
Remember me


Chronic distal radioulnar joint (DRUJ) instability is a challenging problem of hand surgery practice. The complex motion and function of DRUJ make surgeons give special consideration to pathologies of this joint. DRUJ instability can occur in isolation or associated with dislocations, fractures and malunions of radius and ulna, and ligamentous injuries.1 Untreated DRUJ instability leads to alterations in wrist and forearm kinematics, which can result in loss of function and disability secondary to decreased grip strength, ulnar-sided wrist pain and degenerative changes.2
In case of mild instability in lower-demand patients, nonsurgical management including functional bracing, exercise program could be appropriate in the first-line treatment of chronic DRUJ instability. However, when there is gross DRUJ instability, pain, weakness, and failed nonsurgical management, surgical options should be considered. The common goals of the surgery are to increase stability and decrease pain while preserving wrist and forearm motions.
Proper bony alignment is a prerequisite for the stability of the DRUJ. Corrective osteotomy should be performed in case of a malunion accompanying DRUJ instability. However, soft tissue reconstruction is indicated in DRUJ instability with an irreparable triangular fibrocartilage complex (TFCC) when there is no bony malalignment or instability persists following bony correction.3 Several reconstruction techniques have been defined to re-create DRUJ stability. Soft tissue reconstruction procedures can be divided as extra-articular and intra-articular. Extra-articular procedures do not attempt to reconstruct the normal anatomy; however, these techniques create a tether directly between the ulna and radius or indirectly tether the joint using a tenodesis. On the other hand, intra-articular procedures attempt to mimic the normal anatomy by reconstructing the radioulnar ligaments. These intra-articular techniques are usually more complex and technically demanding than the extra-articular techniques.
Nakamura described a new technique in patients with chronic DRUJ instability.4 The technique combines both ligament reconstruction and tenodesis using a distally pedicled half-slip of the extensor carpi ulnaris (ECU) tendon graft. In the surgical technique, the graft is first passed through the TFCC remnants, and then through the bone tunnel made from the center of the fovea to the ulnar neck proximally. The ECU half-slip is then anchored to the ulnar fovea with an interference screw.4 The advantages of this technique are reconstruction of the foveal bundle of TFCC by an extra-anatomical way and stabilization of ECU in its groove. However, as the purpose is to reattach the TFCC to the fovea, this technique cannot be performed in cases when there is severe damage to the total structure of the TFCC. Moreover, making bone tunnel can be complicated with fracture or bone tunnel expansion in time which result in recurrent DRUJ instability.
We herein would like to present a new technique in the treatment of chronic DRUJ instability using hemi-ECU tendon graft without making a bone tunnel.
ANATOMYThe bony architecture of the DRUJ leads the joint inherently unstable. Shallower dimension and greater radius of curvature of the sigmoid notch compared with the ulna head result in both rotational and translational motion. This causes natural laxity of the joint. There are 4 types of sigmoid notch morphologies: flat type (42%), C type (30%), S type (14%), and ski slope (14%). Each of these variations of sigmoid notch have variable contribution rates on the stability of DRUJ. A cadaveric study demonstrated that only 20% of DRUJ stability was provided by bony constraints.5 This study shows that the stability of DRUJ is predominantly provided by surrounding soft tissue.
Soft tissue stabilizers of DRUJ can be divided into two; dynamic and static. The ECU tendon and the pronator quadratus form the dynamic stabilizers. They act as agonists/antagonists and stabilize the joint during pronation-supination when they are under tension. The static stabilizers of DRUJ are composed of interosseous membrane, ulnocarpal ligaments, joint capsule, and TFCC. The primary static stabilizers of the DRUJ are palmar and dorsal radioulnar ligaments which is a part of TFCC. Recent studies have focused attention on the distal oblique band, the thickened distal portion of the interosseous membrane. This bundle is present in 40% of the cases, and the presence of this bundle results in a significantly more stable DRUJ even TFCC is torn.
When the role of soft tissue stabilizers in the stability of DRUJ was examined, the palmar radioulnar ligament was found to provide the greatest restraint to dorsal translocation of the ulna and both interosseous membrane and dorsal-palmar radioulnar ligaments provide restraint to palmar translocation.5 The importance of each soft tissue stabilizer to DRUJ stability was demonstrated by an in vitro kinematic study. Gofton et al found that sectioning all soft tissues altered the DRUJ kinematics.6 However, normal DRUJ motion was observed when the radioulnar ligaments and TFCC were intact. Moreover, near-normal kinematics were observed after sectioning the radioulnar ligaments and preserving the remaining soft tissue constraints.
INDICATIONS/CONTRAINDICATIONSThe surgical indication for the present technique is chronic, symptomatic, gross DRUJ instability with TFCC foveal detachment. Furthermore, the articular cartilage of DRUJ should be in good condition and, sigmoid notch and ulnar styloid should be competent. The present technique is suitable for wrists with positive, neutral or negative ulnar variance unless there is a bony malalignment. Major symptoms of the patients are pain, mainly during pronation and supination, clicking, weakness, and loss of forearm rotation. Laxity should be assessed with the elbow against a table in forearm neutral, pronation, and supination, and then compared with the uninjured side. The anteroposterior drawer test or stress test is performed by locking the radius and rocking the ulna from the volar to the dorsal (Video 1, Supplemental Digital Content 1, https://links.lww.com/TIO/A59). A positive piano-key test shows DRUJ instability.
The technique is contraindicated in case of advanced DRUJ arthrosis, ulnar styloid nonunion, or chronic DRUJ instability with ulnar styloid atrophy. Moreover, any bony malalignment and sigmoid notch incongruity should be addressed before performing this reconstruction procedure.
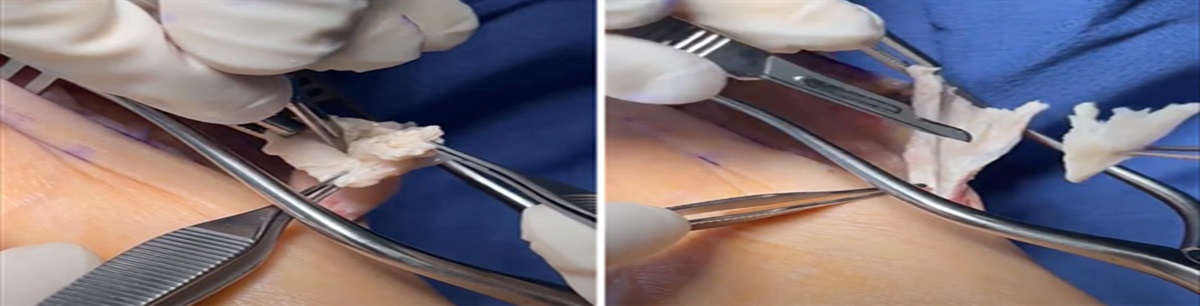
SURGICAL TECHNIQUEThe patient is positioned in the supine position under general or regional anesthesia. An upper arm tourniquet is applied. An approximately 8 cm, longitudinal, dorsal skin incision is made over the ECU tendon, starting from the tip of the ulnar styloid continued proximally. The dorsal sensory branch of the ulnar nerve is identified and preserved. ECU tendon sheath is incised, and distally based, ulnar-half ECU tendon graft is harvested (Fig. 1A, B). Next, a soft tissue tunnel is made with a right angle mosquito just beneath the TFCC and around the ulnar styloid (Fig. 2). The tendon graft is taken with mosquito forceps through this soft tissue tunnel and turned around the ulnar styloid (Fig. 3A). The tendon graft is then sutured to itself with pulvertaft weave technique under appropriate tension in neutral rotation (Fig. 3B). The tension and stability of DRUJ is checked with anteroposterior drawer test. Forearm rotation is checked for any limitations.
 FIGURE 1:
FIGURE 1: A, Half of the ECU tendon is incised distally. B, Distally based partial ECU tendon graft is harvested. ECU indicates extensor carpi ulnaris.
 FIGURE 2:
FIGURE 2: Soft tissue tunnel is made with a right angle mosquito just beneath the TFCC and around the ulnar styloid. TFCC indicates triangular fibrocartilage complex.
 FIGURE 3:
FIGURE 3: A, The tendon graft is turned around the ulnar styloid. B, The tendon graft is sutured to itself with the pulvertaft weave technique.
The patient is immobilized in a long-arm cast for 3 weeks in neutral rotation. The cast is then removed, and rehabilitation is initiated under the supervision of a hand therapist in the 3rd week (Video 2, Supplemental Digital Content 2, https://links.lww.com/TIO/A60).
EXPECTED OUTCOMESThe present study demonstrates a new technique using a distally based ECU tendon slip for the stabilization of DRUJ. Stabilization of DRUJ is provided through the stabilization of the distal ulna. In this technique, the ECU tendon acts as a static stabilizer besides its dynamic stabilizer effect. The ECU tendon slip is turned around the ulnar styloid and sutured back onto itself, which provides direct stability on the distal ulna in gross DRUJ instability with complete disruption of soft tissue stabilizers of DRUJ. Moreover, this technique also indirectly increases the stabilization of the DRUJ by tensioning the superficial portion of the radioulnar ligaments and the remaining soft tissue stabilizers in cases with incomplete disruption of soft tissue stabilizers.
The major advantages of this technique over others are straightforward technical application and a shorter operation time without a need for a bone tunnel. Thus, this technique avoids the complications related to bone tunnels, such as fracture, expansion of the tunnel, and loosening. This is especially important in osteoporotic patients. Furthermore, there is no need for any implant fixation which avoids implant-related complications.
COMPLICATIONSThe dorsal sensory branch of the ulnar nerve may be injured during exposure. Rupture of the tendon graft may occur if the graft is not harvested in sufficient thickness. The half thickness of the ECU tendon is appropriate to perform this technique. Infection and recurrent instability could be other possible complications of this procedure.
REFERENCES 1. Carr LW, Adams B. Chronic distal radioulnar joint instability. Hand Clin. 2020;36:443–453. 2. Mulford JS, Axelrod TS. Traumatic injuries of the distal radioulnar joint. Hand Clin. 2010;26:155e163. 3. Mares O. Distal radioulnar joint instability. Hand Surg Rehabil. 2017;36:305–313. 4. Nakamura T. Anatomical reattachment of the TFCC to the ulnar fovea using an ECU half-slip. J Wrist Surg. 2015;4:15–21. 5. Stuart PR, Berger RA, Linscheid RL, et al. The dorsopalmar stability of the distal radioulnar joint. J Hand Surg Am. 2000;25:689–699. 6. Gofton WT, Gordon KD, Dunning CE, et al. Soft-tissue stabilizers of the distal radioulnar joint: an in vitro kinematic study. J Hand Surg Am. 2004;29:423–31.
Comments (0)