Implementation of the CME technique with central vascular ligation (CVL) as a standard procedure for right-sided colon cancers is still a matter of debate. There are concerns of higher morbidity and lengthened hospital stay due to the complexity of the procedure, and the effects on long-term survival are not yet completely clear, although good-quality evidence is gathering that suggests a survival benefit [6, 7].
Nevertheless, with a standardized technique and proper training, most authors in the literature find the CME procedure to be a safe alternative, with morbidity, mortality, and hospital stay not different from conventional right colectomies [8,9,10].
Recently, three randomized controlled trials have reported short-term results comparing CME with conventional laparoscopic right colectomies. The Chinese RELARC trial reported early safety results, with more intraoperative vascular injuries during CME procedures, but no difference in overall postoperative surgical complications and fewer Clavien–Dindo grade III–IV complications in the CME group [11]. The Italian randomized controlled trial by DiBuono et al. found no difference in postoperative complications, with significantly longer operation durations, higher lymph node yield, and better-quality specimens [12]. The Russian COLD trial also found no differences in short-term outcomes such as postoperative morbidity, hospital stay, and readmission rates, with better specimens and more lymph nodes in the CME group [13].
In our study, in line with most of the available literature, postoperative morbidity and length of hospital stay were not different in the CME and conventional groups, with no 30-day mortality occurring.
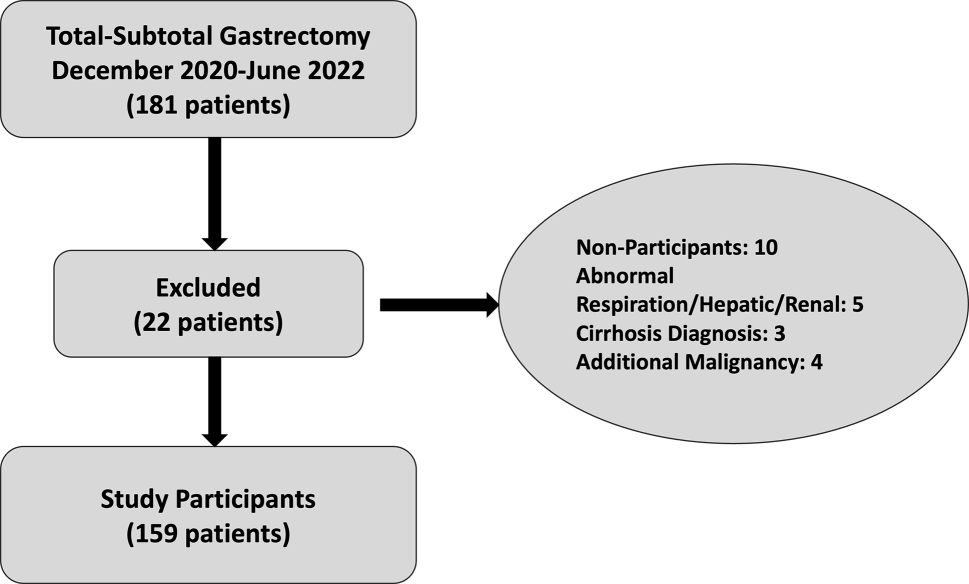
The prospectively recorded data came from a fairly large patient population (n = 131) from a single center, with procedures performed by the same small group of four experienced surgeons within a relatively short period of time (24 months). In our opinion, these factors reduce the heterogeneity of the procedures performed, and contribute to the quality of the comparison, even though the number of CME and conventional procedures were not evenly balanced. This imbalance between the number of CME (n = 28) and nCME (n = 103) cases, however, may have had a limiting effect on our study. As the procedure chosen in case of each patient was up to the surgeon’s clinical decision, this might be a source of unintentional bias, as some physicians were more likely to choose the conventional procedure over CME.
There was also a difference in the demographics of our study population, with more ASA III and older patients in the conventional (nCME) group. This might have had an impact on the rate of postoperative morbidity, even though the majority of postoperative periods (82% CME, 91% nCME; p = 0.166) were either uneventful or Clavien–Dindo 1–2. The significant difference in demographics is also probably the result of an unintentional selection bias, with surgeons reluctant to perform a more challenging procedure on frail and older patients. No such selection bias could be observed, however, considering BMI, which is a crucial technical factor in abdominal surgery and in CME procedures especially. It is also worth noting that the CME procedures investigated were performed in a standardized fashion after structured training and proctorship to ensure good-quality surgery and favorable outcomes.
As expected, the surgical time in CME cases was significantly longer compared to conventional right colectomies, but this did not result in higher morbidity or longer hospital stay. Our opinion is that this increase in procedure time is acceptable.
The lymph node yield of the CME right colectomies was also significantly higher in our study. This result coincides with most of the literature, with a generally higher node count compared to most reports [8, 12, 14]. Lymph node involvement in the central lymphatic region was separately recorded in CME patients. In CME specimens, only one patient had central involvement of 3+ out of 5 central nodes, besides having heavy node positivity in the D2 region as well.
The correlation between the increasing number of lymph nodes retrieved and improvement in long-term survival has long been established in colorectal cancer [15,16,17], and based on this evidence, current guidelines recommend removal of a minimum of 12 lymph nodes [18].
Besides total lymph node count, the rate of positive lymph nodes is also a strong prognostic marker in colorectal cancer, which makes more extensive lymphadenectomy reasonable [19].
An early retrospective study observed a significant difference in 5‑year disease-specific survival between CME and conventional groups in case of node-positive patients who underwent more extended lymphadenectomy (88% in CME vs. 50% in conventional) [14], and a large retrospective study in 2016 showed an increase in 5‑year cancer-related survival especially in stage III colorectal cancer (from 61.7% to 80.9%) with implementation of the CME technique [20]. More recently, another retrospective study also found a significant improvement in 3‑year OS and DFS in the CME group compared to the conventional group (93.5% and 91.6%, vs. 85.0% and 80.0%, respectively) [5] in UICC stage II and III disease. More robust evidence came from a large prospective population-based cohort study, which found a 5-year recurrence-free survival of 9.7% vs. 17.9% in CME vs. conventional right colectomy groups, respectively, with the CME procedure having an 8.2% risk reduction potential [21].
It is important to note that in the aforementioned prospective cohort study and a large meta-analysis [22], the beneficial long-term results of the CME procedure and radical lymphadenectomy regarding DFS and recurrence rate were most profound in node-negative UICC stage I and II patients. This suggests that CME and CVL with extended D3 lymphadenectomy may be the recommended procedure for all right colon cancers regardless of clinical suspicion of node involvement, especially considering the relative inaccuracy of preoperative nodal staging [23].
In our study, the ratio of node-positive to node-negative cancers in the CME and non-CME groups was comparable, and the decision to perform extended lymphadenectomy was not predominantly determined by preoperative staging.
This study has certain limitations. As the setup was non-randomized, the selection of patients for CME or conventional surgery was uneven, and ASA III patients were more likely to be selected for conventional surgery. This might have affected postoperative outcomes.
Laparoscopic and open procedures were not differentiated, as the ratio of open to laparoscopic cases in the CME and conventional (nCME) groups was comparable. Nevertheless, this might have increased heterogeneity.
This case–control study however has some considerable strengths. The surgical cases were performed at a single center, with standardized techniques, by a small group of experienced surgeons during a short period of time, which makes comparison of short-term results more reliable. The number of patients enrolled was relatively high (n = 131) in light of the available literature, and no patients were lost to follow-up.






留言 (0)