1. IntroductionCrohn’s disease and ulcerative colitis (UC), collectively known as inflammatory bowel disease (IBD), are characterized by chronic inflammation of the intestinal wall and follow a relapsing clinical course [
1,
2]. Anemia is the most frequent extraintestinal systemic complication in patients with IBD [
3,
4]. The reported data on the prevalence of anemia in these patients vary from 6% to 74% depending on the population studied [
5]. A systematic review of anemia prevalence in IBD patients in European countries showed an average of 27% and 21% in Crohn’s disease and UC, respectively [
5]. Anemia has a serious negative impact on quality of life and can lead to cognitive dysfunction and reduced exercise capacity [
6]. In severe cases, anemia is associated with extreme fatigue, dyspnea at rest, and heart failure caused by volume overload [
7]. Importantly, the presence of anemia in patients with IBD can predict an increased risk for hospitalization and even increased mortality [
8].The mechanisms of anemia in IBD are diverse. The majority of studies indicate that the leading type of anemia in IBD patients is iron deficiency anemia (IDA), affecting 36% to 90% of patients with Crohn’s disease [
9]. The causes of true iron deficiency in IBD include chronic blood loss, decreased iron intake, and reduced iron absorption due to drug side effects or duodenal involvement [
10,
11]. The second most common form of anemia in this patient cohort is anemia of chronic disease or anemia of inflammation (AI), driven by elevated blood concentrations of proinflammatory cytokines causing hepcidin-mediated iron sequestration in macrophages, inhibition of erythropoiesis in the bone marrow, suppression of erythropoietin production, and enhanced erythrophagocytosis [
12]. The unique characteristic of anemia in IBD is that IDA and AI can coexist in a significant proportion of patients, providing variable contribution to the net decrease in hemoglobin level. This poses a diagnostic challenge because the main laboratory parameters, such as transferrin and ferritin levels, are changed in IDA and AI in opposite directions. The situation is further complicated by the presence of other reported causative factors for anemia in IBD patients, including impaired absorption of vitamin B12/folic acid, hemolysis, myelodysplastic syndrome, and inhibition of erythropoiesis by immunosuppressive drugs [
3].Apart from anemia, undernutrition is a well-recognized extraintestinal systemic manifestation of IBD. Undernutrition is currently diagnosed as a gastrointestinal disorder according to one of the existing definitions [
13,
14]. The most recent international consensus on undernutrition diagnosis (Global Leadership Initiative on Malnutrition, GLIM) is based on phenotypic and etiologic criteria [
15]. Phenotypic criteria include weight loss (%) and low body mass index (BMI), while etiologic criteria include reduced food intake (or assimilation) and the presence of inflammation. Reduced food intake, malabsorption, and predominance of catabolic processes due to hypercytokinemia are key mechanisms of undernutrition in IBD [
16]. Historically, severe protein-energy malnutrition has been considered an etiological factor for anemia [
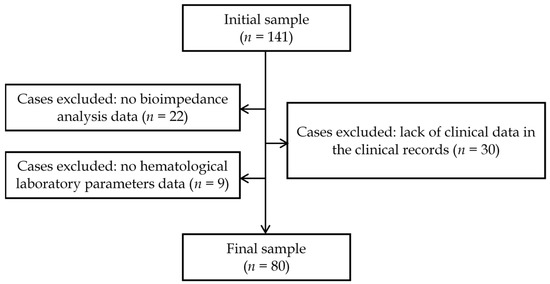
17]. Indeed, certain aspects of undernutrition, such as accelerated catabolism, sarcopenia, and hypoproteinemia, could contribute to anemia development by decreasing the availability of free amino acids for globin chain synthesis in erythroid progenitor cells. To the best of the researchers’ knowledge, the role of undernutrition in the genesis of anemia in patients with IBD has not been previously studied. Therefore, the relationship between undernutrition and anemia in patients with UC was investigated in a cross-sectional retrospective study. 3. ResultsA total of 80 patients with UC were included in the final analysis, and their baseline clinical characteristics are shown in
Table 1. The majority of patients were men (63.7%), 86.3% of the patients were admitted to the hospital with acute disease (S1–S3 disease behavior), and only 13.8% were in the remission phase of UC (S0 disease behavior). Half had pancolitis, while the others had left-sided colitis and proctitis. The prevalence of anemia in the sample population was 40.0%, and its prevalence across nutritional, demographic, disease-associated, and laboratory characteristics is presented in
Table 2.
In the bivariate analysis results, there was a significant association between anemia occurrence and total serum protein levels < 64 g/L (p = 0.009). The associations between BMI < 18.5 kg/m2, low body fat percentage, and anemia in crude analysis were non-significant.
The results of the binary logistic regression analysis are presented in
Table 3. Two binary logistic models were used in this study. Model 1 included BMI-level binary variables and total serum protein level binary variables as the main independent variables and others as covariates. In Model 2, BMI was replaced by a fat mass level binary variable (low body fat percentage).
In Model 1, variation in anemia across the total serum protein background remained at a significant level after adjustment for covariates. The variation in Model 2 across low body fat percentage shifted from a non-significant to a significant level after adjustment for covariates.
Model 2 fitted better than Model 1 (e.g., Nagelkerke R2 was 0.238 vs. 0.182, respectively), so patients with low body fat percentage had 8.5 times greater odds for belonging to the patients with anemia compared to the patients with normal or increased body fat. Those who had total serum protein level
Figure 2. A direct correlation between hemoglobin level and total serum protein level was observed (ρ = 0.479, p 4. Discussion
The main finding of the present study is the relationship between poor nutritional status and anemia in patients with UC. The phenotypic undernutrition indicators associated with anemia were decreased total serum protein and total body fat mass deficit. Based on the available literature, the pathogenetic pathways connecting these two factors with anemia were considered.
Hypoproteinemia in IBD may result from either systemic inflammation or decreased absorption of amino acids in the gastrointestinal tract. The main mechanism of hypoproteinemia in inflammation is elevated blood concentrations of proinflammatory cytokines, such as tumor necrosis factor-α, interleukin-1β, and interleukin-6 [
19,
20]. These cytokines inhibit the biosynthesis of negative acute phase proteins such as albumin and transferrin in hepatocytes, and increase the fractional catabolic rate of albumin. In addition, increased leakage of albumin into the interstitial space due to increased microvascular permeability occurs during acute phase or exacerbated chronic inflammation [
21], which all result in hypoalbuminemia. Because many globulins are positive acute-phase proteins demonstrating elevated levels during inflammation, it is hypothesized that hypoproteinemia was due to hypoalbuminemia in the cohort of patients in this study. Therefore, if hypoalbuminemia is regarded as a marker of inflammation intensity, it would be logical to anticipate that patients with hypoalbuminemia will develop AI [
12]. In this respect, it would be of interest to correlate the levels of albumin with disease activity and the extent of colonic involvement. The second potential cause of hypoproteinemia in the current patient sample is the decreased rate of blood protein synthesis in hepatocytes due to decreased available amino acids [
22]. This can be attributed to a decreased protein intake, impaired digestion of dietary protein, and decreased amino acid absorption. Lambert et al. [
23] demonstrated normal protein intake in patients with IBD. The decreased amino acid absorption rate secondary to mucosal injury is a likely plausible explanation mainly in patients with Crohn’s disease, because only 5% of dietary protein is absorbed in the colon. Nonetheless, decreased amino acid absorption can contribute to hypoproteinemia in patients with UC because of systemic hypercytokinemia effects on enterocyte apoptosis [
24]. Irrespective of the exact mechanism, if one considers hypoproteinemia as a phenotypic criterion of undernutrition, it will lead to the appreciation of factors such as depletion of the free amino acid pool for globin synthesis within maturing erythroid cells in the pathogenesis of anemia in IBD.Low body fat percentage was the second nutritional parameter that demonstrated a significant association with anemia in the adjusted binary logistic regression model. Three principal mechanisms of decreased body fat mass in IBD have been described in the literature [
25,
26]. First, enterocellular malabsorption may be accompanied by impaired absorption and resynthesis of triglycerides due to mucosal injury by leukocyte infiltration [
27], enterocyte apoptosis [
28], and loss of tight junctions between enterocytes [
29]. Second, fat deficit might be accounted for by decreased food intake due to decreased appetite and postprandial abdominal pain [
23]. In this case, the caloric requirements of the body are not fully met, resulting in the partial utilization of endogenous substrates and triglycerides. Third, hypercytokinemia is associated with increased catabolism of triglycerides and an accelerated basal metabolic rate [
30]. The changes in protein-related compartments were not analyzed in the present study; however, it is known that approximately 42% of patients with IBD develop sarcopenia, which persists during disease remission and is found in patients with normal and even increased BMI [
31,
32]. The latter phenomenon, termed sarcopenic obesity, may explain the lack of association between BMI and anemia in the current study, as BMI in such patients cannot be considered a reliable criterion of undernutrition [
33]. Meanwhile, sarcopenia might have demonstrated a strong association with anemia, considering that the free amino acid pool for globin synthesis is derived from muscle protein catabolism or intestinal absorption.This research confirmed the association between anemia and fat tissue deficit. This finding could be explained by existing data on the stimulatory effects of the adipose tissue-derived hormone leptin on in vitro and in vivo erythropoiesis [
34,
35] in conjunction with the well-established direct correlation between plasma leptin concentration and body fat mass [
36]. Thus, patients with body fat deficit might have relative leptin deficiency which contributes to the development of complex anemia in this patient cohort.The data obtained previously on cancer patients lend support to this view. In particular, Maccio et al. [
37] investigated 888 patients with solid cancer and showed that leptin concentration, albumin level, and BMI were positively correlated with hemoglobin level. However, the association between hemoglobin concentration and total body fat percentage demonstrates a bell-shaped curve and seems to have a more complex pattern than direct correlation. It is well established that the majority of patients with morbid obesity have anemia, a mixture of IDA and AI according to its origin. Markedly elevated plasma leptin stimulates hepcidin expression in hepatocytes, thereby causing sequestration of iron in macrophages and decreasing iron absorption in the small intestine [
38,
39,
40]. In conclusion, the results obtained improved the understanding of anemia pathogenesis in IBD patients and added two potentially new etiological factors: deficiency of amino acids for globin synthesis and leptin deficiency-mediated decreased erythropoiesis.
The present study has several limitations. First, important parameters relevant to disease activity (e.g., C-reactive protein and proinflammatory cytokines) and iron metabolism (transferrin, ferritin, hepcidin, etc.) were not presented and analyzed because of the study’s retrospective design. Second, alterations in protein-related body compartments highly relevant to the mechanisms of anemia were not analyzed because of the lack of data in the records. Third, the number of patients with anemia in our cohort was relatively small (n = 32). When performing statistical analysis and modeling, we relied on the total numbers of patients in the sample rather than on the prevalence of parameters under study in the cohort. Moreover, it was impossible to envisage the real prevalence of anemia, hypoproteinemia, etc. in the population studied at the moment of study initiation. According to the generally held principles of logistic regression modeling, it is sufficient to have at least 10 observations per each studied independent variable. Fourth, the cross-sectional study design provides only limited evidence for the causal role of undernutrition in anemia. It should be noted, however, that the majority of analyzed factors with putative effects on iron metabolism and/or erythropoiesis, such as age, sex, and disease behavior, have already influenced the end-point at the time of hemoglobin measurement. This minimizes the probability of dynamic changes, although UC severity may be both the cause and consequence of malnutrition. Therefore, both patients with initial undernutrition and those with undernutrition secondary to severe UC might have been included in the study. It is presumed that such secondary interactions had minimal effect on the results of binary logistic regression modeling. Further studies will provide additional evidence of causality for the relationship between undernutrition and anemia in IBD patients using such criteria as “dose–response” effect, consistency of relationship, and experimental support.







留言 (0)