
Remember me


Older people with advanced serious illnesses have repeated unplanned early readmissions to acute care hospitals after discharge. Readmissions and overutilization drive over half of health care costs in the United States.1-3 Patients often share similar characteristics in the way they use services, such as long lengths of stay, frequent encounters with their primary providers, and frequent hospital readmissions.4,5 Other common characteristics include polypharmacy, multiple chronic comorbidities, and frailty traits.4,6-12 This takes a toll upon the physical and emotional reserves of the patient, leading to frailty and a loss of independence.4 These circumstances may affect one's Sense of Coherence and make it difficult to find comprehensibility, manageability, and meaningfulness at this time of their lives.
THEORETICAL FRAMEWORKAs one ages, there are expected losses. Loss of resources including friends and family due to death may lead to isolation.13Loss of the resources of health and agility leads to a loss of physical independence.14-16 The inability to drive may lead to further loss causing isolation and the loss of hobbies.16-18 These losses may compound the ability of seriously ill older people to cope effectively. Antonovsky refers to such resources as generalized resistance resources19,20
The concept of Sense of Coherence was the theoretical framework for this study. Sense of Coherence is a way of perceiving one's surroundings and environment as (1) structured and predictable, that one (2) has the resources to address the stressors one may confront and (3) possesses the belief that these stressors and challenges are worthwhile to overcome. Until now, sense of coherence20 was understood to be a mostly stable state after the age of 30.19,20
Sense of Coherence is a construct that is comprised of 3 concepts. The first is Comprehensibility, which is the extent to which one perceives stimuli as making cognitive sense and is ordered and structured, rather than arbitrary and disordered.19,20 The next is Manageability, which is the individual's perception that they have the resources required to thrive during times when difficulties are encountered.19,20 The third is Meaningfulness, which refers to how an individual feels that life makes sense emotionally and that difficulties met are worth the effort to enlist the effort to overcome19,20
Sense of Coherence has not been explored specifically as it pertains to the aging individual as they experience losses, which are natural as one ages and as one nears the end of life. The research question for this study was how do seriously ill, older adults maintain or reconstruct their Sense of Coherence in the presence of loss and illness as they near the end of life?
METHODS DesignInterpretive Description was selected to guide the design of this study.21 Interpretive description allows the flexibility needed in qualitative research when using an existing theory. This flexibility allows for a design with an eye toward real-world solutions that can be applied at the bedside by the clinician.21 The use of Interpretive Description allowed for the use of deductive questioning using a priori codes from the construct of sense of coherence.
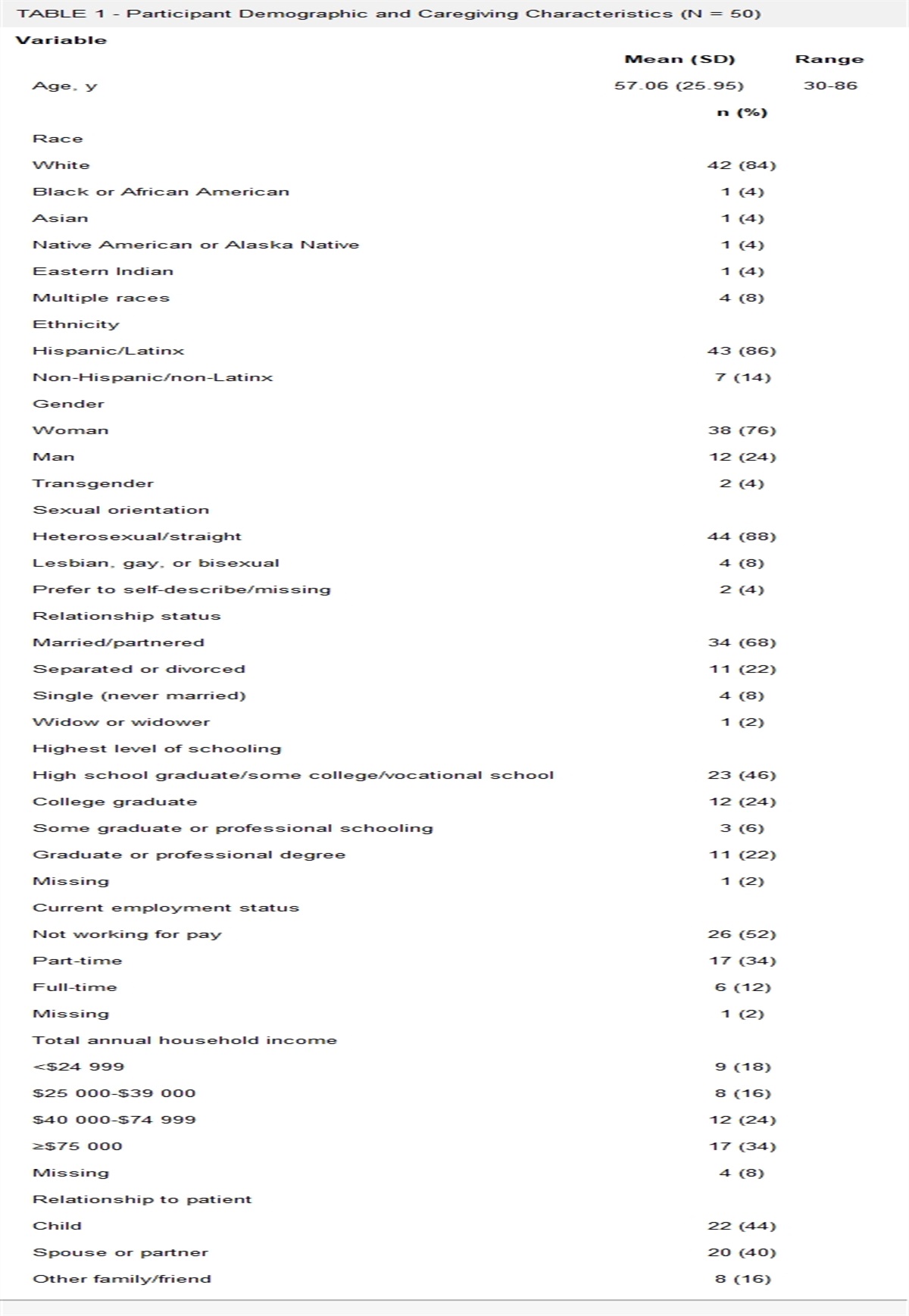
PopulationThe participants were older adults older than 65 years in an acute hospital during unplanned 30-day readmission who were English speaking (Table 1).
TABLE 1 - Inclusion and Exclusion Criteria Inclusion Criteria Exclusion Criteria 65 years of age or older Admitted on observational statusa Readmitted to the hospital within 30 days of their last hospital discharge Planned readmissions for interventions English speaking Possesses capacity as described in Human Research Protection Program Policy 340aThis refers to a person who returns to the hospital and is kept in the hospital for observation, rather than a formal readmission.
The exclusion criteria excluded patients admitted on observational status. Observational care is care provided in the hospital when the patient is not formally admitted and the stay is less than 2 midnights.22
SettingThis research was conducted in a large academic hospital in New England, United States.
Sample RecruitmentPotential participants were identified using a purposive approach. An analytics report was generated by the hospital's data analytics team using the inclusion criteria. Patients were informed of the study by hospital case managers and provided with an information sheet. If the patients agreed, the researcher visited the patient and explained the project. Informed consent was obtained from each willing participant.
Data CollectionData were collected through semistructured interviews. Once an interview was completed, it was transcribed. The transcriptions were uploaded to Atlas.ti for analysis and coding.
Data AnalysisDirected content analysis, also known as Deductive Category Application, was used to evaluate and interpret data.23 This approach allows for existing theory to direct a research question using a deductive tactic with the goal of conceptual expansion of a theoretical framework. Mayring's Model of Deductive Category Application was followed (Figure).23
 FIGURE: Mayring's model of deductive category application.23
FIGURE: Mayring's model of deductive category application.23The concepts derived from Sense of Coherence (Comprehensibility, Manageability, and Meaningfulness) were used as a priori codes and the theoretical framework19,20 This was followed by inductive, iterative coding searching for themes and patterns. Table 2 illustrates the organization of the codes. Synthesizing of the data and theorizing commenced in preparation for writing the interpretive description.21
TABLE 2 - Results of Deductive Analysis and Subsequent Inductive Analysis Overarching theme Comprehensibility Incomprehensibility Subthemes Directed communication comprehensibility Intuitive comprehensibility Directed communication incomprehensibility Intuitive incomprehensibility Associated codes Continuity of message Acceptance Big picture conversation: unclear Avoidance Big picture conversation Getting weaker/sicker Low health literacy Denial Intellect/education Insight Not understanding the limitations of medicine Lack of insightTwo ethical issues were addressed: (1) working with a vulnerable population24,25 and (2) determining capacity in this population.
Steps were taken to provide safeguards to protect participants by stopping interviews if the participant showed signs of fatigue or distress. Also, the participants were asked to interrupt the interview if they felt they were fatigued.
Capacity was assessed using the university's institutional review board's policy.
RESULTSThe purposive recruitment resulted in 25 participants. One person was excluded because of a lack of capacity. The demographic data of the participants are presented in Table 3. The data include age, sex, ethnicity, insurance coverage, and physical/medical characteristics.
TABLE 3 - Demographic Characteristics of the Sample Characteristics Result N Mean Median Range Age 75.3 75 65-95 Sex Female 13 Male 12 Ethnicity White 19 African descent 4 Asian 1 Latino/Hispanic 1 Insurance coverage Medicare only 7 Medicaid only 1 Dual coveragea 4 Medicare advantage 5 Medicare with private supplemental insurance 8 Physical/medical characteristics Frailty documented in chart 11 Number of comorbidities 3.34 3 0-10 Number of prescriptions 13.52 13 4-24aDual coverage is indicative of low socioeconomic status and provides the greatest access to health care in the United States.
In the context of Antonovsky's midlevel theory and model of Salutogenesis, the expected losses experienced by older people will be referred to as Serial Loss of Generalized Resistance Resources. During the study, it was realized that this is a new concept to be included in the nomenclature of Salutogenesis and is related to Sense of Coherence.
ComprehensibilityComprehensibility is an existing concept within the construct of Sense of Coherence. It was examined specifically within the context of older people who are facing Serial Loss of Generalized Resistance Resources, declining health, and nearing death. Comprehensibility affects the patient's ability to cope, access resources, and find meaning in their experience.
The following are associated with increased Comprehensibility:
An example of an exchange in this interview shows how important clear and consistent communication is to patients.
Olivia: I did not like the communication in X at all. I think it's much better here. When I was up on floor X it was great. I saw all kinds of people every day, and, um, you know, everybody had, you know, put in their two cents worth, but everybody's told me what…everybody seemed to be pretty much on the same, you know, there weren't a lot of, if any, discrepancies, and, um, I got very clear written information when I left.
Effective communication requires updates not only to the patient but between members of the health care team to enhance this participant's Comprehensibility.
The next example shows evidence of the understanding of circumstances related to a “big-picture conversation” he had sometime during the trajectory of his illness.
Edward: And unfortunately, I get these, between the congestive heart failure and these, you know, somebody along the line, a doctor somewhere, I give you a list of doctors I see, you won't believe it, said to me, you know, I'm in frail health. And I know I'm in frail health. I have been for a long time. So that makes me more susceptible, I think, to picking up things.
A “big-picture conversation” that includes a discussion of expectations, the risks and benefits of treatments, the prognosis, and the patient's personal goals is necessary to increase comprehensibility.
Within this text, there is an expression of gratitude for truth-telling from the provider.
Ursula: Really the more communication that we had was here, you know. That they really explain to you really clear what is going on. What I have, what I have to do and all that. There was things that I didn't even know. The doctor here is explaining to me a lot of thing really clearly… It makes a lot of difference…Communication between the doctor and patient is, it make a lot of difference because you expect that the doctor tells you really what's going on without no holding back. You know, and that's what happen, you know.
The heaviest burden in prognostic communication lies with the clinician. Equally important to Comprehensibility is the ability of the participant to process and understand the information.
This participant expressed her ability to perceive the physical changes she was experiencing, such as the decline in her function and strength.
Barbara: Well I've been sick since last April, you know with the pneumonia, I never really recovered from that, uh, I…I…I went to PT I uh went to the gym. I'm a gym person, and I thought I was doing very well and then I started getting tired again. All I wanted to do is rest. I couldn't wait to get into my favorite chair and fall asleep. And my husband started worrying about me, so we went to the doctor and he said “It's unusual for you to feel this way” so he said “I suggest you go to the hospital, get a complete work-up,” and that's what I did, called 911 went in and here I am, and then I went home thinking my husband could take care of me, and it was just too much, uh, he didn't say it (voice goes up) by I knew it.
Her insight helped her to understand that her health was waning and would not return. This participant died less than 48 hours after the interview.
This excerpt is an example of how one participant came to understand her circumstances.
Hannah: I keep telling myself, my children, it can happen any time, any day…I realize and I think mother died the way, heart…
Researcher: Did your doctor ever tell you that you could go at any time?
Hannah: No, never…that's what I realized.
This is an illustration of how one is able to obtain comprehensibility intuitively through past experiences of watching others' disease processes.
This is another excerpt from the previous interview. It reflects how a life review is pertinent through memory and the reality of the current situation.
Hannah: My husband died 22 years ago, June 20. He was born on December 20 and died on June 20, 74 years after. Good guy. Pianist. Had 2 diplomas. I loved it at night, summer night, he was sitting and playing and I in my nightgown going down my driveway…I had a long driveway…and the music come, just everybody are young at that time…you don't think forward what is going to happen.
The ability to accept one's circumstances allows for Comprehensibility. It provides an opportunity for planning, reflection and life review.
IncomprehensibilityIncomprehensibility is a new concept for sense of coherence in the context of older people at the end of their lives. This is a state in which the individual lacks an understanding of their prognosis and the ramifications on their circumstances in the environment of serious illness. This is detrimental to the individual's ability to plan and access necessary resources to help them cope and adapt to build a strong Sense of Coherence. These are examples of a lack of understanding due to poor communication resulting in Incomprehensibility.
This is an example of confusion regarding one's condition.
Ike: I started shaking all over in the middle of the night. I couldn't stop.
Interviewer: You couldn't stop? You started shaking in the middle of the night and you couldn't stop?
Ike:…And now I came back and I go downstairs and got over there and I just stood and shook again. Interviewer: Huh. What did they say was the problem?
Ike: They don't know.
This participant's medical record reflected that he had syncope and dehydration. The participant had a long history of heart disease, which included a myocardial infarction. There was no evidence of a big-picture conversation ever occurring between this participant and his providers. This is further evidence of the need for truth-telling and big-picture conversations.
This excerpt displays confusion or misunderstanding of circumstances and information that may be provided by the clinician.
Researcher: Why were you taking muscle relaxers?
Frank: Pain in my neck. I stopped taking one and um, that morning I 2 or 3 o'clock in the morning they told me I got up, the last I remember, I got up and I called my son, and the next thing I know I was in the hospital, and they said I had been in a coma for a couple of weeks, and um, they traced it back to this muscle relaxer. Evidently, it was the type of deal when you don't stop taking it all of a sudden, but nobody had said anything…I have been going downhill ever since.
Researcher: You had some other problems, didn't you?
Frank: No.
Researcher: What about your lungs?
Frank: That was all tied into that.
This patient had chronic obstructive pulmonary disease but appeared to find understanding his diagnosis challenging, although he stated it had been explained to him. Despite his records reflecting he had been told otherwise, he insisted that his chronic obstructive pulmonary disease was related to stopping his muscle relaxers and remained unaware of the disease process.
This is an example of how avoidance of a discussion of one's mortality (big picture conversation) prohibits Comprehensibility.
Researcher: What does this all mean to you?
Quincy: It means (chuckles) I don't know, I just try to do the best I can. Do you know what I mean?
Researcher: Does it make you think about your own mortality?
Quincy: No, not really.
Researcher: Not really?
Quincy: (angrily) No. No, it doesn't, no.
Quincy had the highest number of 30-day readmissions in 12 months and the greatest number of comorbidities. It was evident that there had been many discussions of his prognosis, but he avoided the topic in the interview. It seemed he used anger to avoid the topic of his mortality.
Other participants either were challenged by or did not understand the limitations of Western medicine or had unrealistic expectations for the outcomes of their conditions.
In this example, either misunderstanding or denial was a barrier to understanding, leading to Incomprehensibility.
Aaron: You know, you know…that's what I can't figure out…here I am at hospital X, and they can't figure out what I got going and it's because it's a combination of things. You know the liver, the ah, what's that thing called? Alcohol-related? Cirrhosis, that's right. Kidney. So they're trying to weigh everything all at the same time.
This participant was in multisystem failure and struggles to appreciate that there are some things that medicine cannot remedy regardless of how prestigious the doctors or hospital. His medical records reflected that he had several big-picture conversations but was unable to understand or accept that nothing could be done about his multisystem failure.
Aaron's situation was rich in data. Aaron continued to describe and question his situation.
Aaron: Well there were a lot of things in play when I came here because I thought it was strictly a, um, gallbladder issue and they found all sorts of different problems with the liver, kidneys a “bacriol” that goes through my blood…A bacteria, yeah. It goes through my blood, and they're working on all of it. As of today, all of the vitals, as of this morning all of my vital signs are perfect, including my liver, including my kidneys, everything except for…they're still trying to figure out that last piece of the puzzle to be able to complete the process.
Interviewer: And what piece of the puzzle is that?
Aaron: The gallbladder.
According to his nurse, all the correct information had been relayed to him that morning. This may have been an issue of lack of awareness by the providers of how to speak with very sick people or perhaps a state of denial.26
It is difficult to say if Aaron was confused or in denial. Denial is another way that participants exhibit incomprehensibility. The realities of disease progression make facing these stimuli difficult, but ultimately, inevitable. In some cases, denial is a protective mechanism. In others, denial may hinder the individual from acceptance and create an impediment to planning and reconciliation at the end of life.
Continuing with Aaron, this excerpt is a description of Aaron's last day of work.
Aaron: So, I was home for a week, and then my regular…I went to work on Monday and uh, they called my wife and said “Come pick your husband up, he's not driving home” ‘cause they could see I was sick and didn't have the enthusiasm or voice that I had going in there. So, they did that and I and went back Tuesday and they said we have to put you on a leave of absence for medical until your better and come back. Whenever you're ready to come back you've got a job.
It appears Aaron could not read between the lines of what his employers found evident. It seems he was unable to gauge his abilities through his physical senses. Everyone around this participant recognized that he is seriously ill, but it appears the patient may not have had the insight to recognize his circumstances. This participant died during that hospital admission.
EXISTING LITERATUREThere is little in the literature specific to end-of-life and Sense of Coherence. That contained in the literature presently concerns itself with caregivers of terminally ill people.27-29 There is room for further research and development of Antonovsky's theory.30 Antonovsky had just begun contemplating the subject, which he presented in a speech at the University of California at Berkeley shortly before he died, but his ideas were in their genesis regarding end of life for older people.31 A few years later, Erikson republished his original work with a ninth chapter included for the “final phase of life.”32 Erikson's work echoed much of what Antonovsky opined and he adopted Sense of Coherence as a point of theorizing. Erikson wrote about the importance of integrity at the end of life. His work is theoretical with little practical application or intervention, but theories are a jump-off point to all understanding and lend themselves to many research opportunities.
Antonovsky's and Erikson's works, as well as the findings of this study, validate the need for further investigation of Sense of Coherence and serial loss of general resistance resources at end of life as a unique life phase independent of other stages in life. This study is a start in such work. With further research, we will learn how to better intervene to make difficult times more manageable for older adults dying in a society with death anxiety, death denial, and unrealistic expectations of Western Medicine.
Regarding Serial Loss of Generalized Resistance Resources, similar ideas have been discussed in other literature; however, the phenomenon has not been given a name.33-35 This research has led to the labeling of this phenomenon.
RECOMMENDATIONSInterventions can be developed to help these patients strengthen their comprehensibility and Sense of Coherence. Before interventions can be implemented, there will need to be further studies on Serial Losses of Generalized Resistance Resources. In addition, the clinician will be required to have the skills to recognize patients as they begin to enter this phase of life. This will require the development of tools that could be used to help identify those who are at risk. It is recommended that this should be presented to palliative care and geriatric fellows to begin disseminating knowledge.
Interventions resulting from this study's findings may increase Comprehensibility through education on the relationship between Serial Loss of Generalized Resistance Resources, and overtreatment,36-38 and the importance of excellent communication by the clinician.39-41 With this knowledge, the clinician potentially holds the key to contributing to a stronger Sense of Coherence and a more healthful dying process by freeing the patient from the confusion caused by Incomprehensibility.
Conclusion/DiscussionAntonovsky's and Erikson's works, as well as the findings of this study, validate the need for further investigation of Sense of Coherence and Serial Loss of Generalized Resistance Resources at the end of life as a unique life phase independent of other stages in life. This study is a start in such work. With further research, we will learn how to better intervene to make difficult times more manageable for older adults dying in a society wrought with death anxiety, death denial, and unrealistic expectations of Western medicine.
This research resulted in 2 new concepts contributing to Antonovsky's theoretical construct of Sense of Coherence and the midlevel theory of Salutogenesis.19,20 These concepts are Incomprehensibilty and Serial Loss of Generalized Resistance Resources. These findings suggest that Sense of Coherence is a more dynamic state than previously believed, especially in older adults with serious illnesses. Sense of Coherence was believed to be a mostly stable state once an individual reached the age of 30 years.20 The strength of one's Sense of Coherence was based upon the quality of General Resistance Resources, which is a myriad of resources including relationships, physical ability, knowledge, and many other characteristics.
Unfortunately, Antonovsky did not consider permanent changes in Generalized Resistance Resources that are expected to occur as one ages and nears the end of life. Through this research, this phenomenon was identified and is a new concept, that being Serial Loss of Generalized Resistance Resources. In the presence of serious illness, the loss of spouses and friends to death, physical agility, independence, and impending death, it is very unlikely that the individual will be able to regain these resources, and the losses are permanent and progressive.
Incomprehensibility is the counterpart of Comprehensibility. Incomprehensibility refers to the lack of understanding of one's prognosis, limitations, and the fact that they are on a trajectory of ever-increasing loss and ill health that will result in their death. To this date, this concept can be applied only to this specific population studied until further research is completed.
Incomprehensibility is a result of varying factors. It can result from the avoidance and denial of information provided by their clinician. It can be a result of a lack of health literacy. The most detrimental factor leading to Incomprehensibility is the failure of clinicians to provide the essential information and/or not evaluate for understanding required to make sure their patient is informed.
The responsibility of this intervention is the propriety of the clinician, as well as the evaluation to determine whether the patient has achieved understanding.
When a patient suffers Incomprehensibility in the environment of serial loss of general resistance resources, the result is often chaos. Although Serial Loss of Generalized Resistance Resources is anticipated to continue, not fully understanding their circumstances and prognosis may impede the ability of the individual to draw on remaining existing resources and plan for a meaningful death. What makes serial loss of general resistance resources unlike other losses is that these losses occur when there is no time to recuperate and replace these resources as they are so near end of life.
Truth told by a clinician has further implications for our patients than one merely understanding that they are near the end of life. Truth-telling, in and of itself, may allow an individual to understand that time is limited and recognize the importance of engaging in life review, reconciliation, garnering existing resources, and acquiring a deeper meaning of their own mortality. This is the essence of Sense of Coherence for people at this stage of life.
References 1. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA. 2018;319(10):1024–1039. doi:10.1001/jama.2018.1150. 2. Agency for Healthcare Research and Quality. Health Care Cost and Utilization Project. U.S. Department of Health and Human Services. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb278-Conditions-Frequent-Readmissions-By-Payer-2018.jsp. Accessed January 9, 2023. 3. Sisko AM, Keehan SP, Poisal JA, et al. National health expenditure projections, 2018-27: economic and demographic trends drive spending and enrollment growth. Health Aff. 2019;38(3):491–501. 4. Author. Learning How Older People Form Sense of Coherence through an Interpretation of Their Experiences of Decline and Serious Illness During a 30-Day Readmission: An Interpretive Description. Lancashire, UK: Lancaster University. 5. Glans M, Kragh Ekstam A, Jakobsson U, Bondesson Å, Midlöv P. Risk factors for hospital readmission in older adults within 30 days of discharge—a comparative retrospective study. BMC Geriatr. 2020;20(1):467. 6. Lin Y, Yang C, Chu H, et al. Association between the Charlson Comorbidity Index and the risk of 30-day unplanned readmission in patients receiving maintenance dialysis. BMC Nephrol. 2019;20(1):363. 7. Iyengar A, Goel N, Kelly JJ, et al. Effects of frailty on outcomes and 30-day readmissions after surgical mitral valve replacement. Ann Thorac Surg. 2020;109(4):1120–1126. 8. Rafiq M, Keel G, Mazzocato P, Spaak J, Savage C, Guttmann C. Deep Learning Architectures for Vector Representations of Patients and Exploring Predictors of 30-Day Hospital Readmissions in Patients With Multiple Chronic Conditions. Berlin: Springer; 2019:228–244. 9. Elsamadicy AA, Freedman IG, Koo AB, et al. Modified-frailty index does not independently predict complications, hospital length of stay or 30-day readmission rates following posterior lumbar decompression and fusion for spondylolisthesis. Spine J. 2021;21(11):1812–1821. 10. Thorell K, Midlöv P, Fastbom J, Halling A. Use of potentially inappropriate medication and polypharmacy in older adults: a repeated cross-sectional study. BMC Geriatr. 2020;20(1):73. 11. Nwadiugwu MC. Frailty and the risk of polypharmacy in the older person: enabling and preventative approaches. J Aging Res. 2020;2020:1–6. 12. Pazan F, Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. 2021;12:443–452. 13. Lekalakala-Mokgele E. Death and dying: elderly persons' experiences of grief over the loss of family members. S Afr Fam Pract. 2018;60(5):151–154. 14. Padilla Colón CJ, Molina-Vicenty IL, Frontera-Rodríguez M, et al. Muscle and bone mass loss in the elderly population: advances in diagnosis and treatment. J Biomed (Syd). 2018;3:40–49. 15. El Abd A, Schwab C, Clementz A, Fernandez C, Hindlet P. Safety of elderly fallers: identifying associated risk factors for 30-day unplanned readmissions using a clinical data warehouse. J Patient Saf. 2022;18(3):230–236. 16. National Academies of Sciences E, Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System. Washington, DC: National Academies Press; 2020. 17. Qin W, Xiang X, Taylor H. Driving cessation and social isolation in older adults. J Aging Health. 2020;32(9):962–971. 18. Lamanna M, Klinger CA, Liu A, Mirza RM. The association between public transportation and social isolation in older adults: a scoping review of the literature. Can J Aging. 2020;39(3):393–405. 19. Antonovsky A. Health, Stress, and Coping. San Francisco: Jossey-Bass; 1979. 20. Antonovsky A. Unraveling the Mystery of Health. San Francisco: Jossey-Bass Publishers; 1987. The Jossey-Bass Health Series. 21. Thorne S. Interpretive Description: Qualitative Research for Applied Practice. 2nd ed. Philadelphia: Routledge; 2016. 23. Mayring P. Qualitative content analysis. Forum Qual Soc Res. 2000;1(2). 24. Gómez A, Padrós M, Ríos O, Mara LC, Pukepuke T. Reaching Social Impact Through Communicative Methodology. Researching With Rather Than on Vulnerable Populations: The Roma Case. Madrid: Frontiers Media SA; 2019:9. 25. De Chesnay M, Anderson B. Caring for the Vulnerable. Burlington, MA: Jones & Bartlett Learning; 2019. 26. Cassell EJ, Leon AC, Kaufman SG. Preliminary evidence of impaired thinking in sick patients. Ann Intern Med. 2001;134(12):1120–1123. 27. del-Pino-Casado R, Espinosa-Medina A, López-Martínez C, Orgeta V. Sense of coherence, burden and mental health in caregiving: a systematic review and meta-analysis. J Affect Disord. 2019;242:14–21. 28. Waldrop DP, McGinley JM. “I want to go home”: how location at death influences caregiver well-being in bereavement. Palliat Support Care. 2020;18(6):691–698. 29. Villaseñor T, Perrin PB, Donovan EK, et al. Parkinson's family dynamics and caregiver sense of coherence: a family-systems approach to coping in Mexico and the United States. Aging Med (Milton). 2020;3(4):252–259. 30. Hochwälder J. Sense of coherence: notes on some challenges for future research. SAGE Open. 2019;9(2):2158244019846687. 31. Antonovsky A. The salutogenic approach to aging. Lecture held in Berkeley. 1993:981–982. 32. Erikson EH, Erikson JM. The Life Cycle Completed: Extended Version. New York, NY: W.W. Norton & Co.; 1998. 33. Escourrou E, Herault M, Gdoura S, Stillmunkés A, Oustric S, Chicoulaa B. Becoming frail: a major turning point in patients' life course. Fam Pract. 2019;36(2):231–236. 34. Gitterman A, Knight C. Non-death loss: grieving for the loss of familiar place and for precious time and associated opportunities. Clin Soc Work J. 2019;47(2):147–155. 35. Perissinotto C, Holt-Lunstad J, Periyakoil VS, Covinsky KE. A practical approach to assessing and mitigating loneliness and isolation in older adults. J Am Geriatr Soc. 2019;67(4):657–662. 36. Heppner HJ, Haitham H. Intensive care of geriatric patients—a thin line between under- and overtreatment. Wien Med Wochenschr. 2022;172(5-6):102–108. 37. Hay CM, Donovan HS, Campbell GB, Taylor SE, Wang L, Courtney-Brooks M. Chemotherapy in older adult gynecologic oncology patients: can a phenotypic frailty score predict tolerance? Gynecol Oncol. 2019;152(2):304–309. 38. Szilcz M, Wastesson JW, Morin L, Calderón-Larrañaga A, Lambe M, Johnell K. Potential overtreatment in end-of-life care in adults 65 years or older dying from cancer: applying quality indicators on nationwide registries. Acta Oncol. 2022;61(12):1437–1445. 39. Anderson RJ, Bloch S, Armstrong M, Stone PC, Low JT. Communication between healthcare professionals and relatives of patients approaching the end-of-life: a systematic review of qualitative evidence. Palliat Med. 2019;33(8):926–941. 40. Lee RY, Brumback LC, Sathitratanacheewin S, et al. Association of physician orders for life-sustaining treatment with ICU admission among patients hospitalized near the end of life. JAMA. 2020;323(10):950–960. 41. Scheunemann LP, Ernecoff NC, Buddadhumaruk P, et al. Clinician-family communication about patients' values and preferences in intensive care units. JAMA Intern Med. 2019;179(5):676–684.
Comments (0)