1. IntroductionExtended-spectrum β-lactamases producing Enterobacterales (ESBL-PE) are a severe threat to hospitalized patients [
1]. The carriage of ESBL-PE is diagnosed in 2 to 49% of patients during an intensive care unit (ICU) stay [
2,
3,
4]. During hospitalization, patients can acquire ESBL-PE due to cross-transmission from colonized to non-colonized patients and/or in relation to antibiotic pressure [
5,
6,
7]. The consequences of ICU-acquired ESBL-PE for patient outcomes remain controversial. Some studies have shown that ICU-acquired ESBL-PE carriage is associated with high mortality, excessive ICU and hospital length of stay (LOS), and high hospital costs [
8,
9,
10].During the COVID-19 pandemic, hygiene measures were significantly strengthened, mainly contact and respiratory precautions. In this context, bacterial cross-transmission was thought to be at its lowest level. However, several studies showed an increased prevalence of ESBL-PE during the pandemic [
11]. This may have resulted from antibiotic pressure, since early in the pandemic antibiotics were widely overused [
12,
13]. This suggests that the misuse of antibiotics was a pivotal contributor to resistance development during this period.Indeed, based on the high coinfection rate observed during other coronaviruses and H1N1 pandemics [
14,
15,
16], antibiotics were systematically used upon admission to ICU [
17,
18]. In French Guiana, empiric antibiotic treatment was chosen according to the most frequently isolated pathogens in community-acquired pneumonia and the circulating microorganisms in the region, mainly Coxiella burnetti and Leptospira spp. [
19]. Therefore, in French Guiana, cefotaxime was empirically used alone or in combination with levofloxacin. Later, bacterial coinfection was documented only in a few cases, and antibiotics were no longer systematically recommended [
12,
20,
21,
22,
23].
This study aimed to assess the impact of antibiotic prescription on the acquisition of extended-spectrum β-lactamase producing Enterobacterales in ICUs during the COVID-19 crisis.
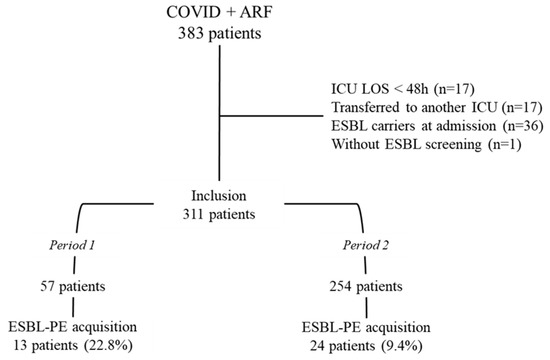
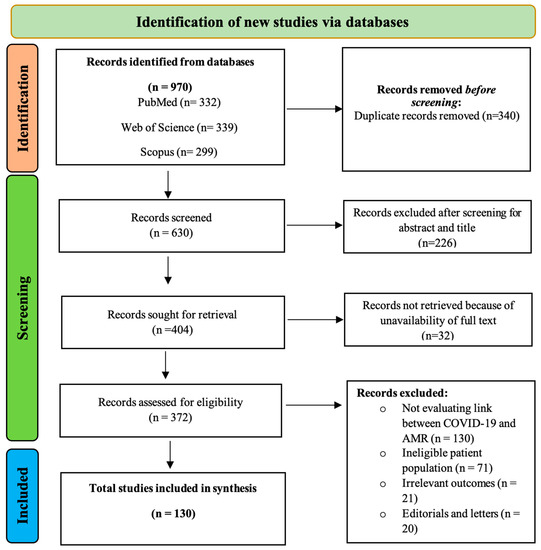
2. ResultsDuring the study period, 383 patients were admitted to the ICU for COVID-19 and respiratory failure, and 311 (81.2%) met the inclusion criteria. Fifty-seven patients were admitted in Period 1 (18.3%) and 254 in Period 2 (81.7%) (
Figure 1). The median age was 63 years (53–71), the male patients were 159 (51.1%), and the median SAPS II score was 29 (24–35). The main registered comorbidities were diabetes mellitus (40.8%) and arterial hypertension (62.1%). The main observed organ failures were respiratory (100%) and renal failure 48 (15.4%).ICU-acquired ESBL-PE carriage was diagnosed in 37 patients (11.9%). This prevalence was 22.8% during Period 1 (13/57 patients) and 9.4% during Period 2 (24/254 patients) (p = 0.005). Antibiotics were prescribed before the ESBL-PE acquisition in 56 patients (98.2%) during Period 1 and 99 patients (39%) during Period 2. The median time from admission to ESBL-PE carriage (in carriers) or to discharge (in non-carriers) was 14 days (10–20). It was 17 days (9–32) in Period 1 and 14 (10–20) in Period 2 (p = 0.460). The main isolated ESBL-PE was Klebsiella pneumoniae (84.6% in Period 1 and 58.3% in Period 2).
Table 1 shows the epidemiologic and clinical parameters recorded upon ICU admission in the whole population and in ESBL-PE carriers and non-carriers.
Table 2 shows the isolated ESBL-PE strains.During the ICU stay, 139 patients (44.7%) received invasive mechanical ventilation (MV). They were 32/37 (86.5%) and 107/274 (39.1%) in ESBL-PE carriers and non-carriers, respectively (pppppp = 0.014) (
Table 3).Nine relevant variables were included in the multivariate analysis to identify independent factors associated with ESBL-PE acquisition in ICU. They were the SAPS II score, renal failure, catecholamine use, MV, and antibiotics prescription prior to ESBL-PE carriage (amoxicillin clavulanate, cefotaxime, piperacillin tazobactam, cefepime, carbapenems). Of these, exposure to cefotaxime was the only factor independently associated with ESBL-PE carriage (p = 0.002, IRR 2.59 [95% IC 1.42–4.75]) (
Table 4). When using propensity score matching estimates, the treatment effect (the increased risk) for cefotaxime was 0.096 (95% CI = 0.02–0.17), p = 0.01.
We compared patients receiving cefotaxime (115 patients) and patients who did not receive any antibiotic (156 patients) prior to ESBL-PE carriage. The prevalence of ESBL-PE carriage was 25/115 (21.7%) in patients exposed to cefotaxime and 7/156 (4.5%) in those not exposed to antibiotics. The absolute risk difference for acquiring ESBL-PE in the ICU in patients exposed to cefotaxime was 17.2%. The relative risk for acquiring ESBL-PE in the ICU in patients exposed to cefotaxime was 3.8. The number of patients we needed to expose to cefotaxime in order to observe one additional ESBL-PE acquisition in the ICU was 6.
3. DiscussionESBL-PE carriage is a major concern in intensive care facilities [
24]. In a previous study conducted in our unit, it was found in 27.6% of patients and was acquired during the ICU stay in 19.6% [
25]. Additionally, the proportion of patients carrying ESBL-PE who developed ICU-AI to the same microorganism was 51.2% in ESBL-P K. pneumoniae, and 40% in ESBL-P Enterobacter spp. [
25]. Due to this high rate of ESBL-PE carriage, we continue screening patients upon admission and weekly during the ICU stay [
26]. In the present study, the prevalence of ESBL-PE acquisition was 22.8% during the first period, higher than that observed in the previous study from our unit [
25] and 9.2% during the second period. This is probably due to the impact of antibiotics pressure on the ESBL-PE epidemiology.The emergence of multidrug-resistant organisms and their spread across healthcare settings are caused by multiple factors, including antibiotics use and cross-transmission due to gaps in infection control. During the COVID-19 pandemic, infection control and hygiene measures were drastically upgraded. In this context, the risk of bacterial cross-transmission was thought unlikely to occur. However, massive dissemination of resistant bacteria was observed in some ICUs [
27]. This was explained by the increased workload, the heaviness of the care in particular, the need to change positions (prone and supine position), and the use of replacement professionals less or not qualified to compensate for absences and resignations. In addition, the global situation has been responsible for a shortage of personal protective equipment and hydroalcoholic solutions in connection with production and delivery issues [
28,
29]. In the study by Emeraud et al. [
28], the dissemination of multidrug-resistant bacteria was stopped quickly after correcting these factors. In French Guiana, the epidemic started 5 months after Europe, leaving time to prepare. In addition, comparatively the epidemic peak occurred later, 5 weeks after the first admissions, whereas in Europe it was reached in just one week. Thus, we benefited from the necessary time to supply and hire qualified health professionals. Additionally, we recruited healthcare workers from mainland France, Martinique, and Guadeloupe who were familiar with the intensive care context and infection control measures and who had already participated in managing COVID-19 patients in their home ICU. In this context, the infection control measures were respected, especially that the hygiene team of our hospital performed regular supervision and training in compliance with protective measures. Accordingly, our study is a quasi-experimental investigation where the ESBL-PE acquisition caused by cross-transmission is unlikely to occur. Consequently, it reflects the specific role of antibiotics consumption in the acquisition of ESBL-PE carriage in ICUs.At the beginning of the COVID-19 crisis, the worldwide scenario was the empirical use of antibiotics in about 90% of COVID-19 patients mainly in the ICU [
30,
31,
32]. In this context, an estimated 25–50% of antimicrobials prescribed in hospitals were considered unnecessary or inappropriate, directly impacting antimicrobial resistance [
33]. A review by Al-Hadidi et al. highlighted that during the COVID-19 pandemic, 75% of adults with comorbidities received an antimicrobial without pathogen isolation and the antibiotics used were inappropriate in more than one-third of cases [
15]. Indeed, empirical antibiotics prescription was based on the high coinfection rate observed during previous coronaviruses and the H1N1 epidemic and on the recommendations published at the beginning of the pandemic [
14,
16]. In French Guiana, the antibiotic strategy was based on the systematic use of cefotaxime alone or in combination with levofloxacin in severe COVID-19 patients. This policy evolved with the better knowledge of the disease [
12,
20,
21,
22,
23]. Our study investigated the antibiotic exposure before ESBL-PE acquisition and during the whole ICU stay in non-ESBL-PE carriers. Overall, half of the patients received antibiotics. They were 81% in ESBL-PE carriers and 46% in non-carriers. In addition, prior exposure to cefotaxime was independently associated with the acquisition of ESBL-PE carriage in ICUs. However, levofloxacin use was not included in the multivariate analysis model because it was regularly associated with cefotaxime when prescribed. Our results are similar to other studies reporting third-generation cephalosporins (3GC) as an independent factor associated with ESBL-PE acquisition. Moreover, the restricted use of 3GCs resulted in a significant decrease in the acquisition of ESBL-PE carriage [
34,
35,
36]. However, our study is quasi-experimental with two distinct periods (with and without systemic empiric antibiotic prescription) in a context of reinforced hygiene measures and a homogenous studied population regarding the first diagnosis (acute respiratory failure in COVID-19 patients) and the baseline patient’s characteristics. This model accurately identifies the closest weight to reality of the impact of antibiotics use on the ESBL-PE carriage epidemiology in ICUs.
This study has potential limitations. First, this is a monocentric study. However, our unit accounted for 80% of ICU beds in French Guiana. For this, it gives an accurate picture of ESBL-PE acquisition in ICU in French Guiana during the COVID-19 crisis. Second, the microbiological identification was phenotypic without genotypic identification. Nevertheless, this is an epidemiological study investigating the ESBL-PE carriage independently of the responsible enzyme.
4. Materials and Methods 4.1. Setting and Patients
Our study was prospective and observational. It was conducted over 19 months, from 1 April 2020, to 31 December 2021, in the medical-surgical intensive care unit of the Cayenne General Hospital in French Guiana.
We included patients older than 18 admitted to the ICU for respiratory failure with positive SARS-CoV-2 screening. A positive screening of SARS-CoV-2 was assessed through positive real-time polymerase chain reaction (RT-PCR) testing on nasopharyngeal swab samples or endotracheal aspirates. We excluded all patients transferred from another ICU, those with an intensive care length of stay shorter than 48 h, those who were ESBL-PE carriers on admission, and those who had not been screened for ESBL-PE carriage.
Our hospital has a capacity of 500 to 600 beds and serves as a referral center for almost 300,000 inhabitants from all of French Guiana [
37]. Our ICU works according to European and French standards with a 1:2 nurse-to-patient ratio. All patients have dedicated equipment for care and monitoring. Hand hygiene is based on alcohol hand rub (at room entrance and exit, and between each distinct procedure of care) and the use of single-use gloves during nursing. Additionally, medical and non-medical staff wear single-use gowns when entering the patient’s room.
During the first wave, the protocol to manage COVID-19 patients with severe respiratory symptoms included systematic antimicrobial therapy with cefotaxime alone or in combination with levofloxacin, prescribed upon admission to the ICU. Since September 2020, we changed the protocol and antibiotics were no longer systematically prescribed and were reserved only for documented infections. According to this protocol change, we defined two periods in this study. Period 1 refers to routine, empiric antibiotics use, and Period 2 refers to the period where antibiotics were not prescribed systematically.
ESBL-PE carriage was routinely screened using rectal swabbing upon ICU admission and weekly afterward during the ICU stay (1 swab/patient/week—every Monday). Rectal samples were performed using Transystem™ (Copan Italia spa, Brescia Italy). Rectal swabs were plated on ChromID® ESBL agar (bioMérieux, Marcy-l’Etoile, France) and incubated for 48 h at 37 °C under aerobic conditions. Strains were identified using mass spectrometry (Maldi Biotyper, Bruker, Wissenbourg, France). Antibiotic susceptibility and the ESBL-E phenotype were determined through disk diffusion and interpreted according to EUCAST (
www.eucast.org, accessed on 26 November 2019). ESBL production was confirmed by the double-disk diffusion method using ceftazidime or cefotaxime with clavulanic acid [
38]. ESBL-PE carriage was defined as the isolation of ESBL-PE from surveillance or clinical culture. ESBL-PE isolated 7 days after admission in patients with previous negative specimens were considered ICU-acquired [
39]. Enterobacter spp. included Enterobacter cloacae, Klebsiella aerogenes, and Enterobacter asburiae. 4.2. Data Collection and DefinitionsThe data were recorded in an MS Excel spreadsheet using the hospital’s electronic health care systems. The main outcome was the ICU-acquired ESBL-PE carriage. The following parameters were prospectively collected: gender, age, BMI score, simplified acute physiology score (SAPS II) [
40], organ failure based on SOFA score (defined as an acute change in total SOFA score ≥ 2 points) [
41], and comorbidities (i.e., obesity, hypertension, diabetes, etc.). We also recorded data regarding the management and outcome such as the maximal respiratory support (high-flow nasal cannula (HFNC), non-invasive mechanical ventilation (NIV), and invasive mechanical ventilation (MV)), need for vasopressors, and renal replacement therapy (RRT), ICU-acquired infection (ICU-AI), ICU and hospital LOS and mortality. ICU-AIs were defined according to the International Sepsis Forum consensus conference [
42]. Ventilator-associated pneumonia (VAP) was defined as pneumonia occurring in patients under MV for more than 48 h [
43]. In our study, only the first episode of positive ESBL-PE sampling was studied. 4.3. Statistical AnalysisThe results were reported as the number of patients in whom the data were recorded (Nb), the median and inter-quartile range (IQR:1st–3rd quartiles), or numbers with percentages. Initial bivariate statistical comparisons for categorical variables were conducted using the Chi-square or Fisher’s exact tests. Continuous variables were compared using the Mann–Whitney U-test. Because the design was prospective and because logistic regression computes odds ratios, which for highly prevalent variables overestimates relative risks, we used a generalized linear model (GLM) with a Poisson family and a log link and robust error variance to identify patients’ characteristics associated with ESBL-PE acquisition in ICU [
44]. Non-redundant variables selected through bivariate analysis (p ≤ 0.05) and considered clinically relevant were entered into the GLM model. Measures of association are expressed as incidence rate ratios with 95% confidence intervals (CI). Furthermore, treatment effects were computed using propensity score matching using STATA 16 treatment effects command (STATA corporation, College Station, TX, USA).The absolute risk difference (ARD) of acquiring ESBL-PE in the ICU was defined as the difference between the event rate between the two groups exposed and not exposed to antibiotics. The relative risk of acquiring ESBL-PE in the ICU was defined as the ARD divided by the event rate in the group without antibiotics exposure. The number needed to treat (NNT) or the number of patients we needed to expose to antibiotics in order to observe one additional ESBL-PE acquisition in ICU was calculated as the inverse of the risk difference (NNT = 1/ARD) [
45]. All statistical tests were two-tailed, and p ≤ 0.05 was considered significant.
Statistical analyses were carried out with Excel (2010 Microsoft Corporation, Redmond, DC, USA), IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, NY, USA), and STATA 16, Stata Corporation, College Station, TX, USA.

留言 (0)