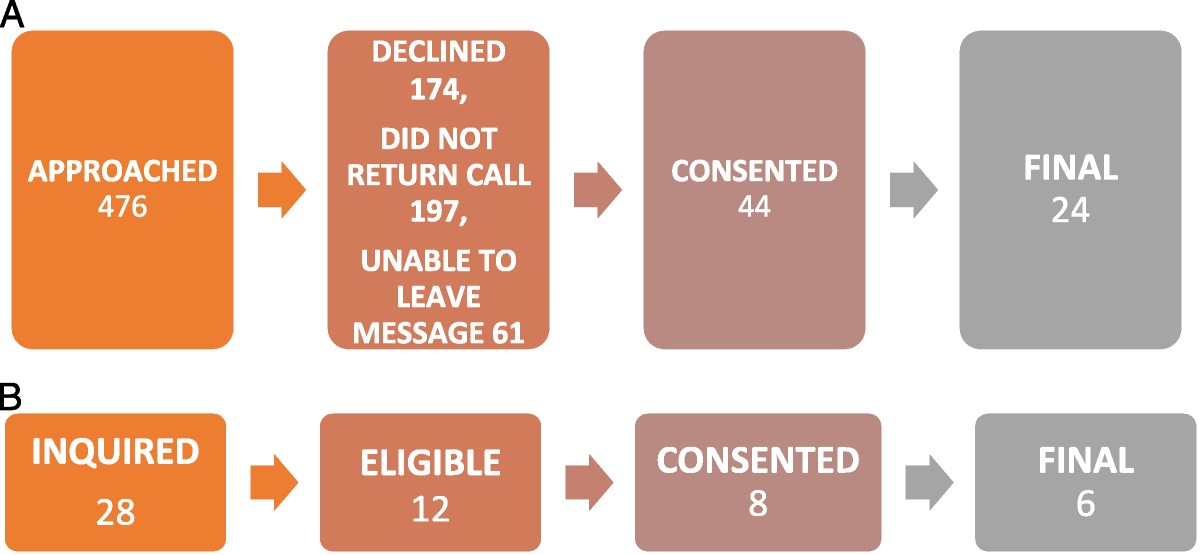
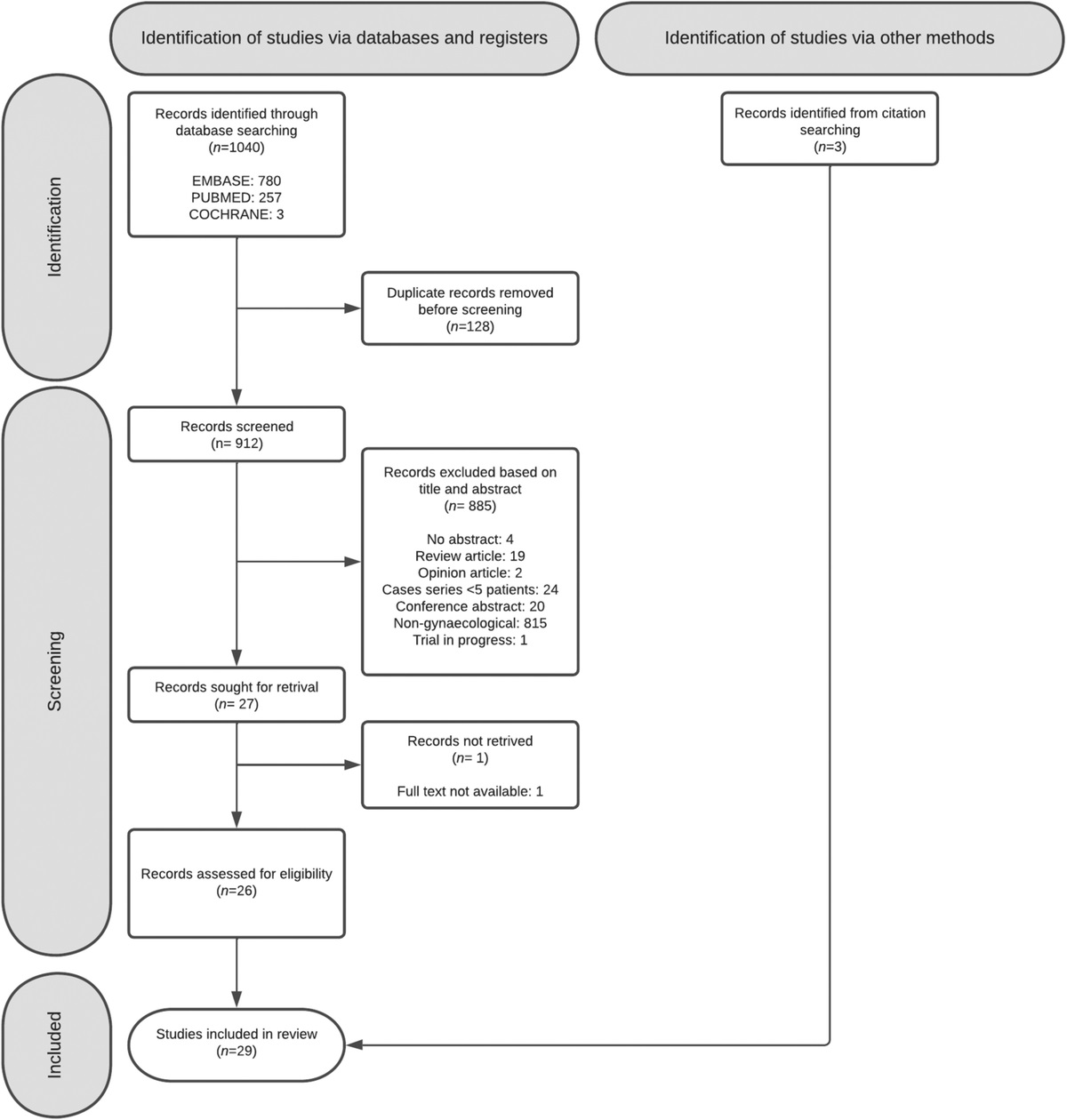
RESULTSA total of 933 participants from 32 schools were willing to be tested for STIs (Figure 1). One or more STIs were found in 819/930 (88.1%) of the participants and FGS was found in 210/933 (22.5%). More than half of these rural secondary school-going young women had been pregnant (Table 1). The mean age was 18.7 years (SD, 1.6), indicating that approximately half of them had missed a year or more of schooling. Mean number of lifetime partners was 1.9 (SD, 0.5), age at sexual debut 16.6 (SD, 1.5), and mean number of partners the last month was 0.7 (SD, 0.5). Only 25% (227/926) had used condoms the last week. Most women had been exposed to fresh water at high risk of schistosomiasis contamination at some point in their lives (881/930 [94.7%]). Urinary S. haematobium ova excretion was found in 256/840 (30.5%). In the positive cases, the geometric mean intensity urinary S. haematobium was 57.9 eggs per 10 mL. There was no difference in mean age of those who had FGS compared with those who did not. Evidence of a previous HSV infection (serology) was found in 286/900 (31.8%) of the participants. However, only a handful of pupils had current blisters. The prevalence of current Chlamydia, HPV, trichomoniasis, and gonorrhea were 218/827 (26.4%), 149/551 (27.0%), 163/839 (19.4%), and 102/827 (12.3%), respectively.
 FIGURE 1:
FIGURE 1: Flow chart of participants in the study. aFemale pupils in schools with more than 20% urinary schistosomiasis, grades 10–12, and sexually active. bDid not undergo gynecological examination (n = 416), did not submit a questionnaire (n = 42), did not submit urine (n = 295), and 301 had overlapping reasons for being excluded.
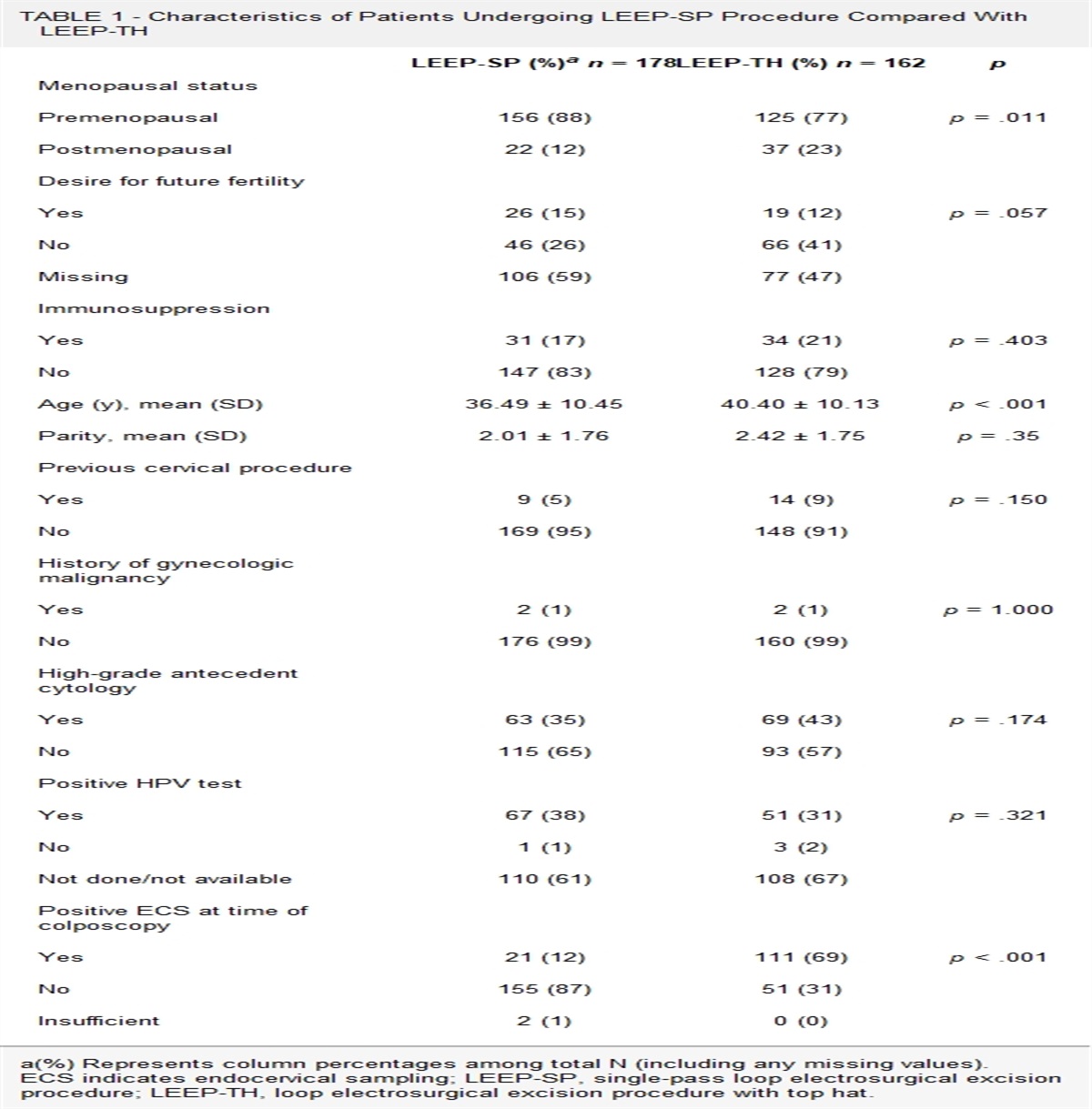
TABLE 1 - The Main Characteristics of Participants with FGS Variable No. participantsSome points were not answered in the questionnaire.
aSchistosoma haematobium ova found in a single urine sample, some did not submit urine samples.
bRiver, dam, pond, or stream.
cLocal popular religion.
dUniversity level.
e8–12 years of school.
f1–7 years of school.
FGS indicates female genital schistosomiasis.
Human papillomavirus testing was done in a subsample of 551 patients (55%) and was positively associated with FGS. When HPV was analyzed against the subtypes of sandy patches seen in Figure 2, it was positively associated with superficial grainy sandy patches (age-adjusted odds ratio [OR] = 1.85; 95% CI = 1.05–3.245; p = .03) and homogenous yellow patches (adjusted OR [AOR] = 2.43; 95% CI = 1.49–4.0; p < .001). Human papillomavirus was however, not associated with deep grainy patches (age-adjusted OR = 0.70; 95% CI = 0.30–1.7; p = .42), but the sample size was small (51 cases).
 FIGURE 2:
FIGURE 2: Lesions of FGS in a young South African woman. Solid arrows: Grainy sandy patch embedded in homogenous yellow patch (rectangle). Hatched arrows: Abnormal blood vessels. Oval: Nabothian cyst.
There was significantly less C. trachomatis in the FGS-positive group than in the FGS-negative, after controlling for age, HSV serology, and trichomoniasis. Chlamydia was also negatively associated with superficial grainy sandy patches (age-adjusted OR = 0.44; 95% CI = 0.26–0.75; p = .002) and deep grainy patches (AOR = 0.30; 95% CI = 0.12–0.77; p = .01). Homogenous yellow patches showed the same tendency (AOR = 0.71; 95% CI = 0.42–1.19; p = .19). Similarly, the chlamydia prevalence tended to be lower in the urinary schistosomiasis-positive cases than in urinary schistosomiasis-negative, although this difference was not significant (AOR = 0.70; 95% CI = 0.45–1.02; p = .06). Half (109/218 [50.0%]) of the C. trachomatis cases were clustered in 8/32 (25.0%) schools, indicating possibly some super-spreader events. After stratification, taking out the chlamydia high-endemic schools, FGS remained negatively associated with Chlamydia, after adjusting for age, trichomoniasis, and HSV serology (AOR = 0.41; 95% CI = 0.22–0.79; p = .007), but not in the 8 schools, each of which had more than 35% Chlamydia. Of the study participants, 12.6% (110/876) had been treated for an STI previously. There was a significant association with having HSV (OR = 1.5; 95% CI = 1.2–1.9, p = .001) but no association was found with FGS (p = .97), Chlamydia (p = .33), dual infection with FGS and Chlamydia (0.45), or other STIs.
Trichomonas vaginalis was associated with the clinical finding of “homogenous yellow patches” (age-adjusted OR = 1.74; 95% CI = 1.10–2.75; p = .019). No other STIs were associated with grainy sandy patches (data not shown). Positive HSV serology and current trichomoniasis were higher in the FGS-positive group than in the FGS-negative but the differences were not significant. The mean bacterial vaginosis scores were the same in FGS-positive and negative populations. Only 29/901 (3.2%) cases were positive for T. pallidum, and there was no significant difference between the groups (p = .49).
As expected, FGS was positively associated with urinary schistosomiasis (OR = 2.32; 95% CI = 1.77–3.02; p < .001). Female genital schistosomiasis was found not only in 89/256 (34.8%) of those who were positive for urinary schistosomiasis but also in 110/584 (18.8%) of the participants where urinary schistosomiasis was not detected, showing that not all with urinary schistosomiasis have FGS and that urine analysis alone does not suffice for FGS detection. Among the 5 participants who denied any waterbody contact, none were diagnosed with urinary schistosomiasis, although sandy patches were found in 1 case. Urinary schistosomiasis was not associated with any of the other reproductive tract infections.
As further exploration, we included HPV in the multivariable analysis of Table 2. Human papillomavirus remained significantly associated with FGS (AOR = 1.71; 95% CI = 1.11–2.38; p = .016). There was less Chlamydia in the FGS-positive than in the FGS-negative, but the difference was not statistically significant (AOR = 0.67; 95% CI = 0.42–1.07; p = .096).
TABLE 2 - The Association Between STIs and FGS in Young Women FGS+ a FGS− OR (95% CI) b pc AOR d (95% CI) pe Mean age, y (SD) 18.7 (1.6) 18.7 (1.6) 0.97 HSV-2 serology f 36.9% (75/203) 30.4% (212/697) 1.39 (1.00–1.93) 0.079 1.36 (0.97–1.89) 0.077 T. vaginalis PCR g 24.2% (50/207) 18.1% (113/632) 1.44 (0.99–2.10) 0.055 1.44 (0.99–2.097) 0.056 C. trachomatish 19.6% (37/189) 28.4% (181/638) 0.62 (0.41–0.92) 0.017 0.61 (0.41–0.92) 0.018 HPV 34.9% (52/149) 23.9% (96/402) 1.71 (1.14–2.56) 0.010 NI i NI T. pallidumj 4.0% (8/201) 3.0% (21/700) 1.34 (0.56–3.07) 0.49 NI k NI HSV PCR l 4.7% (5/107) 4.9% (12/244) 0.95 (0.33–2.76) 0.92 NI k NI N. gonorrheah 13.8% (26/189) 11.9% (76/638) 1.18 (0.73–1.90) 0.50 NI NI BV m 61.7% (115/185) 62.2% (375/608) 1.01 (0.73–1.43) 0.91 NI NI Mean BV score (SD) 6.5 (2.8) 6.6 (2.5) Candida species n 7.5% (14/186) 9.0% (55/608) 0.97 (0.74–1.27) 0.80 NI NI Mean candidiasis score (SD 0.2 (0.6) 0.2 (0.6)Denominator varies because specimens were not available for all analyses.
aFGS determined by colposcopic inspection.
bOdds ratio (95% confidence interval).
cChi-square test.
dAdjusted for age.
eLogistic regression.
fHerpes simplex virus.
gIn-house PCR.
hStrand displacement assay.
iNot included (NI) in multivariable logistic regression analysis due to small sample size; however, explored in last paragraph of results.
jRapid plasma reagin and T. pallidum hemagglutination assays.
kNot included in multivariable analysis due to p > .2.
lOnly 351 analyzed (financial reasons).
mNugent criteria, score > 7.
nMicroscopy.
BV indicates bacterial vaginosis.
Comparing FGS-positive and negative, there was no difference in duration since the last sexual intercourse (p = .37), lifetime partners (p = .29), age at sexual debut (p = .34), number of partners the last month (p = .66), or condom use (p = .41).
DISCUSSIONFemale genital schistosomiasis was almost as common as Chlamydia, with both infections affecting more than one fifth of this young rural population. As published previously, the study shows that FGS seems to be a risk factor for HPV.24,25 Unexpectedly, the FGS-positive had less concurrent chlamydia infection compared with those without FGS. This has not been reported previously.
Female genital schistosomiasis manifestations cause a chronic state of intravaginal inflammation that could aid the acquisition of STIs.9,26 This inflammation may cause symptoms and may make women go to local health institutions for treatment. Diagnosis in rural, low-resource areas is almost invariably based on patient history and point-of-care inspection, very rarely confirmed by laboratory analyses.27 The S. haematobium transmission and likewise FGS are likely to have occurred in early childhood and therefore before STIs,8 indicating that there are intravaginal damages already from a young age. If the vaginal discharge has been constant since childhood, it could be argued that it would be interpreted as normal by the patients.8,28 However, 2 studies found that adults with FGS report having abnormal discharge.29,30 This may indicate that they experience changes in discharge, possibly because the bleeding and ulcerous surfaces of FGS are super-infected by other agents such as bacteria, as has been found for S. haematobium of the bladder in mouse models.31 Refractory symptoms must, however, be interpreted with caution, reinfection with STIs is common, symptoms may persist for a while after adequate treatment, or persisting symptoms may be caused by FGS.
There was an overall trend of higher prevalence of STIs in the FGS-positive participants. However, Chlamydia was the exception. Chlamydia is often asymptomatic.32 Young women with FGS and (asymptomatic) Chlamydia may have sought STI treatment (provided for free by the local clinics) more often than those without FGS. Alternatively, dual infection (with FGS and Chlamydia) might cause intensified symptoms, leading to health-seeking behavior and antibiotic treatment for vaginal discharge.27 This could not be confirmed in our study.
Our study's conclusions have the following limitations. To confirm the small differences between the groups, we would have had to have a larger sample size. Almost all participants in this population had local freshwater contact at some point in their lives, and they may have had FGS previously, diluting the findings of this study. The WHO currently recommends visual pelvic examination for diagnosis of FGS,10 whereas in areas where laboratory analyses are not available, WHO recommends only STI treatment based on patient information or genital examination for vaginal discharge, not mentioning FGS.33 Urine sampling cannot be used for FGS diagnosis.2 Due to logistic and resource constraints, only 1 urine sample was collected per participant. Multiple samples would likely have yielded a higher prevalence of urinary schistosomiasis due to day-to-day variations in egg excretion. This was a limitation in this study. Furthermore, FGS diagnosis is dependent on the colposcopic inspection of all intravaginal surfaces, including the fornices and posterior and anterior vaginal walls.10 Therefore, we may also have missed some FGS-positive cases, and we cannot preclude that STIs were sometimes misdiagnosed as FGS. This might have obscured differences between the FGS-positive and FGS-negative groups.3
The symptoms of FGS overlap with symptoms of the various STIs causing discharge, a burning sensation in the genitals, and ulcers.8 However, in countries where FGS is endemic, laboratory testing for STIs and examinations are often not performed. In rural Africa, abnormal discharge and genital ulcers are currently managed syndromically as STIs, without laboratory testing.34 The current syndromic management for vaginal discharge entails treatment for Chlamydia, gonorrhea, and trichomoniasis, but not for FGS.34 Therefore, patients may be inadvertently overtreated for STIs and undertreated/not treated for FGS.
Examinations for FGS rely on clinical expertise and are not yet performed in routine health care.10,26 The risk of misdiagnosis of FGS as an STI warrants rewriting the syndromic management protocols and algorithms for genital tract disease, especially in endemic areas. Furthermore, symptoms of STIs and FGS are also found in children with S. haematobium.8 Yet, health professionals are not taught about FGS, and FGS is not on the list of differential diagnoses for genital ulcers and discharge. Therefore, changes in the health professionals' curricula and the protocols for management of reproductive tract diseases in females are necessary.35,36 Antischistosomal treatment should be added to the treatment protocols and FGS should be considered among the differential diagnoses.
Preventive treatment for S. haematobium with praziquantel is not expensive and readily available and may provide a reduction in FGS occurrence. Further research is needed to understand the physiological mechanisms behind the sandy patches and to explore if praziquantel treatment can reduce the incidence of HPV and subsequent cervical cancers.
REFERENCES 1. Madden FC. A case of Bilharzia of the vagina. Lancet 1899;1:1710–6. 2. Swai B, Poggensee G, Mtweve S, et al. Female genital schistosomiasis as an evidence of a neglected cause for reproductive ill-health: a retrospective histopathological study from Tanzania. BMC Infect Dis 2006;23:134. 3. Poggensee G, Kiwelu I, Weger V, et al. Female genital schistosomiasis of the lower genital tract: prevalence and disease-associated morbidity in Northern Tanzania. J Infect Dis 2000;181:1210–3. 4. Kjetland EF, Leutscher PDC, Ndhlovu PD. A review of female genital schistosomiasis. Trends Parasitol 2012;28:58–65. 5. World Health Organization. Schistosomiasis fact sheet. 2019. Available at: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis. Accessed July 19, 2019. 6. Zhang Y, Koukounari A, Kabatereine N, et al. Parasitological impact of 2-year preventive chemotherapy on schistosomiasis and soil-transmitted helminthiasis in Uganda. BMC Med 2007;5:27. 7. Feldmeier H, Poggensee G, Krantz I, et al. Female genital schistosomiasis. New challenges from a gender perspective. Trop Geogr Med 1995;47:S2–15. 8. IEA Hegertun, Sulheim Gundersen KM, Kleppa E, et al. S. haematobium as a common cause of genital morbidity in girls: a cross-sectional study of children in South Africa. PLoS Negl Trop Dis 2013;7:e2104. 9. Jourdan PM, Roald B, Poggensee G, et al. Increased vascularity in cervicovaginal mucosa with Schistosoma haematobium infection. PLoS Negl Trop Dis 2011;5:e1170. 10. Mbabazi PS, Vwalika B, Randrianasolo BS, et al. World Health Organization Female Genital Schistosomiasis. A Pocket Atlas for Clinical Health-Care Professionals. Geneva: WHO; 2015. 11. Leutscher PDC, Ramarokoto C-EE, Hoffmann S, et al. Coexistence of urogenital schistosomiasis and sexually transmitted infection in women and men living in an area where Schistosoma haematobium is endemic. Clin Infect Dis 2008;47:775–82. 12. Yirenya-Tawiah D, Amoah C, Apea-Kubi KA, et al. A survey of female genital schistosomiasis of the lower reproductive tract in the Volta Basin of Ghana. Ghana Med J 2011;45:16–21. 13. Appleton CC, Maurihungirire M, Gouws E. The distribution of helminth infections along the coastal plain of Kwazulu-Natal Province, South Africa. Ann Trop Med Parasitol 1999;93:859–68. 14. Galappaththi-Arachchige HN, Hegertun IEA, Holmen S, et al. Association of urogenital symptoms with history of water contact in young women in areas endemic for S. Haematobium. A cross-sectional study in rural South Africa. Int J Environ Res Public Health 2016;13:1135. 15. Holmen SD, Kleppa E, Lillebø K, et al. The first step toward diagnosing female genital schistosomiasis by computer image analysis. Am J Trop Med Hyg 2015;93:80–6. 16. Nemungadi TG, Furumele TE, Gugerty MK, et al. Establishing and integrating a female genital schistosomiasis control programme into the existing health care system. Trop Med Infect Dis 2022;7:382. 17. Sang HC, Mwinzi PNM, Odiere MR, et al. Absence of lower genital tract lesions among women of reproductive age infected with Schistosoma mansoni: a cross-sectional study using a colposcope in Western Kenya. PLoS Negl Trop Dis 2022;16:e0010473. 18. Holmen S, Galappaththi-Arachchige HN, Kleppa E, et al. Characteristics of blood vessels in female genital schistosomiasis: paving the way for objective diagnostics at the point of care. PLoS Negl Trop Dis 2016;10:e0004628. 19. Doehring E, Vester U, Ehrich JH, et al. Circadian variation of ova excretion, proteinuria, hematuria, and leukocyturia in urinary schistosomiasis. Kidney Int 1985;27:667–71. 20. Mbatha JN, Taylor M, Kleppa E, et al. High-risk human papillomavirus types in HIV-infected and HIV-uninfected young women in KwaZulu-Natal, South Africa: implications for vaccination. Infect Dis (Lond) 2017;49:601–8. 21. Kleppa E, Holmen SD, Lillebø K, et al. Cervical ectopy: associations with sexually transmitted infections and HIV. A cross-sectional study of high school students in rural South Africa. Sex Transm Infect 2015;91:124–9. 22. Zimba TF, Apalata T, Sturm WA, et al. Aetiology of sexually transmitted infections in Maputo, Mozambique. J Infect Dev Ctries 2011;5:41–7. 23. Dellar RC, Dlamini S, Karim QA. Adolescent girls and young women: key populations for HIV epidemic control. J Int AIDS Soc 2015;18:19408. 24. Kjetland EF, Ndhlovu PD, Mduluza T, et al. The effects of genital Schistosoma haematobium on human papillomavirus and the development of cervical neoplasia after five years in a Zimbabwean population. Eur J Gynaecol Oncol 2010;31:169–73. 25. Pillay P. Female genital schistosomiasis as a risk factor for squamous cell atypia in an epidemiological longitudinal cohort of young women in KwaZulu-Natal. 2016. Available at: https://researchspace.ukzn.ac.za/handle/10413/16543. Accessed May 31, 2023. 26. UNAIDS, World Health Organization. No More Neglect. Female Genital Schistosomiasis and HIV. Integrating Reproductive Health Interventions to Improve Women's Lives. Geneva, Switzerland: World Health Organization; 2019. 27. Farley TA, Cohen DA, Elkins W. Asymptomatic sexually transmitted diseases: the case for screening. Prev Med 2003;36:502–9. 28. Kjetland EF, Ndhlovu PD, Kurewa EN, et al. Prevention of gynecologic contact bleeding and genital sandy patches by childhood anti-schistosomal treatment. Am J Trop Med Hyg 2008;79:79–83. 29. Kjetland EF, Ndhlovu PD, Mduluza T, et al. Simple clinical manifestations of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med Hyg 2005;72:311–9. 30. Leutscher P, Ravaoalimalala VE, Raharisolo C, et al. Clinical findings in female genital schistosomiasis in Madagascar. Trop Med Int Health 1998;3:327–32. 31
留言 (0)