
Remember me


Talectomy is generally used as a salvage procedure for managing failed ankle arthrodesis or arthroplasty, neuropathic arthritis, and post-traumatic osteonecrosis of the talus.1 Early talectomy is rarely indicated in comminuted fracture-dislocation or severely crushed open injuries of the talus especially in cases with bone loss.1 The late reconstruction procedure usually includes ankle arthrodesis which is accomplished by variable techniques.2 Herein we introduced a new modified technique using fibular strut autograft as a biological plate for augmentation of tibiocalcaneal arthrodesis with a nail.
CASE PRESENTATIONThe patient was a 42 years old man with open fracture-dislocation of the right talus because of falling from a height. After irrigation and debridement of the wound, primary talectomy was done owing to a large bone loss of the talar body and the ankle joint was temporarily fixed with a spanning external fixator. The second stage of surgical treatment was postponed for 6 weeks when the wound had been completely healed and there were not any clinical or paraclinical signs of active infection. The external fixator was removed 2 weeks earlier than the second stage to reduce the risk of infection.
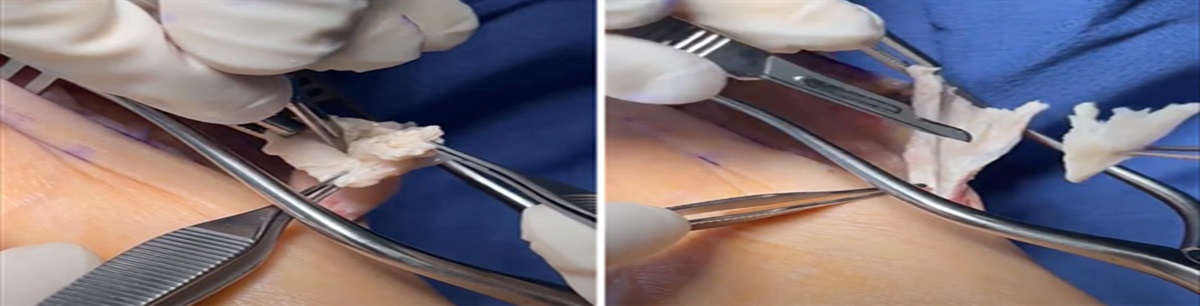
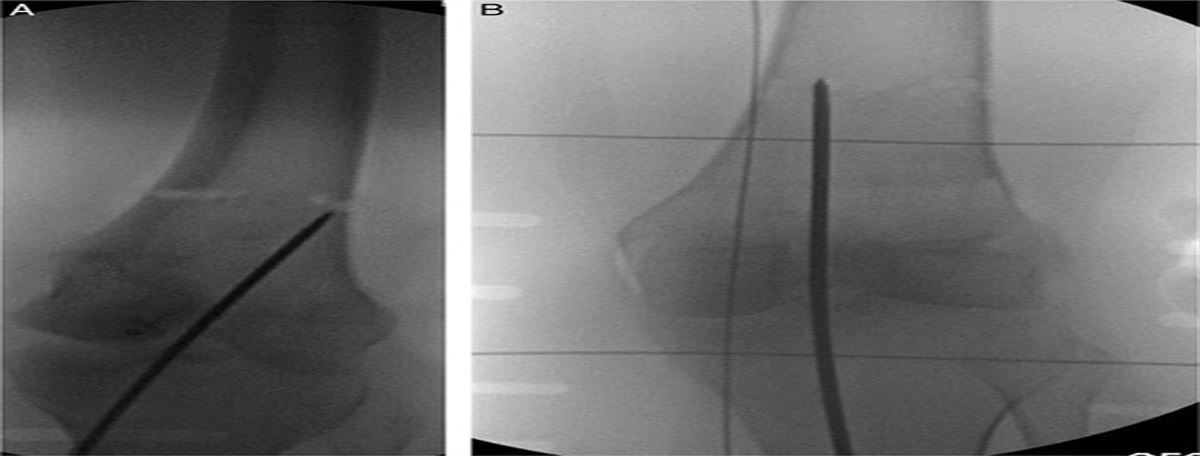
SURGICAL TECHNIQUEIn the second stage, under spinal anesthesia in the supine position, the subtalar and ankle joints were approached through a curved lateral skin incision. Lateral malleolus was detached from syndesmosis ligaments, mobilized, and extracted through the previous fracture line. After shaving articular surfaces of the tibial plafond and calcaneus using a narrow osteotome, the medial side of the distal tibia and calcaneus were decorticated. Irrigation and removing debris were intently done. Afterward, the femoral head allograft was shaved and reshaped by an oscillating saw. The prepared allograft was placed in the ankle mortise by an impactor (Fig. 1). In this stage of the procedure, a guide pin was inserted through the point in which the second ray line crossed the intermalleolar line at the plantar side of the foot. Under fluoroscopy control, the guide pin was passed through the allograft and got into the center of the tibia. Reaming was done and the nail was inserted over the guide pin from the calcaneus into the tibia. Thence, the distal fibular fragment was shaved and longitudinally split in the sagittal plane into 2 parts. One of them was used as morselized bone graft in the ankle joint and the other one was fixed to the decorticated lateral side of the distal tibia and calcaneus with 2 screws as a “biological plate” (Fig. 2). The screw which fixed the fragment to the distal tibia was passed through the dynamic hole of the nail (Figs. 3 and 4). After irrigating, the surgical wound was closed in 2 layers. A short leg splint was applied for 2 weeks postoperatively and changed to a short leg cast for the next 4 weeks. After removing the cast, the “controlled ankle motion” boot was continued until 3 months postoperatively. The patient was encouraged for nonweight bearing for 6 weeks and toe touched weight-bearing for the next 6 weeks. Anticoagulant agents were continued for 6 weeks. During 3-month follow up there was no complication clinically and radiographically. Postoperative visits will be continued for 9 months ahead with 3 months’ intervals to reassess the union of the fusion site.
 FIGURE 1:
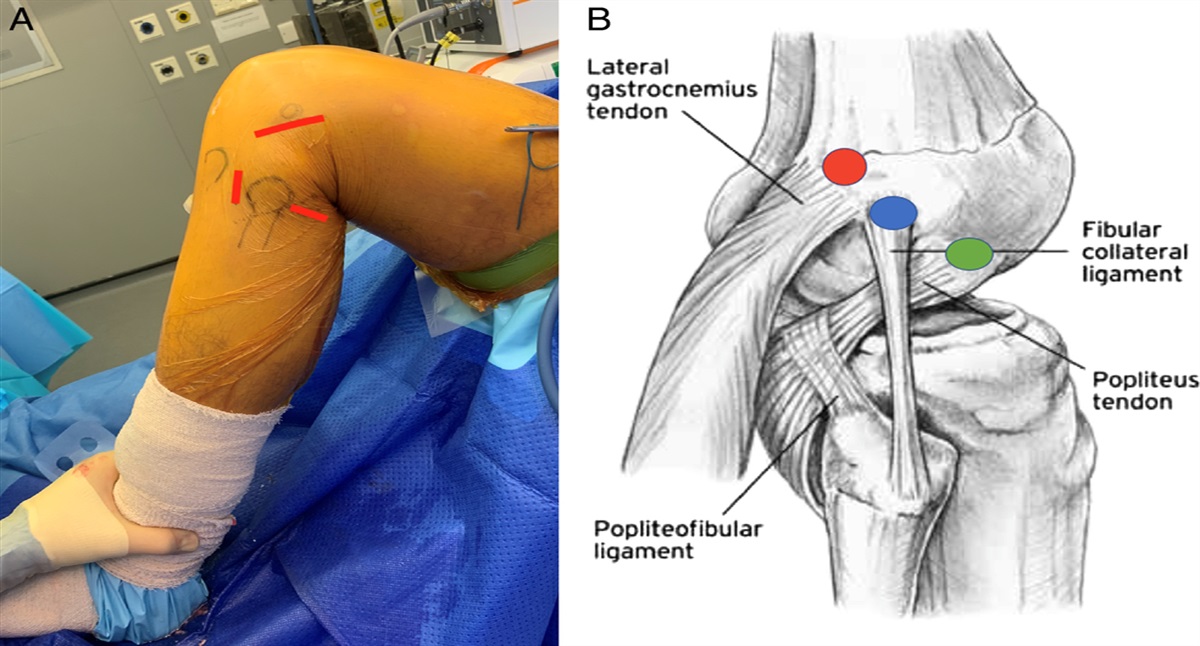
FIGURE 1: Intraoperative photography. Distal fibular fragment was extracted and femoral head allograft after preparing the ankle joint was inserted.
 FIGURE 2:
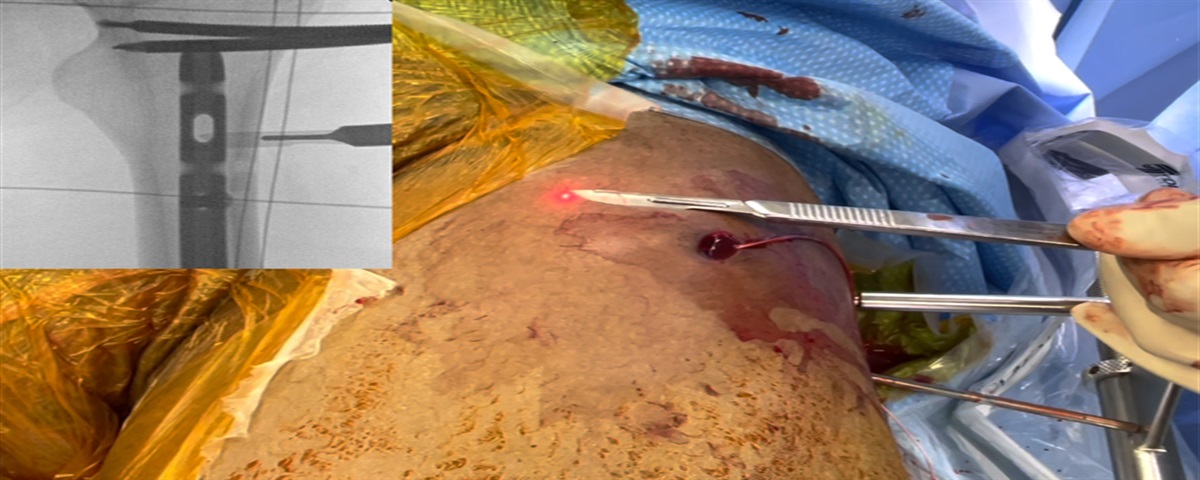
FIGURE 2: Intraoperative photography. Biological fibular plate was fixed to the fusion site with 2 screws.
 FIGURE 3:
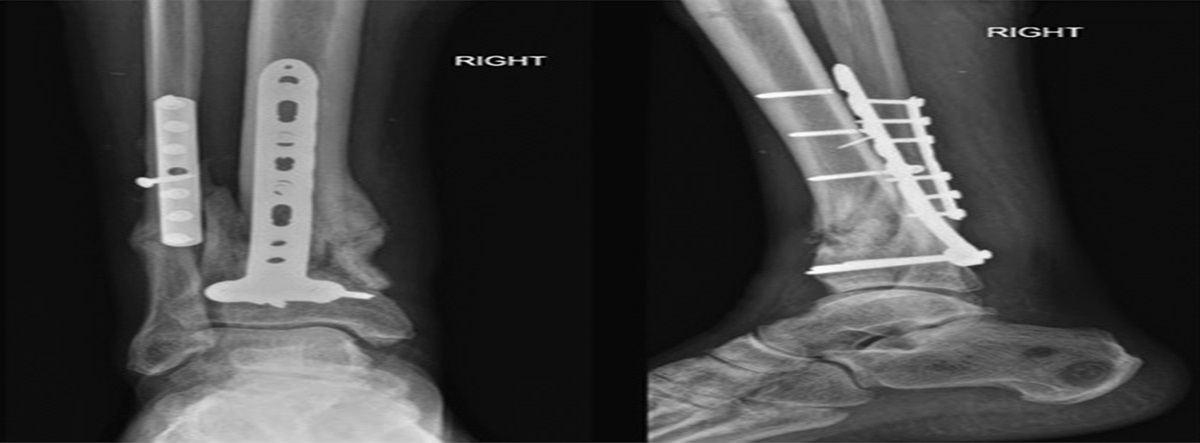
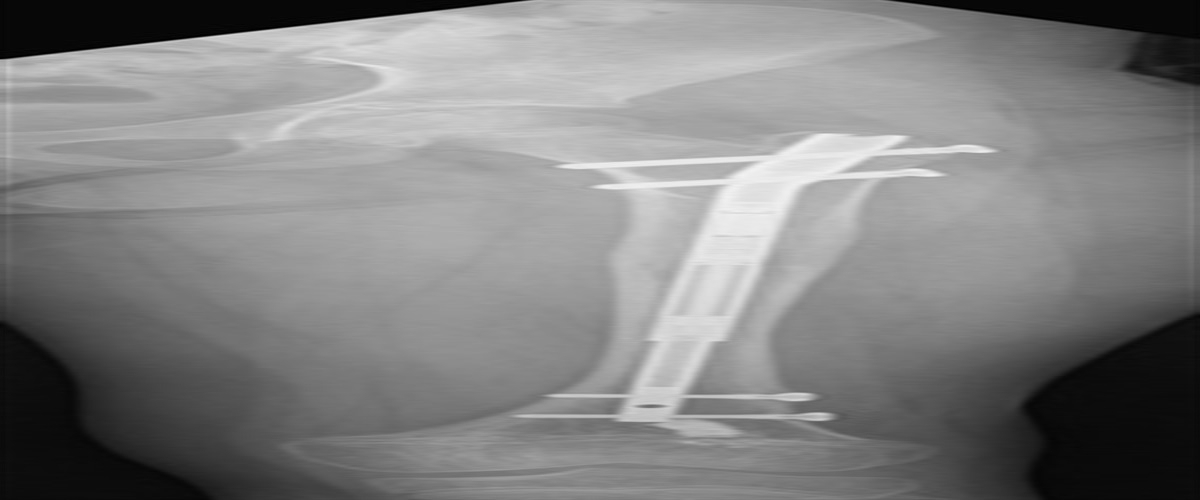
FIGURE 3: Postoperative anteroposterior radiography of right ankle demonstrated tibiocalcaneal fusion with intramedullary nail and biological fibular plate.
 FIGURE 4:
FIGURE 4: Postoperative lateral radiography of right ankle demonstrated tibiocalcaneal fusion with intramedullary nail and biological fibular plate.
DISCUSSIONTalectomy was first introduced in 1608 as a surgical treatment of open fracture of talus and used as a salvage procedure for persistent infection of talus over the past 300 years.1 Early excision of the talus combined with subsequent ankle arthrodesis is one of the surgical treatment options in open fracture-dislocation of the talus. Tibiocalcaneal arthrodesis could improve ankle stability and function after talectomy.2 There were variable techniques described for tibiocalcaneal arthrodesis. Tibiocalcaneal arthrodesis with crossed screws or retrograde nails is more common than the other techniques.3 Previous studies showed low complication rates and satisfactory outcomes of tibiocalcaneal arthrodesis using intramedullary nails.2 Furthermore, the application of interposition femoral head allograft for ankle arthrodesis with talar body defect showed satisfactory clinical outcomes.4 The transfibular approach and using the fibular fragment as morselized or strut interposition bone graft was previously described in the literature but related studies were extremely limited. Alessio Bernasconi and colleagues used the distal fragment of fibular osteotomy as strut interposition bone graft during tibiocalcaneal arthrodesis procedure with retrograde intramedullary nail. They sectioned the distal fibular fragment into 3 or 4 columns and placed them in the ankle joint to regain the height and fill the void.5 Derek Ley and Hassan3 used a fibular biological plate for augmentation of tibiocalcaneal arthrodesis with crossed screws. The authors mentioned that the aforementioned technique could provide stable fixation, reduce hardware requirement, and subsequently decrease the infection rate. The other advantages were obviating the additional incision for graft harvesting, less donor site morbidities, and shortening of surgical procedure time.3 Roukis and Kang6 used vascularized pedicle fibular onlay bone graft for augmentation of complicated tibiocalcaneal arthrodesis. We used a similar technique with some differences. Because of the complete detachment of the fibular fragment, we assumed the joint surface was more accessible and consequently the preparation of the joint surface was easier and more accurate in our technique. In contrast, halving the fibular fragment in the sagittal plane using a bone saw provides a flat contact surface that is perfectly matched with the prepared site on the lateral side of the calcaneus, allograft, and tibia. We believe that the use of vascularized pedicle fibular graft will limit the contact surface of calcaneus and fibular graft because of inadequate distal transfer of the graft. However, in our technique, this limitation is eliminated and the contact surface of graft and bone will be increased which consequently results in more stable construction. Lee et al7 also used almost a similar technique for tibiotalar arthrodesis. However, they transferred only the anterior part of the distal fibula as a strut graft for augmentation of tibiotalar arthrodesis. Furthermore, the arthrodesis was done using cannulated screws. In the current technique, we preferred intramedullary nailing for tibiocalcaneal arthrodesis because of more satisfactory outcomes and a more stable construct. Moreover, halving the distal fibula in the sagittal plan makes it possible to use half of the distal fibula as the morselized bone graft to improve the fusion process and the other part as a strut graft for augmenting the construction. We believed that fixation of fibular strut graft and intramedullary nail with a single screw through the dynamic hole of the nail provides stable fixation besides less hardware usage than fixation of the nail and biological plate separately. In contrast, using intramedullary nail provided more protection of strut bone graft against axial loads compared with arthrodesis with screws. Overall, advantages of the current technique are including; enhancement of stability with augmenting biological plate to intramedullary nailing, improvement of union rate of fusion because of morselized corticocancellous autografting, decreasing infection rate because of less hardware usage. The other advantage of this technique is obviating the additional incision for graft harvesting which is avoiding prolongation of procedure time and additional morbidities.
HIGHLIGHTS Utilization of fibular strut autograft as an augmented biological plate is a new technique of tibiocalcaneal arthrodesis with intramedullary nail. This technique provides more stable fixation besides rather biological advantages of autologous bone grafting without causing additional morbidities. Tibiocalcaneal arthrodesis with intramedullary nail provides more protection of strut bone graft against axial loads in compared with arthrodesis with crossed screws. Fixation of fibular strut graft and intramedullary nail with single screw through dynamic hole of the nail provides stable fixation besides less hardware usage than fixation of nail and biological plate separately. REFERENCES 1. Kharwadkar N, Nand S, Walker AP. Primary talectomy for severe fracture-dislocation of the talus with a 15-year followup: case report. Foot ankle Int. 2007;28:272–275. 2. Franceschi F, Franceschetti E, Torre G, et al. Tibiotalocalcaneal arthrodesis using an intramedullary nail: a systematic review. Knee Surg Sport Traumatol Arthrosc. 2016;24:1316–1325. 3. Derek Ley DPM, Hassan M. Can biological fibular plates provide viable fixation for tibiocalcaneal arthrodesis? Podiatr Today. 2020;33:4. 4. Coetzee JC, Den Hartog BD, Stone McGaver R, et al. Femoral head allografts for talar body defects. Foot Ankle Int. 2021;42:1071100720983811. 5. Bernasconi A, Patel S, Malhotra K, et al. Salvage tibiotalocalcaneal arthrodesis augmented with fibular columns and iliac crest autograft: a technical note. Foot Ankle Spec. 2021;14:79–88. 6. Roukis TS, Kang RB. Vascularized pedicled fibula onlay bone graft augmentation for complicated tibiotalocalcaneal arthrodesis with retrograde intramedullary nail fixation: a case series. J Foot Ankle Surg. 2016;55:857–867. 7. Lee DY, Kyung MG, Cho YJ, et al. A modified transfibular technique of ankle arthrodesis using partial fibular resection and onlay bone graft. PLoS One. 2020;15:e0241141.
Comments (0)