Recommendation 1: Initial evaluation should include a focused history and physical examination. A full panel of blood tests including blood gas and lactate levels are also important to look for suggestions of bowel ischemia. Grade of recommendation: Strong recommendation, based on low- or very-low-quality evidence, 1C.
Symptoms of sigmoid volvulus include abdominal pain, constipation and vomiting (a late sign) [4,5,6, 9, 19, 27, 28]. In 30–41% of cases, patients report previous episodes of abdominal distention [3]. This triad is much more common in endemic volvulus, rather than the sporadic kind of volvulus (88% versus 33%) [28].
In the “volvulus belt” countries, the clinical presentation may be acute with peritonitis and shock. In this fulminant clinical presentation, the prognosis is poor because colonic necrosis and perforation would possibly have already occurred, by the time the patient first presents for care [25]. Conversely, in Western countries, the patient usually presents 3 to 4 days after the onset of symptoms [26]. The classic patient is elderly, institutionalized and under psychotropic medications that causes chronic constipation. The history should elicit the above-mentioned risk factors, including a personal history of previous sigmoid volvulus, which is present in 30–40% of cases.
Classically, the clinical examination will identify abdominal distension, diminished bowel sounds and often an empty rectum on digital examination [2, 20, 27,28,29]. However, the examination is often difficult due to the presence of abdominal distension, which is the result of colonic obstruction of several days duration; if there are no signs of peritoneal irritation, as is often the case, this may result in a delay in diagnosis. Nonetheless, the absence of peritonitis does not indicate the absence of bowel ischemia. Asymmetric gaseous abdominal distention associated with emptiness of the left iliac fossa is pathognomonic for sigmoid volvulus, though this can be very challenging to detect [5].
The duration of symptoms lasts from a few hours to several days [5, 20, 21, 26,27,28, 30,31,32]. As these patients are typically old with comorbidities, any vomiting and dehydration can tip them over into renal insufficiency. Thus, blood testing of electrolytes and renal function is necessary.
Bear in mind that as these patients may have neuropsychiatric issues, history may not be forthcoming or accurate. The physical examination and testing of blood gas and lactate levels are crucial, although bowel ischemia may be present in the absence of hyperlactatemia.
Recommendation 2: Diagnostic imaging for sigmoid volvulus is initially based on plain abdominal radiographs, showing a classic coffee bean sign. Grade of recommendation: Strong recommendation, based on low- or very-low-quality evidence, 1C.
Plain abdominal radiographs are often diagnostic of sigmoid volvulus. Chest radiographs are also sufficient to detect the presence of free air, in cases of perforation. Imaging should be done expediently. The classic finding is that of a coffee bean, projecting toward the upper abdomen, sometimes above the transverse colon, which has been described as the “northern exposure sign” [5, 29, 33,34,35,36,37].
Recommendation 3: CT imaging can be used in cases where the diagnosis is in doubt, or if ischemia or perforation is suspected. Grade of recommendation: Strong recommendation, based on low- or very-low-quality evidence, 1C.
In cases in which clinical assessment and plain abdominal radiographs are insufficient to confirm the diagnosis of sigmoid volvulus, or if a complication is suspected (e.g., impending ischemia), urgent CT imaging is indicated. When performing CT imaging, the use of intravenous contrast can facilitate the diagnosis of colonic ischemia [35, 36, 39,40,41]. In the study by Swenson et al. [21], the positive diagnostic yield of CT for sigmoid volvulus was 89%. Other diagnoses that can mimic the presentation of colonic volvulus, such as obstruction due to a neoplasm or pseudo-obstruction, can also be evaluated with the above modalities.
The addition of a contrast enema may help confirm the diagnosis of sigmoid volvulus by demonstrating a “bird’s beak” sign, at the point of colonic torsion [5, 24, 28, 33, 37, 38]. However, an enema is strictly contraindicated when perforation is suspected. When using a contrast enema, a water-soluble contrast is much preferred over barium contrast, because the latter could cause a chemical peritonitis in the setting of a perforated colon.
Recommendation 4: In patients in whom ischemia or perforation is not suspected clinically and/or radiologically, flexible endoscopy should be performed as a first line to decompress the sigmoid colon. Grade of Recommendation: Strong recommendation, based on low- or very-low-quality evidence, 1C.
In the absence of colonic ischemia or perforation, the initial treatment of sigmoid volvulus is urgent endoscopic detorsion, which is effective in 60–95% of patients [3, 21, 22, 27, 42,43,44]. Endoscopic detorsion carries a 4% morbidity, and some series show a 3% mortality rate [22, 27, 45].
Successful detorsion implies that the endoscopist must visualize and go past the transition points (typically 2 points are found) [2, 20, 22, 45, 46]. At the end of detorsion, endoscopic view of the mucosa to assess sigmoid colon viability is mandatory. After successful detorsion of the sigmoid colon, a decompression flatus tube should be left in place to maintain the reduction, allow for continued colonic decompression, and facilitate mechanical bowel preparation as needed [2, 20,21,22, 43, 44, 47,48,49,50,51,52].
After successful endoscopic detorsion, long-term recurrence has been observed in 43% -75% of patients [20,21,22, 26, 47, 52, 53]. As each future episode of volvulus carries its attendant risks of ischemia or perforation, operative intervention should be strongly considered during the index admission or soon thereafter [20,21,22, 26, 52, 54].
The literature favors flexible endoscopy over rigid endoscopy because of its superior diagnostic performance, particularly in assessing ischemia and because of its lower perforation rate [36]. Rigid sigmoidoscopy can fail to diagnose sigmoid volvulus and miss ischemia in up to 24% of cases.
The favorable impact of colonoscopy is perfectly illustrated in Turkey’s very large retrospective series that compiled 952 patients, over a period of 46.5 years [22]. Colonic decompression had evolved from the initial use of barium enema (1966–1968), to rigid sigmoidoscopy (1968–1988), to the introduction of the flexible endoscope in 1988, and exclusive use of flexible endoscopic decompression from 2003 onwards. In the Turkish experience, barium enema resulted in successful decompression in 69% of cases but was burdened with a morbidity of 23%, a mortality of 8% and early recurrence in 11% of cases. With rigid sigmoidoscopy, the authors observed successful decompression, morbidity, mortality and early recurrence rates of 78%, 3%, 1% and 3%, respectively. With the advent of flexible endoscopy, rates of successful decompression, morbidity, mortality and early recurrence were 76%, 2%, 0.3% and 6%, respectively.
Yassaie et al. [47] described 31 patients with sigmoid volvulus who underwent successful endoscopic detorsion and no further interventions. Recurrent volvulus was diagnosed in 19 (61%) of these patients at a median of 31 days. Of these 19 patients, 7 underwent colectomy and 12 had repeat endoscopic detorsion alone, of whom 5 (48%) were diagnosed with a third episode of volvulus at a median interval of 5 months and 3 (25%) required emergent sigmoid colectomy [47].
Nonetheless, in cases in which advanced mucosal ischemia, perforation or impending perforation of the colon are discovered during endoscopy, the procedure should be aborted. Emergency colectomy is warranted in these cases.
There seems to be little role for a completion screening colonoscopy before surgery, mainly because of its technical difficulty. The colon is often extremely long and redundant, with angulations that are difficult to traverse. Preoperative total colonoscopy should be offered only if there is clinical or radiological suspicion of underlying neoplasia [21, 55, 56].
Endoscopy is therefore limited in most cases to short flexible colonoscopy performed during endoscopic detorsion, which also rules out neoplastic obstructions at the rectosigmoid junction, the other principal entity in the differential diagnosis. In case of diagnostic uncertainty, a virtual colonography can be performed instead of total colonoscopy.
Recommendation 5: Urgent sigmoid resection is indicated when endoscopic detorsion of the sigmoid colon is not successful and in cases of non-viable or perforated colon. Strong recommendation, based on low- or very-low-quality evidence, 1C.
In 5–25% of patients with sigmoid volvulus, they will present with colonic ischemia, perforation, peritonitis or septic shock on admission. These patients require upfront urgent colectomy [2, 4, 20,21,22, 26, 27, 42, 49, 57,58,59,60,61]. Intraoperatively, resection of infarcted bowel should be performed without detorsion and with minimal manipulation to prevent release of endotoxin, potassium and bacteria into the general circulation and to avoid perforation of the colon [24, 51, 62,63,64].
The decision to perform an isolated sigmoid colectomy versus a high anterior resection should be individualized. However, since this is a benign pathology, a full oncological anterior resection is not typically needed. The main consideration would be the vascular supply of the remnant colon. The decision to perform primary colorectal anastomosis, defunctioned colorectal anastomosis or end colostomy should be individualized, with consideration of both the overall condition of the patient and the colon.
Kuzu et al. [60] reported on 106 sigmoid volvulus cases accumulated over 8 years. They performed sigmoid resection with end colostomy (Hartmann procedure, n = 49) or sigmoid resection with colorectal anastomosis without diverting ostomy (n = 57). A Hartmann procedure was used more often in patients with a non-viable colon or peritonitis and resulted in increased postoperative complications and mortality (8% vs 5%), whereas anastomotic leak occurred in 7% of patients in the anastomosis group [60].
Atamanalp et al. [20] reported on 952 patients with sigmoid volvulus. In this series, a Hartmann procedure was the most commonly performed emergency operation, with overall morbidity of 42% and mortality of 20%. Coban et al. [60] reported on sigmoid resection with non-diverted or diverted colorectal anastomosis and found 12% and 0% anastomotic leaks and a mortality rate of 8% and 10%, respectively.
Overall, there are insufficient data to support one technique over another in emergent cases for sigmoid volvulus, as most show no difference in mortality or overall surgical postoperative complications among the various approaches [57,58,59, 65, 66]. Despite the evidence, end colostomy creation is often the most appropriate choice for hemodynamically unstable patients or when there are significant concomitant factors, such as increased ASA or Acute Physiology and Chronic Health Evaluation II score, coagulopathy, acidosis or hypothermia, all of which add prohibitive risk to the integrity of a colorectal anastomosis [22, 58, 60, 67,68,69].
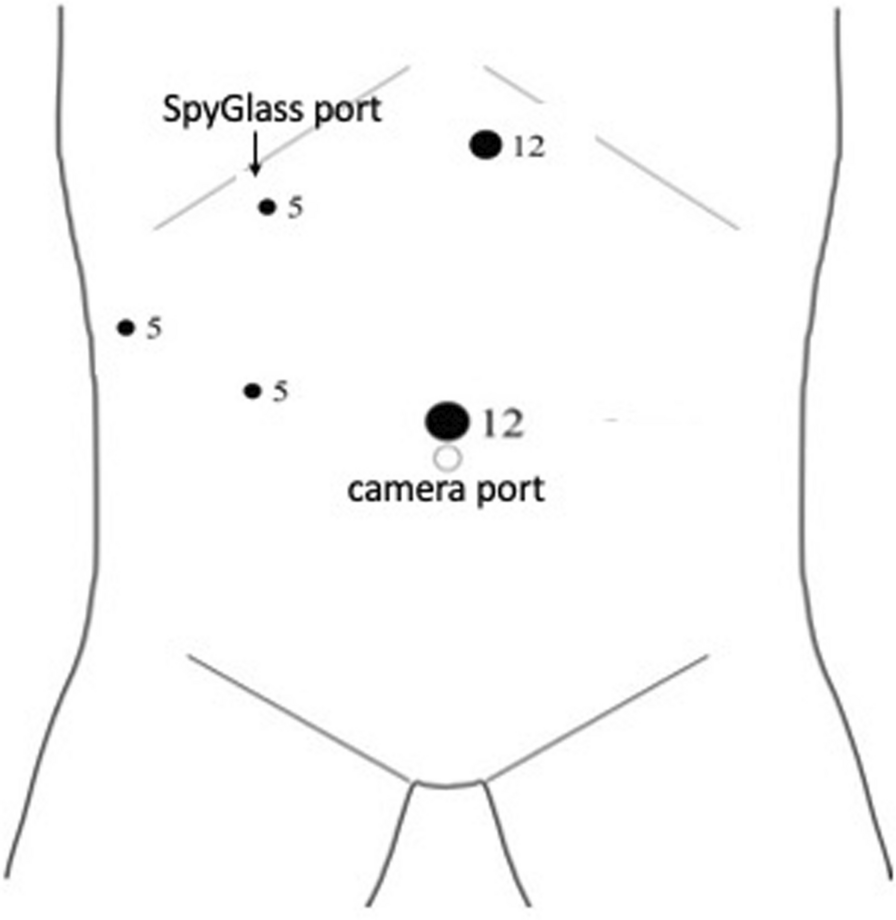
The role of laparoscopic surgery for emergency colorectal operations is still unclear. One recent comparison of open and laparoscopic cases demonstrated a twofold increase in anastomotic leaks in the latter group but similar overall postoperative morbidity [57]. Additional published results indicate that the laparoscopic approach is a suitable alternative to laparotomy in select cases by surgeons who are competent with this technique [34, 70,71,72].
Recommendation 6: For patients with successful endoscopic decompression, sigmoid colectomy should be offered to prevent recurrent volvulus. The colectomy should be performed as early as possible, even during the index admission. Grade of Recommendation: Strong recommendation based on low-quality evidence, 1C.
After colonoscopic detorsion followed by conservative management, the recurrence rate of sigmoid volvulus varies from 45 to 71% [21, 27, 49, 55,







留言 (0)