
Remember me

My husband of over 45 years, Philip Abbott, was the patient who will be discussed in this piece. He had an extremely rare and aggressive strain of prostate cancer. He was a computer consultant, and we had run our own successful business in the Yorkshire Dales for 11 years, when we decided to “escape to the country” back in 2000, having lived most of our married life in Dartford, an industrial town in Kent.
We decided to retire to Norfolk, a county we both loved, in 2011, and although very happy to be out of the world of IT, Phil did not want to fully retire. He became a bus driver for a centre for the disabled on a part-time basis and enjoyed not sitting behind a computer screen for hours every day, and it also gave him the exercise he needed to remain healthy (or so we thought).
Early SignsIn late 2014 he was becoming increasingly breathless and had a niggling ache in his chest. Having been diagnosed years back with a hiatus hernia, he just thought it was this playing up, but this was not so. In February 2015, after a bad scare and an overnight stay in our local hospital, Phil was found to have quite a significant blockage in his left ventricular coronary artery. He was successfully fitted with a stent and recovery was swift and amazingly uneventful.
All was well, and we decided to change our eating habits and lose some weight. Phil lost 2 and a half stone by cutting down on carbohydrates, which made him feel healthier than he had in quite some years.
At the end of January 2018, and with no other symptoms, Phil discovered a small amount of blood in his urine when he went to the bathroom. Although he felt well, we made him an appointment with our general practitioner (GP) to see if he had a kidney infection. Our GP arranged for a blood test to be done and performed a digital rectal examination of the prostate. This was found to be enlarged and a bit lumpy instead of being round and smooth. To be on the safe side, he referred Phil to a urologist.
I will add that when my husband was 65 years old in 2016, he went for his WellMan appointment with his GP and asked for a prostate specific antigen (PSA) test to be included with the other blood test. He was concerned, as although he showed no symptoms, he had lost two friends from prostate cancer just the year before. He was talked out of it by the GP, who said that it alone was not a very reliable test as an indicator and that it may give him false positive or negative results, so it was never done.
The Diagnosis Journey and Early TreatmentIn early February 2018, Phil attended the Urology department at the Norfolk and Norwich University Hospital (NNUH), where an ultrasound and a flexible cystoscopy were performed. The cystoscopy results confirmed a grossly abnormal prostate with a papillary lesion sitting on the median lobe of the prostate which projected into the bladder. The bladder itself was normal. More worrying though was the ultrasound result, which showed some incidental lesions on the liver. We were really becoming quite worried at that point and thought the worst.
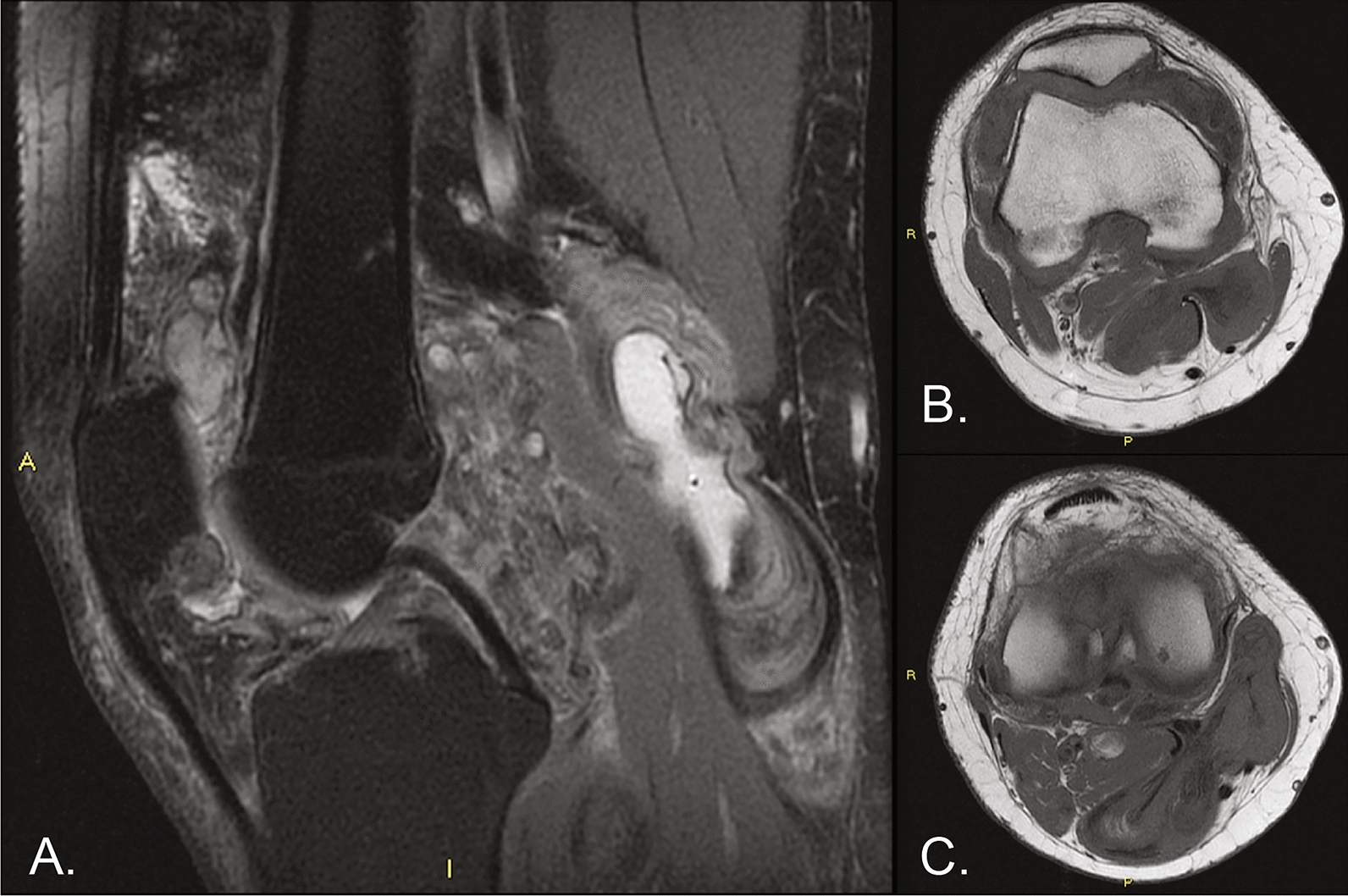
Computed tomography (CT) scans of the thorax and abdomen (Fig. 1) were arranged, and in late February 2018 Phil had a transrectal ultrasound scan and biopsy of the prostate. By the beginning of March, Phil had started to feel noticeably unwell, consumed by fatigue as well as dizziness, night sweats, a racing heart and aches in his body. So back to the GP we went, where she immediately contacted the medical registrar at the NNUH. With just yeses and noes and furtive looks from our GP, we began to expect the worst. They informed us to go straight to the walk-in department at NNUH.
Fig. 1
CT scan of the thorax and abdomen
Here we saw an oncology consultant Dr Jenny Nobes, who confirmed our worst nightmare when she diagnosed Phil with having Gleason 10 prostate cancer with a PSA of 9.5. She also suspected that he had widespread liver metastases, which could possibly be another primary cancer. What luck!
Although his prostate cancer was not curable, it could be managed quite well with medication and possibly chemotherapy, depending on a liver biopsy. The body scans had come back clear, with no spread to the lymph nodes or pelvic area.
Phil was started straight away with bicalutamide to take for 4 weeks and an injection of leuprorelin was arranged for 2 weeks later, which would need to be continued indefinitely. Dr Nobes also arranged for an urgent liver biopsy and prescribed dexemethasone to manage his liver symptoms.
On the 20 March, an ultrasound-guided biopsy of the liver was performed under general anaesthetic. A nuclear bone scan followed a few weeks later to see whether Phil’s cancer had spread into any bones. We waited 6 weeks for an appointment for the results, thinking that, had it been really bad, then the consultant would have been in touch straight away.
Advancement: Rare Small-Cell Prostate CancerAn appointment with the oncologist came on the 24 April 2018 – a day we will never forget, as it was here that we were delivered the shocking blow. Phil had an extremely rare and aggressive small-cell prostate cancer that had spread to the liver. The bone scan was clear, but nonetheless, the diagnosis was terminal. We were numb with shock and just looked at each other. We asked about chemotherapy, and Dr Nobes said that there was nothing that could be offered; in fact, chemotherapy in this case could prove fatal – another blow.
She said that in her 8 years as a consultant, she had only ever seen one case as rare as ours. Although she gave us the news with the utmost care and with great sensitivity, we were totally devastated. The palliative care team would be in touch, and she advised us to make any plans to visit anyone we needed to, sooner rather than later. After we could think again, I asked for a prognosis, to which the reply was “a few weeks”. I was in shock, so asked whether she instead meant a few months, and she again said, “no, a few weeks”. I wanted some plain speaking here; I needed to know just how much time we had left. The poor consultant was very uncomfortable saying this, but I had to know! Eventually, the answer came: “It could be as little as 6–8 weeks”.
We were understandably knocked down by this terrible news and were faced with the gut-wrenching task of telling our children and Phil’s family and friends. Our son, who lives in America, had been to visit in April after the first initial diagnosis and made swift arrangements to visit us in early June, thinking he could spend some more precious time with his dad. Our daughter and son-in-law, who live about 5 hours away visited soon after our tearful phone conversation and continued to support us as much as they could.
Phil’s work colleagues took him out and visited him at home, and friends who lived further afield came over to see us. Everyone was so saddened and could not believe the news.
The palliative care team sorted out everything needed to make him comfortable and helped with the forms for financial support. The worst form for me that he had to fill in was a do-not-attempt-cardiopulmonary-resuscitation form, which really hit the situation home and left me sobbing.
Phil really wanted to stay at home, but it soon became apparent that we could not manage physically as he became increasingly poorly. He ultimately changed his mind and asked to go into the local hospice when the time came. Sadly, the waiting list was quite long, and he did not have the luxury of time.
End of LifeContinuing to decline quite rapidly, Phil suffered from restless leg syndrome, for which he was prescribed ropinirole. His sleep was disturbed, and even lorazepam and oral morphine had little effect. I spent many a night with him on the edge of the bed unable to sleep and not knowing how to help him.
He contracted a painful skin infection on his thigh and lower back over the late-May bank holiday, and he was admitted by ambulance to our local James Paget Hospital Accident and Emergency (A&E), where he was put on intravenous antibiotics. By this stage, he was too weak and ill to fight, and although the antibiotics did clear up the infection well, he never really recovered from it. He was extremely uncomfortable for that last week because the location of the infection rash meant it was constantly agitated and left him wet and sore. Additionally, with his liver giving up, he also became heavy and bloated around his lower body and could not move without help. After 5 days in an A&E overflow ward, he was transferred to a side room in a ward more dedicated to cancer.
Our son got over to see his dad on 2 June 2018, and they had some quality hours together. My son and my daughter stayed with me, fed me and ferried me to and from to the hospital. I am not sure I would have coped on my own without them.
FarewellMy dear brave husband died on 4 June 2018 on his 67th birthday. He had one set goal – of reaching his birthday – which we were all so happy he achieved. This was exactly 6 weeks after being given the final diagnosis. He was taken too soon, and my heart was ripped out in the process.
Phil was always philosophical about the diagnosis. He accepted that there was nothing that could be done and said things such as “none of us will be getting out of this alive” and “it is what it is”. He kept his sense of humour even when he knew there was no hope. He also had so much praise for the National Health Service (NHS) staff and the ambulance service and was always grateful for the care he received, but I admittedly felt let down by the palliative care team.
I miss him terribly, but if my story can help those who read it and can encourage more research into rare prostate cancers so that maybe others in the future can get the help they need, then all was not lost.
I am grateful for the 6 weeks we had left together so that we could start to make plans that would help me after he passed, and so that we could say the things to each other and to others that needed to be said. Some wives kiss their husbands goodbye when they leave the house, only for them to never return again when fate deals them a blow. So at least we had those 6 weeks. They may have been the hardest and saddest weeks of our lives, but it is a time I will always cherish.
Questions from the Next of KinIt has been 5 years since Phil was first diagnosed with prostate cancer. I have reflected on this case and created a list of questions which I hope physicians treating this cancer will be able to address. I hope that these questions will be useful for patients and their close ones in better understanding this rare subtype of prostate cancer, and maybe even help guide further research in the area:
1. Why do these rare cancers mostly have a low PSA reading?
Answer: Small-cell carcinoma (SCC) of the prostate is composed of neuro-endocrine (NE) tumour cells, which are not associated with PSA production [1]. PSA levels therefore tend to remain disproportionately low and thus are not a reliable indicator of disease burden [1].
2. Could these rare cancers be present in the body long before any symptoms are felt or an advanced stage of diagnosis confirmed?
Answer: SCC of the prostate remains a rare prostate cancer subtype representing 0.5–2% of patients [2, 3]. It tends to follow an aggressive and rapid disease course with early metastatic spread [2, 3]. Common presenting symptoms include lower urinary tract symptoms such as hesitancy and dysuria or may relate to site of metastatic spread, for example, bone pain or respiratory symptoms [4]. Further research may inform reliable biomarkers to aid early diagnosis of prostatic SCC; however, given the disposition to rapid disease spread, patients unfortunately often present in the advanced stages of disease [1, 5, 6].
3. How are rare cancers such as these picked up, apart from the commonly used PSA? Of note, Phil had a full set of annual blood tests in late 2017, and all were normal as far as we knew.
Answer: PSA may aid diagnosis and monitoring of the more commonly diagnosed adenocarcinoma subtype of prostate cancer [7]. SCC of the prostate and prostate adenocarcinoma often present with similar clinical symptoms [4]. Although radiological evidence of osteolytic bone metastasis, compared with osteoblastic bone metastasis seen in prostate adenocarcinoma, may raise suspicion of prostatic SCC, diagnosis primarily relies on biopsy of suspected lesions and further histological classification [4, 5]. Potential diagnostic and monitorable biomarkers for prostate SCC have been identified but require further research to allow standard clinical implementation [1, 6].
4. Why were we only offered hormone therapy and steroids as a palliative treatment plan, having been told that chemotherapy could be fatal and so not an option?
Answer: Chemotherapy prescribing should carefully balance potential risks and benefits and aim to minimise patient morbidity and mortality [8]. Patients with evidence of organ dysfunction, such as deranged liver function tests and a deteriorating performance status as in the present case, are at higher risks of chemotherapy-related complications which can be life-threatening. Where the potential risks are judged too great, palliative input with prioritisation of symptom management is often more appropriate to maximise quality of life [8].
5. Will men ever be offered a screening programme to pick up these rare and aggressive forms of prostate cancer, before it becomes an advanced stage and incurable?
Answer: Despite its prevalence, screening programmes for prostate cancer remain contentious owing to a lack of evidence that modalities such as PSA measurements precipitate a significant mortality reduction [7]. Furthermore, there are concerns that screening may contribute additional risk and even harm to patients, such as unnecessary and invasive investigations and treatment [7]. Recent evidence following 15 year follow-up of the Prostate Testing for Cancer and Treatment (ProtecT) trial has, for example, demonstrated a low mortality regardless of patients with localised prostate cancer being assigned to active monitoring, prostatectomy or radiotherapy treatment [9]. Biomarkers such as chromogranin A, neuron-specific enolase or carcinoembryonic antigen have been identified as potential diagnostic and monitoring parameters for prostate SCC; however, these require further analysis and definition prior to implementation [1, 6]. Further clarification regarding the efficacy and modality of prostate cancer screening is therefore needed, particularly when considering histological subtypes.
Comments (0)