
Remember me

Anxiety disorders are among the most frequently occurring psychiatric disorders in the United States, with an estimated 7.8% lifetime prevalence of generalized anxiety disorder in adults, and a cumulative 20% to 30% prevalence of all anxiety disorders among older adolescents/young adults.1–3 These disorders can cause significant functional impairments, reductions in quality of life, patient and family burden, and increased utilization of healthcare services.3 Like many neuropsychiatric disorders, anxiety is associated with complex pathophysiology, including aberrant neural inhibition—which, in the central nervous system, is mediated in part through the predominant inhibitory neurotransmitter γ-aminobutyric acid (GABA) and its receptors.4 Indeed, GABA has long been a central therapeutic target for the treatment of neuropsychiatric symptoms.4 The benzodiazepines are a class of allosteric GABA receptor modulators commonly used to treat a range of disorders, including anxiety and sleep disorders.4
Lorazepam, a member of the benzodiazepine class, has long been used for the short-term treatment of anxiety, first receiving US Food and Drug Administration (FDA) approval in 1977 as an immediate-release (IR) formulation (Ativan).5 Historically, lorazepam has been clinically used as an antianxiety agent for acute or chronic anxiety, as a premedication before surgical procedures, as a sedative in intensive care settings, or to treat agitation in severe panic attacks.6,7 Although lorazepam has been used in clinical practice for over 4 decades for a variety of indications, the overall prescription of benzodiazepines and lorazepam has declined over the past decade.8–10 Current indications include the short-term treatment of excessive anxiety associated with anxiety neurosis and adjunct relief for severe anxiety related to upcoming surgical intervention.5 Oral, oral concentrate, sublingual, intravenous, and intramuscular administration modalities have subsequently become available to treat both the original indications and additional indications, including as an anticonvulsant aid.6,7,11
Given the long history of lorazepam use, its pharmacokinetic (PK) and metabolic profile have been previously characterized.6,7,11,12 When given orally, lorazepam is quickly absorbed in the gastrointestinal tract, with previous reports noting maximum plasma concentrations achieved approximately 2 to 3 hours after dosing and bioavailability ≥90%.6,7,11 The half-life documented in previous reports is between 10 and 20 hours, with pharmacological effects typically dissipating after 6 to 8 hours.7 Lorazepam is metabolized in the liver, where it undergoes direct conjugation to glucuronic acid via glucuronyl transferase to form a pharmacologically inactive metabolite that is primarily excreted through the kidneys.6,7 Of note, IR lorazepam has demonstrated a safe hepatic profile, with acute or clinically apparent liver injury or serum alanine aminotransferase elevations being quite rare.13
Traditionally, IR lorazepam is prescribed at doses usually ranging from 2 to 6 mg/day given in tablets 2 to 3 times daily (BID/TID), but the daily dose can be from 1 to 10 mg/day for some patients.12,14 Although this dosing regimen can be effective for the treatment of short-term anxiety, the IR lorazepam formulation and IR benzodiazepines in general have limitations. First, serum concentrations of IR benzodiazepines rise quickly, which can lead to off-target effects such as memory loss and sedation.15,16 Detrimental adverse effects such as impaired recall have been reported with IR lorazepam in a dose-related manner.5 Moreover, just as plasma concentrations of IR benzodiazepines rise quickly, they can also fall quickly to subtherapeutic levels, leading to a breakthrough effect in which anxiety symptoms reemerge before the next scheduled dose.16 Lastly, dosing multiple times throughout the day represents a high pill burden, which has been shown to reduce treatment adherence, thus worsening outcomes.15 As such, a formulation providing fewer fluctuations between peak and trough lorazepam serum concentrations would provide relief throughout the day while reducing rebound/breakthrough anxiety and risk for adverse events (AEs), and—if given with fewer pills—lessen the pill burden on patients.15
With these considerations in mind, extended-release (ER) lorazepam (Loreev XR) was approved by the FDA in August 202117 for the treatment of anxiety disorders in adults who are already receiving stable, evenly divided, TID dosing of IR lorazepam tablets.18Extended-release lorazepam is prescribed as a once-daily capsule (doses of 1, 1.5, 2, and 3 mg; with the 3-mg dose equivalent to the previous total TID IR dosage) that may be swallowed whole or opened and sprinkled onto soft food.18Extended-release lorazepam may therefore provide flexible dosing administration options to patients already benefiting from IR lorazepam, with fewer fluctuations in drug levels throughout the day. Here we report PK data analyzed across a series of phase 1 studies comparing the bioequivalence of 3 mg once-daily ER lorazepam with IR lorazepam given TID, and the impact of food or sprinkling administration on PK characteristics of the ER formulation in healthy adults.
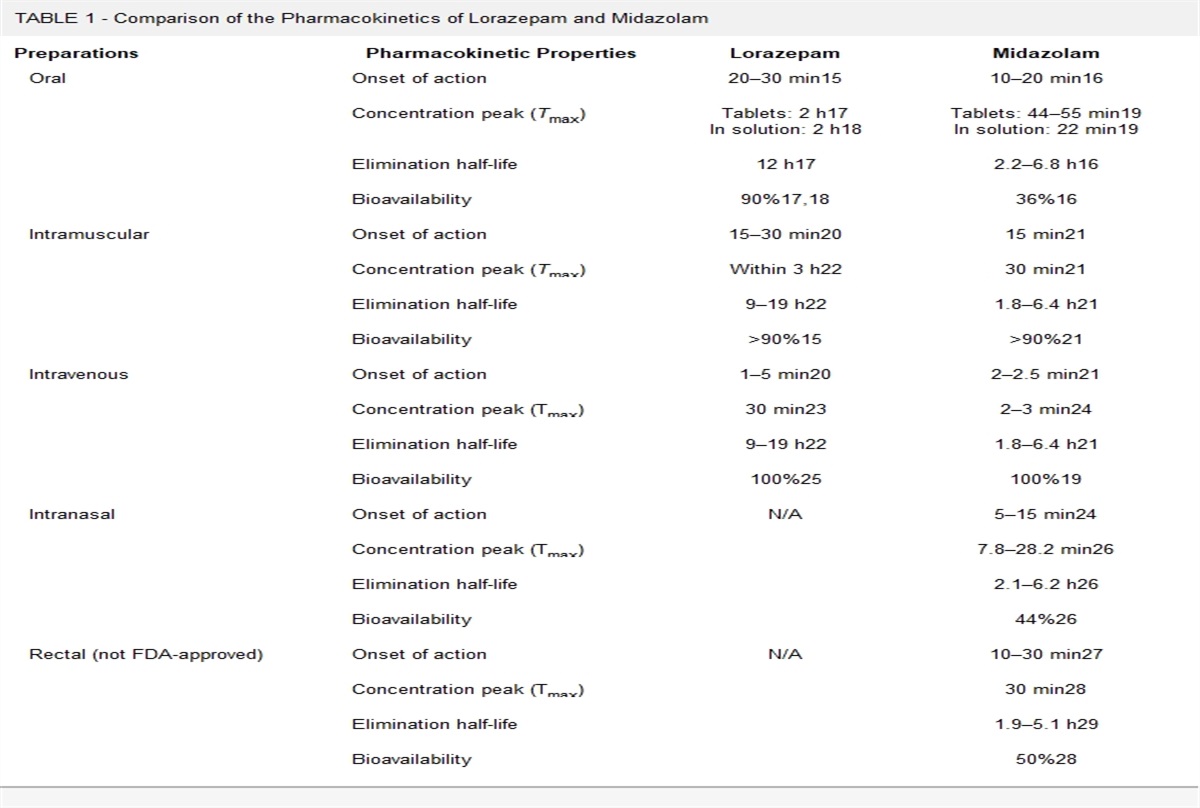
MATERIALS AND METHODS Study SynopsesDuring the clinical development of ER lorazepam, multiple phase 1 studies were conducted to evaluate its PK and safety profile (summarized in Table 1). Because IR lorazepam is typically given TID, the first study compared the steady-state PK profile of once-daily ER lorazepam to TID (every 8 hours [q8h]) IR lorazepam. As flexible administration is an important property of an anxiolytic, the second study explored the impact of food on bioavailability of once-daily ER lorazepam. Finally, because some patients experience difficulty swallowing solid oral dosage formulations,19,20 the third study examined the PK profile of ER lorazepam sprinkled onto soft food compared with that of intact capsule administration. This study also included a dose proportionality evaluation of the highest (1 × 4 mg) and lowest (4 × 1 mg) investigational dose forms for ER lorazepam (4 mg is higher than the maximum FDA-approved dose strength). Finally, a fourth study investigated ER lorazepam (4 mg once daily [QD]) compared with IR lorazepam 2 mg BID (every 12 hours), assessing the bioequivalence and safety of the ER formulation at a higher dose than the approved dose strength (Supplemental Materials, https://links.lww.com/JCP/A851).18
TABLE 1 - Summary of the Phase 1 ER Lorazepam Studies Study N* Study Type Primary Objective 1 43 ER/IR Randomized, open-label, 2-period, 2-sequence, 2-treatment, relative bioavailability Steady-state comparison of PK profile of ER lorazepam 3 mg QD and IR lorazepam 1 mg q8h (TID) 2 28 Randomized, open-label, 2-period, 2-sequence, 2-treatment, food-effect relative bioavailability Comparison of PK profile of QD ER lorazepam 4 mg under fed and fasted conditions 3 30 Randomized, open-label, 3-period, 6-sequence, 3-treatment, relative bioavailability Evaluation of the sprinkle effect of ER lorazepam 4 mg compared with the intact capsule; evaluation of dose proportionality of PK profile of ER lorazepam Supplemental study 4 69 ER,*Number of participants reflects the size of the PK population of each study.
q12h, every 12 hours.
For studies 1 to 3, participants were healthy adult men or women between the ages of 18 and 55 years, with a body mass index between 18 and 30 kg/m2 and a weight ≥60 kg. Inclusion criteria required all participants to have no major recent or ongoing clinically significant pathology, active or chronic disease, or clinically significant findings upon physical examination, vital sign collection, 12-lead electrocardiogram (ECG), or laboratory assessments. All assessments were made by the investigator or a certified physician to rule out any existing pathology. In study 1, participants were further screened using the Columbia-Suicide Severity Rating Scale. Pregnant or breastfeeding female participants were excluded. All women underwent a serum pregnancy test, and all participants had a urine alcohol, drug (including but not limited to cannabinoids, opioids, cocaine, phenylcyclohexyl piperidine, amphetamines, barbiturates, and benzodiazepines), and cotinine screen performed. Among other medical history criteria, participants were excluded if they had a recent exposure to any pharmacological agents with known interactions with benzodiazepines or agents that could interfere with the evaluation of ER or IR lorazepam. Each study was performed at a single institutional review board–approved research unit, and all participants provided written informed consent (see Supplemental Materials, https://links.lww.com/JCP/A851). Randomization (1:1) schedules were prepared using Worldwide Clinical Trials and SAS software, with each participant receiving treatment according to their assigned randomization schedule.
Study End Points/AssessmentsAll participants who received at least 1 dose of study treatment and had at least 1 postbaseline measurement were included in the safety population, whereas all participants who completed at least 1 treatment period and provided sufficient data were included in the PK population. The completer population included all participants who completed both study periods and had no major protocol deviations. The following general PK parameters were calculated for each study (see individual study methods hereinafter for specific parameters): total plasma clearance (CL/F), maximum plasma concentration (Cmax), time to reach maximum plasma concentration (Tmax), and area under the plasma concentration-time curve (AUC). Plasma concentrations of lorazepam were measured by liquid chromatography with tandem mass spectrometry (see Supplemental Materials for further details, https://links.lww.com/JCP/A851). Concentration-time data for lorazepam were analyzed using Phoenix WinNonlin (Version 8.1; Certara, L.P.) in conjunction with the Pharsight Knowledgebase Server (PKSO; Version 4.0.4; Certara, L.P.). Pharmacokinetic parameters were considered bioequivalent if the 90% confidence intervals (CIs) of the geometric mean ratios fell within the range of 80% to 125%. In all presentations of data and summary statistics, concentrations below the limit of quantitation were set to zero.
Safety assessments across the 4 studies included monitoring AEs, clinical laboratory tests (serum chemistry, hematology, and urinalysis), vital signs, ECGs, and physical examinations. Additional safety assessments in study 1 and supplemental study 4 included monitoring responses to the Columbia-Suicide Severity Rating Scale.
Study 1 Specific Methods: ER Lorazepam (3 mg) Compared With IR Lorazepam TIDStudy 1 was a randomized, open-label, 2-period, 2-sequence, 2-treatment, relative bioavailability, steady-state study comparing the steady-state PK profile of once-daily ER lorazepam 3 mg with that of IR lorazepam 1 mg q8h. The safety of once-daily ER lorazepam 3 mg and IR lorazepam 1 mg q8h after multiple doses to achieve steady-state levels was also evaluated. One hundred three participants were screened, and 46 were enrolled. Each participant received 2 separate multiple-dose administrations of treatment A (ER lorazepam 3 mg) QD or treatment B (IR lorazepam 1 mg) q8h. Participants were randomized to 1 of 2 treatment sequences, AB or BA, and were switched to the next treatment after a washout period of at least 10 days. During each treatment period, participants received their study medication each day from day 1 to day 8, and predose blood draws were taken on days 5 to 8 to verify that steady state had been achieved. Pharmacokinetic profile draws were then taken on day 8. For treatment A, these occurred each hour for the first 18 hours after dosing, then at 24, 36, 48, 72, 96, and 120 hours after dosing. For treatment B, blood draws occurred at 0, 0.5, 1, 1.5, 2, 3, 4, 6, 8, 8.5, 9, 9.5, 10, 11, 12, 14, 16, 16.5, 17, 17.5, 18, 19, 20, 22, 24, 30, 36, 48, 72, 96, and 120 hours after dosing. All participants received a standard diet while in the clinical research center and fasted overnight for a minimum of 8 hours before each morning dose on days 1 to 7 and for at least 4 hours after the morning dose on day 8. All participants had their meals between 4 and 10 hours after each morning dose and had a snack at least 13.5 hours after the morning dose. Participants receiving treatment B (q8h) took their evening meal at least 2 hours after the second (8-hour) dose and had a snack at least 2.5 hours before the third (16-hour) dose. Water was prohibited for 1 hour before each dose and for 2 hours after; at other times, it was allowed ad libitum.
Calculated PK parameters were analyzed using descriptive statistics and included maximum observed plasma concentration at steady state (Cmax,SS), time to reach Cmax,SS, minimum observed plasma concentration on day 8 at 24 hours after dosing (Cmin), average concentration at steady state (Cav), area under the plasma concentration-time curve for the dosing interval (AUCTAU,SS), area under the plasma concentration-time curve from time 0 to 24 hours after dosing (AUC0–24), percent fluctuation (Flu%), swing, apparent total plasma clearance at steady state (CLSS/F), and terminal elimination half-life (t1/2). Steady-state conditions were determined using linear square regression for each predose concentration on days 5 to 8.
Relative bioavailability for ER and IR lorazepam under steady state (day 8) was evaluated using an analysis of variance (ANOVA) model with ln-transformed Cmax,SS, Cmin, and AUCTAU,SS (AUC0–24 was used for treatment B). The statistical model contained treatment, period, and sequence as fixed effects and participants nested within sequence as the random effect. Statistical analyses were performed using appropriate software; for example, Phoenix WinNonlin (Version 8.1; Certara, L.P.) and SAS (Version 9.4; SAS Institute Inc).
Study 2 Specific Methods: Effect of Food on Bioavailability and PK Profile of ER LorazepamStudy 2 was a randomized, open-label, 2-period, 2-sequence, 2-treatment, relative food-effect bioavailability study, with the primary goal of comparing the PK profiles of once-daily ER lorazepam 4 mg under fed and fasted conditions in healthy adults. The study also included an evaluation of the safety and tolerability of once-daily ER lorazepam 4 mg.
Sixty-one participants were screened and 28 enrolled, with 27 completing both study periods. Participants reported to the facility at least 10 hours before the first scheduled dose and were assigned to either treatment sequence, AB or BA. During each treatment period, participants received a single dose of either treatment A (ER lorazepam 4 mg after an overnight fast of ≥10 hours; fasted condition) or treatment B (ER lorazepam 4 mg after an FDA-standard high-fat, high-calorie breakfast after an overnight fast of ≥10 hours, eaten 30 minutes before dosing; fed condition). The meal (~1000 calories total) consisted of 150 (15%) protein calories, 250 (25%) carbohydrate calories, and 500 to 600 (50%–60%) fat calories, with all meals and snacks being identical for all subjects. Participants were confined to the clinic from day −1 to 48 hours after dosing in each period. There was a washout of least 10 days between period 1 and period 2, upon which participants returned to the facility at day −1 of period 2 and received the alternate treatment as described previously. Pharmacokinetic profile blood draws occurred every hour from 0 (predose) to 16 hours after dosing, and then at 18, 24, 36, and 48 hours after dosing. Participants returned to the facility for subsequent blood draws at 72, 96, and 120 hours after dosing.
The following parameters were calculated for each participant in the PK population: CL/F, Cmax, Tmax, time at which the first quantifiable postdose concentration was observed (Tlag), t1/2, AUC0–12, AUC0–24, area under the plasma concentration-time curve from time zero to the last quantifiable concentration (AUClast), area under the plasma concentration-time curve from time zero extrapolated to infinity (AUCinf), and the percentage of AUCinf based on extrapolation (AUCExtrap). Comparisons of the PK parameters between treatments (fed vs fasted) were performed on ln-transformed Cmax, AUClast, and AUCinf using an ANOVA model (PROC GLM) with sequence, treatment, and period as fixed effects and subjects nested within sequence as the random effect.
Study 3 Specific Methods: Effect of Sprinkling Administration on Bioavailability of Once-Daily ER Lorazepam and Dose ProportionalityStudy 3 was a randomized, open-label, 3-period, 6-sequence, 3-treatment, relative bioavailability study with 2 primary goals: (1) to evaluate the PK profile of ER lorazepam 4 mg when sprinkled onto soft food compared with intact capsule administration in healthy adults, and (2) to evaluate the dose proportionality of the PK profile of ER lorazepam by comparing ER lorazepam 1 × 4-mg doses to ER lorazepam 4 × 1-mg dose under fasting conditions. Safety and tolerability of ER lorazepam were also evaluated.
Seventy-seven participants were screened and 30 enrolled, with 29 completing both study periods. Participants reported to the clinic on day −1 at least 12 hours before the first scheduled dose to ensure a 10-hour fast, and were assigned to 1 of 6 treatment sequences: ABC, BCA, CAB, CBA, ACB, or BAC, separated by a 10-day washout between doses in each period. Treatment A consisted of once-daily ER lorazepam 4 mg sprinkled on soft food (applesauce); treatment B was once-daily ER lorazepam 4 mg given as an intact capsule; and treatment C was once-daily ER lorazepam 1 mg given as 4 intact capsules.
From day −1 to 48 hours after dosing in each period, participants were confined to the clinic, with blood draws every hour from 0 (predose) to 16 hours after dosing, and then at 18, 24, 36, and 48 hours after dosing to obtain a PK profile. Participants returned to the facility for subsequent blood draws at 72, 96, and 120 hours after dosing. For each participant in the PK population, the following parameters were calculated: CL/F, Cmax, Tmax, Tlag, t1/2, area under the plasma concentration-time curve from time zero to time of the last quantifiable concentration (AUC0–t), AUC0–inf, and AUCExtrap.
Comparisons between treatment A and treatment B to assess the effect of administering ER lorazepam sprinkled over food were performed on ln-transformed Cmax, AUC0–t, and AUC0–inf using an ANOVA model. Relative bioavailability for ER lorazepam 4 × 1-mg capsules (treatment C) to ER lorazepam 1 × 4-mg capsule (treatment B) was evaluated using an ANOVA model with ln-transformed Cmax, AUC0–t, and AUC0–inf.
RESULTS Study 1: ER Lorazepam (3 mg) Compared With IR Lorazepam TID Study Population Demographics for Study 1In study 1, of 46 participants (safety population), 43 completed both treatment periods and were included in the analysis (PK population). Three withdrew early in the study for reasons unrelated to AEs (Supplemental Fig. S1A, https://links.lww.com/JCP/A851). The study population included healthy female (n = 12) and male (n = 34) adults ranging from 22 to 55 years of age. The key demographic data are summarized in Supplemental Table S1, https://links.lww.com/JCP/A851.
PK Results for Study 1In study 1, the concentration of lorazepam over time was similar throughout the 24-hour sampling window on day 8 for both ER and IR formulations (Fig. 1). Maximum mean concentrations of lorazepam were achieved at 11 hours after dosing for the ER (33.02 ± 9.83 ng/mL) compared with 1 hour after dosing for the IR (39.30 ± 12.69 ng/mL) formulation. As expected, participants treated with IR lorazepam q8h showed 3 peaks in lorazepam concentrations that corresponded to the timing of each of the 3 daily doses (Fig. 1). The PK profiles of ER and IR lorazepam were also similar on day 8, indicating similar bioavailability (see data summarized in Table 2).
 FIGURE 1:
FIGURE 1: Mean plasma concentration over time of once-daily ER lorazepam (3 mg) versus IR lorazepam q8h (1 mg TID) 24 hours after dosing on a linear scale (study 1). Mean values plotted, with error bars denoting SE of the mean.
TABLE 2 - PK Parameters of Multiple Doses of ER Lorazepam and IR Lorazepam on Day 8 Study 1: Once-Daily ER Lorazepam Compared With IR Lorazepam TID on Day 8 Parameter, Mean (SD) Unless Otherwise Noted ER Lorazepam QD 3 mg (n = 43) IR Lorazepam q8h 1 mg (n = 43) T max,SS, median (range), h 9.0 (4.0–14.0) 1.5 (0.8–3.0) C max,SS, ng/mL 35.3 (10.4) 40.7 (12.9) C min, ng/mL 24.8 (8.8) 29.1 (11.2) C av, ng/mL 28.9 (9.1) 31.9 (10.2) AUCTAU,SS, h × ng/mL 694 (218.9) 264 (85.1) AUC0–24, h × ng/mL 694 (218.9) 765 (244.4) t 1/2, h 17.8 (3.6) 17.6 (4.3) Flu, % [(C max-SS − C min)/C av]* 38.1 (12.9) 38.3 (12.0) Swing, % [(C max,SS − C min,SS)/C min,SS] 47.0 (21.0) 44.0 (16.0) CLss/F, L/h 4.8 (1.5) 4.3 (1.2)*Cmax,SS and Cmin obtained between time 0 and tau, where tau = 24 hours on day 8.
Flu, fluctuation; Tmax,SS, time to reach Cmax at steady state.
Bioequivalence was designated if the 90% CIs between geometric means of PK parameters were within 80% to 125%. In study 1, the 90% CIs of all 3 geometric mean ratios (ER to IR lorazepam given TID) for systemic lorazepam exposure for Cmax,SS, Cmin, and AUCTAU,SS fell within the bioequivalence range of 80% to 125% (Table 3). These data suggest that once-daily ER lorazepam 3 mg and IR lorazepam 1 mg q8h are bioequivalent.
TABLE 3 - Statistical Analyses of the Natural Log-Transformed Exposure of Multiple Doses of ER and IR Lorazepam in Study 1 Study 1: Once-Daily ER Lorazepam Compared With IR Lorazepam TID PK Parameter, Natural Log-Transformed Exposure ER Lorazepam* QD (n = 43) Geometric Mean IR Lorazepam* q8h (n = 43) Geometric Mean Geometric Mean Ratio ER/IR, % 90% CI C max,SS 33.8 38.9 86.9 84.6–89.2 C min 23.2 27.2 85.3 82.2–88.5 AUCTAU,SS 661 730 90.6 88.4–92.8*ER lorazepam administered as 3-mg dose QD; IR lorazepam as 1-mg dose q8h.
There were no serious AEs (SAEs) leading to study withdrawal in study 1. Treatment-emergent AEs (TEAEs) were reported in similar numbers by participants in both treatment groups: 36 TEAEs were reported by 19 participants (41.3%) receiving once-daily ER lorazepam, and 38 TEAEs were reported by 20 participants (43.5%) receiving IR lorazepam q8h (Table 4). The most frequently reported TEAEs (n ≥ 5 participants overall) were constipation (13% ER, 21.7% IR lorazepam), headache (6.5% ER, 8.7% IR), dizziness (8.7% ER, 2.2% IR), and insomnia (6.5% ER, 4.3% IR). A majority of TEAEs were mild in severity (n = 15 [32.6%] ER, n = 12 [26.1%] IR), with 4 and 8 participants reporting moderate TEAEs after ER and IR lorazepam, respectively. Moreover, there were no reports of abnormal physical examinations, clinical laboratory results, vital signs, or ECGs, or reports of suicidality.
TABLE 4 - Safety Overview of ER and IR Lorazepam From Study 1, Safety Population Study 1: Once-Daily ER Lorazepam Compared With IR Lorazepam TID AEs ER Lorazepam* QD (n = 46) IR Lorazepam* q8h (n = 46) All TEAEs, n (%), m 19 (41.3), 36 20 (43.5), 38 Most frequently reported TEAEs (n ≥ 5), n (%), m Constipation 6 (13.0), 6 10 (21.7), 13 Headache 3 (6.5), 3 4 (8.7), 6 Dizziness 4 (8.7), 4 1 (2.2), 1 Insomnia 3 (6.5), 4 2 (4.3), 2 TEAEs by severity, n (%) Mild 15 (32.6) 12 (26.1) Moderate 4 (8.7) 8 (17.4) Severe 0 0 TEAEs by relationship, n (%)† Related to study drug 14 (30.4) 16 (34.8) Not related 9 (19.6) 10 (21.7) All treatment-related TEAEs, n (%), m Constipation 6 (13.0), 6 10 (21.7), 12 Nausea 1 (2.2), 1 0 Headache 2 (4.3), 2 4 (8.7), 4 Dizziness 4 (8.7), 4 1 (2.2), 1 Somnolence 1 (2.2), 1 2 (4.3), 2 Paresthesia 1 (2.2), 1 1 (2.2), 1 Insomnia 2 (4.3), 3 1 (2.2), 1 Anhedonia 1 (2.2), 1 0 Euphoric mood 1 (2.2), 1 0 Vision blurred 3 (6.5), 4 1 (2.2), 1 Acne 1 (2.2), 1 0 Dermatitis acneiform 0 1 (2.2), 1 Decreased appetite 0 1 (2.2), 1 Back pain 0 1 (2.2), 1 SAEs, n (%) 0 0 TEAEs leading to study withdrawal, n (%) 0 0*ER lorazepam administered as 3-mg dose QD; IR lorazepam as 1-mg dose q8h.
†Participants were counted twice if they experienced both a related and an unrelated TEAE.
m, number of events; n, number of participants.
Twenty-eight participants enrolled in study 2 (safety and PK population), with 27 completing both treatment periods and included in the statistical analysis (completer population). One participant withdrew consent for reasons unrelated to AEs (Supplemental Fig. S1B, https://links.lww.com/JCP/A851). Key study demographics are summarized in Supplemental Table S2, https://links.lww.com/JCP/A851: overall, participants were healthy female (n = 9) and male (n = 19) adults aged 18 to 54 years.
In study 3, 30 participants were enrolled (safety population), with all 30 included in the PK population and 29 participants who completed at least 2 study periods included in the statistical analysis (completer population, Supplemental Fig. S1C, https://links.lww.com/JCP/A851). One participant was withdrawn by the investigator for an AE of oral herpes before period 2. Participants were healthy women (n = 9) and men (n = 21) ranging from 26 to 55 years of age. See Supplemental Table S2 for a summary of study demographics, https://links.lww.com/JCP/A851.
PK Results for Study 2 and Study 3Overall, mean lorazepam concentration-time profiles in study 2 were similar under either fasted or fed conditions (Fig. 2), with the first quantifiable lorazepam concentrations observed at 1 hour after dosing in both conditions. Maximum mean lorazepam concentrations were achieved 10 and 11 hours after dosing under fasted and fed conditions, respectively. Mean PK parameters were similar whether ER lorazepam was given with or without food, although administration with food delayed the median Tmax by ~2 hours (Table 5).
 FIGURE 2:
FIGURE 2: Mean plasma concentration-time profiles of once-daily ER lorazepam 4 mg taken under fasted or fed conditions, plotted on a linear scale (study 2). Mean values plotted, with error bars denoting SE of the mean.
TABLE 5 - PK Parameters of Once-Daily ER Lorazepam (4 mg) Administered in Fasted and Fed Conditions (Study 2) PK Parameter, Mean (SD) Unless Otherwise Noted Once-Daily ER Lorazepam (4 mg) Fasted (n = 27) Fed (n = 28) T max, median (range), h 10.0 (6.0–24.2) 12.0 (8.0–24.0) T lag, h 0.0 (0.0) 0.1 (0.5) C max, ng/mL 19.2 (5.1) 19.6 (3.2) AUC0–24, h × ng/mL 354 (92.5) 324 (54.0) AUCinf, h × ng/mL 937 (386.7)* 895 (329.6) t 1/2, h 17.6 (6.7)* 17.4 (6.6) CL/F, L/h 5.0 (2.2)* 5.1 (1.9)*n for these values was 26.
In study 3, overall PK parameters, including median Tmax, mean Cmax, AUC0–t, AUC0–inf, and t1/2 were similar for once-daily 4 mg (total daily dose) ER lorazepam regardless of being sprinkled on food, given intact, or given as 4 × 1-mg capsules (Figs. 3A, B; Table 6), where Tmax occurred at approximately 11 hours across all treatments. Mean plasma concentration-time profiles were nearly identical when once-daily ER lorazepam 4 mg was administered intact versus sprinkled on soft food (Fig. 3A, Table 6). Similarly, when comparing the highest and lowest dose forms, mean plasma concentration-time profiles seemed superimposable for once-daily ER lorazepam administered as either 1 × 4- or 4 × 1-mg capsules (Fig. 3B).
 FIGURE 3:
FIGURE 3: Mean plasma concentration-time profiles of once-daily ER lorazepam 4 mg sprinkled over food or taken as an intact capsule (A), and given as 1 × 4- or 4 × 1-mg capsules (B) plotted on linear scales (study 3). Mean values plotted, with error bars denoting SE of the mean.
TABLE 6 - PK Parameters of Once-Daily ER Lorazepam 4 mg When Sprinkled Onto Food, Taken as an Intact 1 × 4-mg capsule, or Taken as 4 × 1-mg capsules (Study 3) PK Parameter, Mean (SD) Unless Otherwise Noted Once-Daily ER Lorazepam Sprinkled (4 mg; n = 29) Intact (1 × 4 mg; n = 30) Intact (4 × 1 mg; n = 29) T max, median (range), h
Comments (0)