
Remember me


The incidence of periprosthetic fractures after total knee arthroplasty (TKA) and total hip arthroplasty (THA) is increasing, with reports as high as 2.5% after TKA and 5.5% after THA. Of these patients, 7% to 18%1 die within 1 year of surgical treatment. Early mobilization without restrictions and full weight-bearing in elderly hip and periprosthetic fracture patients is thought to improve mortality and morbidity, and accelerate functional recovery.2 Similar effects may be seen with other femur fracture patterns, including those around hip and knee replacements. Nonoperative management of geriatric hip fractures may result in prolonged immobilization, which can lead to bed sores, pneumonia, venous thromboembolism, and skin breakdown around the cast or brace.3 Butt and colleagues reported 2.6 times higher rate of complications in patients managed nonoperatively.
Management of periprosthetic fractures is based on implant stability and bone quality. Revision arthroplasty is often the treatment of choice when implant components are loose. Periprosthetic fractures about stable implants are often managed with open reduction internal fixation. When internal fixation is chosen, surgical goals include the restoration of length, alignment, and rotation while preserving the function of the adjacent prostheses.4 Operative management of displaced distal femur fractures includes plate fixation and or intramedullary nail placement. The chosen construct should be sufficiently stable to permit early mobilization. Similar clinical outcomes were found by Gill et al5 comparing surgical time and intraoperative bleeding using intramedullary nail versus plate fixation when the surgeon used the fixation method they were most comfortable with. When periprosthetic femur fractures are managed with open reduction internal fixation, the application of a second plate has been shown to increase the stiffness of the fixation construct.6 Performing biplanar plating through a single incision decreases the soft-tissue dissection and, in turn, the biological impact.7 Management of interprosthetic fractures is often challenging due to implant size and geometry. While biomechanically suboptimal, the use of cerclage cables or unicortical screws in areas not amenable to bicortical screw placement may be necessary.8,9
There are studies comparing different single and combination fixation constructs, but there is a lack of literature on dual plate fixation of periprosthetic femur fractures with immediate weight-bearing. The purpose of this study was to evaluate periprosthetic femoral fractures treated with biplanar plating and early ambulation.
MATERIALS AND METHODSThis study was approved by our Institutional Review Board. A retrospective chart review of periprosthetic femoral fractures between January 2016 and December 2020 was performed. One-hundred three patients were identified. Inclusion criteria of greater than 18 years of age, periprosthetic fracture with stable implants treated with lateral and anterior or posterolateral dual plating, and immediate postoperative weight-bearing were applied. Seven patients met the inclusion criteria (Fig. 1). Data collected included: age, sex, laterality, preoperative and postoperative ambulatory status, preoperative and postoperative living situation. AO/OTA and Lewis and Rorabeck classifications were applied. All fractures were simple patterns amenable to anatomic reduction with absolute stability for primary bone healing. No patients were identified who had fractures below a THA without ipsilateral TKA, thus, the Lewis and Rorabeck classification was applied.
 FIGURE 1:
FIGURE 1: One hundred three periprosthetic fractures were identified, each fracture was managed with either intramedullary nail, open reduction internal fixation, distal femoral replacement, or nail-plate combination based on fracture pattern, fracture location, and implant stability.
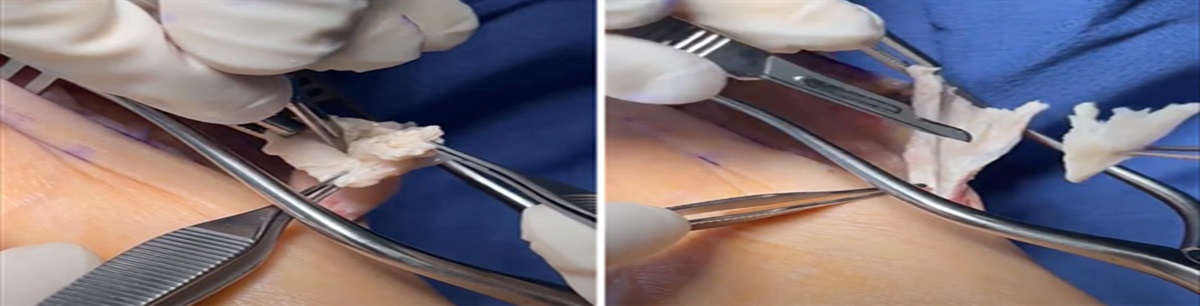
All patients were treated with a lateral femoral condylar plate and an anterior or posterolateral 3.5 mm reconstruction plate. A single, extensile lateral incision was used. Plate length was dictated by the length of the fracture and the presence or absence of total hip arthroplasty, total knee arthroplasty, or both. All patients were permitted to be weight-bearing as tolerated immediately postoperatively. Physical therapy notes were used to confirm that patients understood they were permitted to be WBAT. The senior author permits weight-bearing as tolerated in all geriatric femur fractures and all implants were stable.
The primary outcome was radiographic union, defined as 3 or 4 bridging cortices on orthogonal radiographs. Secondary outcomes were preinjury and postinjury level of functional independence and need for revision surgery. Descriptive statistics were used.
RESULTSSeven patients (6 female and 1 male) with an average age 79.7 (range 63 to 88) years were included (Table 1). All fractures were periprosthetic femur fractures, 4 patients had an ipsilateral, stable THA. There were 4 right and 3 left fractures. Two fractures were classified as 32A (diaphyseal) and 5 33A (supracondylar) per the AO/OTA classification. AO/OTA classification assigns a number to each bone and to the location within the bone.10 All fractures were classified as Lewis and Rorabeck type II (displaced fracture with intact prosthesis) and were amenable to an anatomic reduction and attempted primary bone healing.11 All fractures were low energy. The mean follow-up time was 18 (range 9 to 33) months.
TABLE 1 - Patient Demographics, Ambulatory Status, and Living Situation Patient Age Sex Side TKA THA Preoperative Ambulatory Status Postoperative Ambulatory Status Preoperative Living Situation Postoperative Living Situation Follow-up Duration (Mo) 1 63 M L Y N Cane Rolling walker Home Home 12 2 88 F L Y N Cane Rolling walker Home Home 9 3 87 F R Y Y Rolling walker Rolling walker Home Home 13 4 81 F R Y N Wheelchair Wheelchair Home Home 33 5 73 F R Y Y Rolling walker Rolling walker Home Home 25 6 84 F L Y Y Rolling walker Rolling walker Home Home 14 7 82 F R Y Y Rolling walker Rolling walker Skilled Nursing Facility Skilled Nursing Facility 21All patients were treated with a lateral large fragment locking plate and an anterior or posterolateral 3.5 mm reconstruction plate through a single lateral-based incision (Fig. 2). No differences were found when comparing the location of the second plate, anterior versus posterolateral. Patients started weight-bearing as tolerated immediately following surgery. All fractures achieved bony union after the index procedure with no hardware complications and revision surgeries documented. No infections were noted.
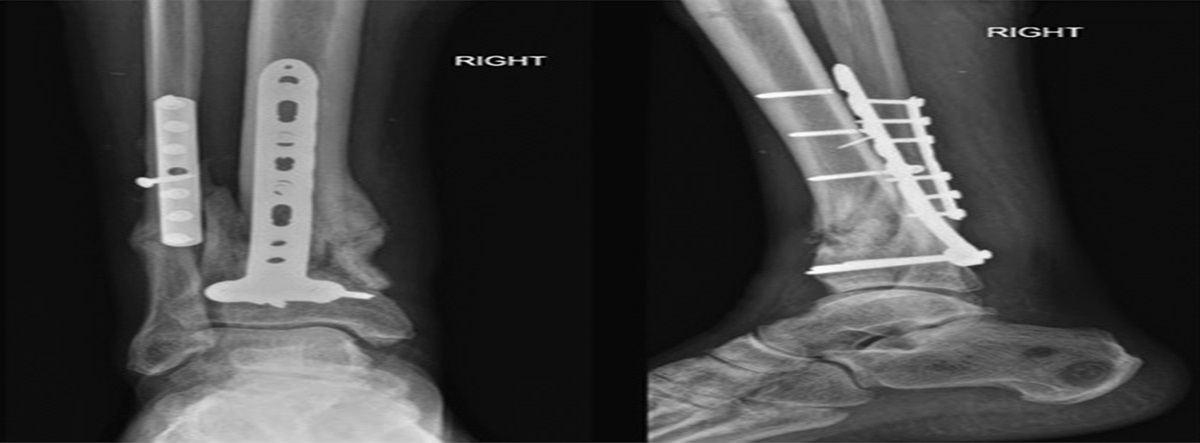
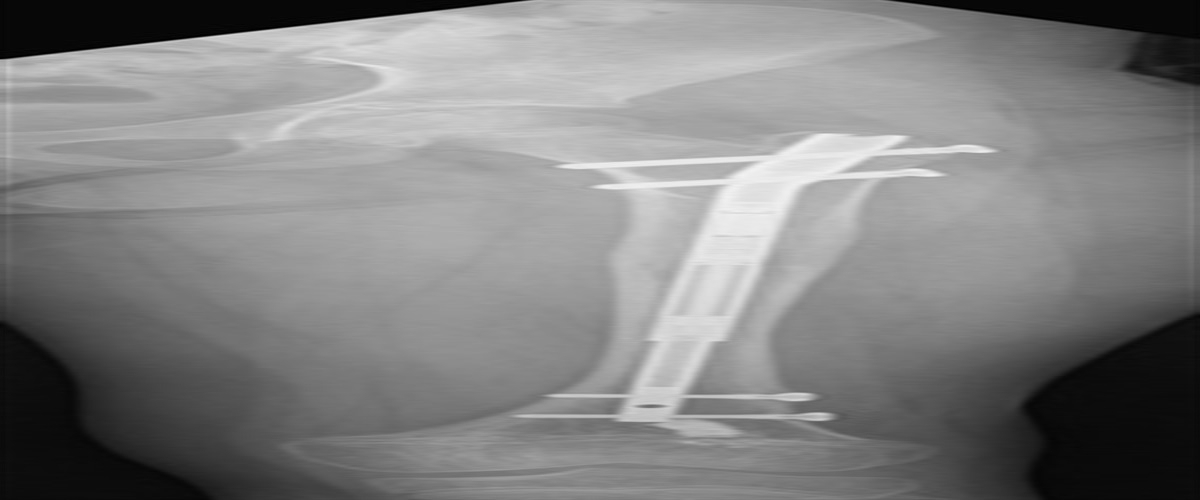
 FIGURE 2:
FIGURE 2: Injury (A) and 7-month follow-up images (B) for an 88-year-old woman treated with dual plating for an interprosthetic femur fracture.
Five (71%) of the 7 patients returned to their preoperative ambulatory status. The 2 patients that required additional ambulatory assistance were using a cane preoperatively and transitioned to a rolling walker postoperatively. All patients returned to their preoperative living environment. No mortalities were identified at a minimum of 1-year postoperative.
DISCUSSIONIn our small series, we had no fixation failures or reoperations, and all patients reached or came near to the prior level of function. Our results suggest that the technique of anatomic reduction and absolute stability accomplished by biplanar plating of geriatric periprosthetic femur fractures, above a TKA, with immediate weight-bearing can achieve satisfactory results.
Early mobilization without restricted weight-bearing in elderly patients improves morbidity and mortality, and accelerates functional recovery. Warren et al12 compared early postoperative complications and outcomes in hip fracture patients who were prescribed weight-bearing as tolerated postoperative day 1 and those who were not. Early weight-bearing postoperatively was associated with decreased morbidity and mortality. They calculated an odds ratio of 0.63 with a P value<0.001 when comparing early weight-bearing versus no-weight-bearing postoperatively in patients treated with cephalomedullary nails.
The concept of immediate weight-bearing for geriatric distal femur fractures is evolving and becoming more common. Beeres and colleagues utilized a helical shaped plate on the ventromedial side of the distal femur in eleven patients. Patients were weight-bearing as tolerated postoperatively, and all went on to bony union.13 Smith et al14 performed a study including 54 patients with stable prostheses who were treated with a single lateral locking plate fixation and immediate weight-bearing. Seventy-three percent of study participants returned to their preinjury ambulation status at 1-year postop. Three implant failures, 1 nonunion and 2 malunions were identified. Sah et al15 reviewed 22 consecutive interprosthetic femur fractures treated with a single-locking plate; 100% of patients went on to bony union. Full weight-bearing was not initiated until 6 weeks postoperatively.
Dual plating (medial and lateral) has been shown to increase the stiffness of the fixation construct and to help regain limb alignment but at the expense of increased soft-tissue dissection.7 Park et al6 performed a biomechanical comparison of single-side lateral plate to femur fractures managed with lateral plate and the addition of a medial locked plate. Load failure was 17.1% greater with the addition of a medial locked plate. Our experience with dual plating of femur fractures in a geriatric population through a single laterally-based incision builds on the findings of others supporting the use of dual constructs in this challenging patient population. This technique likely allows for some of the biomechanical advantages of medial and lateral plating without the additional surgical incision. This, in theory, decreases operative time and should have less of a biological impact.
This study has several limitations. The retrospective nature of the study should be considered. While we attempted to capture all patients within our center, follow-up was not standardized, and there is the potential that some patients were not identified. Our sample size is small at 7 cases and includes primarily fractures that are amenable to an anatomic reduction. An extensible lateral approach, while well tolerated, carries the increased risk of vascular compromise and extended operative times compared with less invasive methods.
CONCLUSIONThe management of periprosthetic femoral fractures is dependent upon the location of the fracture and implant stability. Our results support the possibility of immediate weight-bearing in geriatric periprosthetic femur fractures treated with anatomic reduction and biplanar plating through a single lateral incision, although additional study is needed.
REFERENCES 1. Garner MR, Carmen E Quatman Considerations in Common Geriatric Fractures: Proximal Humerus, Distal Radius and Distal Femur. In: Orthopaedics Knowledge Update Trauma 6. 2. Kubiak EN, Beebe MJ, North K, et al. Early weight bearing after lower extremity fractures in adults. J Am Acad Orthop Surg. 2012;21:727–738. 3. Butt MS, Krikler SJ, Ali MS. Displaced fractures of the distal femur in elderly patients. Operative versus non-operative treatment. J Bone Joint Surg Br. 1996;78:110–114. 4. Nauth A, Ristevski B, Begue T, et al. Periprosthetic distal femur fractures: Current Concepts. J Orthop Trauma. 2011;26:82–85. 5. Gill S, Mittal A, Raj M, et al. Extra articular supracondylar femur fractures managed with locked distal femoral plate or supracondylar nailing: a comparative outcome study. J Clin Diagn Res. 2017;11:RC19–RC23. 6. Park KH, Oh CW, Park IH, et al. Additional fixation of medial plate over the unstable lateral locked plating of distal femur fractures: a biomechanical study. Injury. 2019;50:1593–1598. 7. Scolaro J, Schwarzkopf R. Management of interprosthetic femur fractures. J Am Acad Orthop Surg. 2017;25:63–69. 8. Rozell J, Delagrammaticas D, Schwarzkopf R. Interprosthetic femoral fractures: management challenges. Orthop Res Rev. 2019;11:119–128. 9. Lewis GS, Caroom CT, Wee H, et al. Tangential bicortical locked fixation improves stability in Vancouver B1 periprosthetic femur fractures: a biomechanical study. J Orthop Trauma. 2015;10:364–370. 10. Meinberg EG, Agel J, ROberts CS, et al. Fracture and dislocation classification compendium—2018. J Orthop Trauma. 2018;32:S1–S10. 11. Rorabeck CH, Taylor JW. Classification of periprosthetic fractures complicating total knee arthroplasty. Orthop Clin North Am. 1999;30:209–214. 12. Warren J, Sundaram K, Anis H, et al. The association between weight-bearing status and early complications in hip fractures. Eur J Orthop Surg Traumatol. 2019;29:1419–1427. 13. Beeres F, Emmink B, Lanter K, et al. Minimally invasive double-plating osteosynthesis of the distal femur. Oper Orthop Traumatol. 2020;32:545–558. 14. Smith W, Stoneback J, Morgan S, et al. Is immediate weight bearing safe for periprosthetic distal femur fractures treated by locked plating? a feasibility study in 52 consecutive patients. Patient Saf Surg. 2016;10:26–31. 15. Sah AP, Marshall A, Virkus WV, et al. Interprosthetic fractures of the femur: treatment with a single-locked plate. J Arthroplasty. 2010;25:280–286.
Comments (0)