
Remember me






KEY PERSPECTIVE
What is novel?
This meta-analysis of research published in the last 5 yr demonstrates that psychological distress evaluated with brief screening measures is only associated with a 28% greater risk of first-onset cardiovascular disease (CVD). These results are comparable to those from previous meta-analyses including data based on formal psychological evaluations or medical record diagnoses, suggesting that screeners alone are sufficient for capturing the CVD risk associated with psychological distress.What are the clinical and/or research implications?
Using brief psychological screeners in clinical or community settings is feasible and helpful for early CVD risk stratification. Even without meeting criteria for high psychological distress, patients may benefit from gold standard evidence-based interventions or additional supportive resources to aid CVD primary prevention.Primary prevention initiatives are gaining in prevalence to forestall the onset of cardiovascular disease (CVD).1,2 In the United States (US), patients and their health care providers are currently afforded the most advanced biobehavioral toolkit for cardiovascular risk reduction.3 Still, with an obesity epidemic, sedentary lifestyles, an aging population, and broadening social health disparities, CVD prevalence and associated costs of health care and human life continue to rise.4
Psychological health is an important dimension of cardiovascular health and well-being.5,6 Significant evidence from epidemiology, psychology, psychiatry, cardiology, and public health shows that psychological distress (ie, elevated symptoms of depression, anxiety, post-traumatic stress disorder (PTSD), or perceived psychosocial stress) is associated with earlier CVD onset, more rapid CVD progression, poorer prognosis, and an increased risk of related death.7–14 INTERHEART, a global, case-control study of first myocardial infarction, was one of the largest investigations to demonstrate the importance of psychological health: the population attributable risk of psychological stress and depression was 33%, which exceeded the risk associated with some traditional factors for CVD (eg, hypertension and physical inactivity).15 Additional, prospective cohort studies and meta-analytic summaries have since reinforced these findings, offering compelling evidence that psychological distress—based on clinical diagnoses, formal diagnostic interviews, or self-reported symptoms—is involved in the risk for, and burden of, CVD.9,12–14,16–18
With accumulating evidence linking psychological health and risk for CVD,19 leaders in cardiovascular medicine increasingly acknowledge the importance of psychological health in cardiac and vascular risk.5,20 Contradictory to this acknowledgment, and despite cardiovascular rehabilitation's longstanding empirically-based focus on psychological health and stance that psychological health is as equally important as traditional CVD risk factors, professional associations in cardiovascular medicine continue to be cautious about translating evidence concerning psychological health and cardiovascular risk into clinical guidelines for distress screening and management. Most prominently, the American Heart Association (AHA) recently updated their cardiovascular health metric to “The Essential 8” to include sleep, and suggested that psychological health serves as a context for other health factors (eg, sleep and weight), but that greater evidence is needed to guide the implementation of psychological screening and management.19 Historically, this tempered enthusiasm may have translated into a greater emphasis on psychological distress surveillance in patients with established CVD (eg, AHA Recommendations for Screening, Referral, and Treatment for Depression focused on patients with coronary heart disease) rather than identifying opportunities for primary prevention.21 As the cardiovascular risk that is associated with psychological distress likely begins well before CVD onset, and managing such symptoms appears strategic for reducing cardiovascular risk, patients and providers alike would benefit from the earlier identification of psychological distress.
Across medicine, policymakers, thought leaders, and professional organizations are advocating for more widespread surveillance of psychological distress in routine care settings. For example, since 2009, the US Preventive Services Task Force has recommended annual depression screening among adults aged ≥18 yr and highlighted increased depression risk among those with CVD,22 and the Centers for Medicare & Medicaid Services has covered annual depression screening for adults since 2011,23 but changes to US health care policy develop slowly. As the current health care delivery landscape demands efficient evaluation of patient distress,24 efforts to monitor psychological health using brief, validated self-report measures rather than more burdensome, comprehensive, psychological evaluations or psychiatric interviews continue to gain momentum. Several recent meta-analyses have summarized literature concerning psychological distress and initial CVD risk.7,9–11,14 Yet, no such investigation has specifically focused on the use of brief, self-report screening measures to evaluate distress. This effort is integral to creating screening guidelines for psychological distress in the service of CVD prevention, efforts that will particularly benefit populations with a high risk of CVD.
The primary objective of this investigation was to update and extend literature concerning psychological health and the incidence of new-onset CVD or related mortality by conducting a systematized review of all recent studies in which psychological distress was identified with brief, self-report screening measures only. A complementary objective was to quantify the strength of recent evidence via meta-analysis. Given the breadth of this literature, and past meta-analyses of subdomains of psychological health, a final objective was to identify opportunities for further research concerning psychological health screening and CVD and to develop recommendations for applying these results to improve the implementation of such measures in CVD primary prevention.
METHODS SEARCH PROCEDURESThe Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement25 was used to guide the literature search and associated statistical analyses. Studies were included in the systematized review if they were (1) published in the last 5 yr (2017-2022), to provide estimates based on the most recent state of this science, (2) designed to evaluate the prospective association of psychological health (ie, symptoms of depression, anxiety, PTSD, psychosocial stress, or general mental health-related quality of life) that was assessed at baseline with a validated self-report measure, and risk for incident CVD events, diagnoses, hospitalization, or related mortality, (3) participants were aged ≥18 yr and free from a diagnosed psychiatric disorder at baseline, (4) participants did not have CVD at baseline or CVD was controlled in analyses of more heterogeneous samples, and (5) the follow-up duration was ≥6 mo. Studies were excluded if psychological health was assessed with a formal psychological evaluation or psychiatric interview, or if the predictor was based on a psychiatric diagnosis derived from the medical record. Due to the different pathophysiology of stroke compared with other types of CVD and recent findings highlighting the complexity of psychological distress as a predictor of fatal and nonfatal ischemic stroke,26,27 investigations that included stroke within a composite endpoint were excluded. Despite being a common endpoint, studies that focused on hypertension were also excluded due to being a risk factor for CVD rather than established CVD per se; and further, since the first diagnosis of hypertension typically predates CVD by many years, prevention processes and timelines are likely very different. We excluded records from non-peer-reviewed sources such as theses, dissertations, and conference abstracts, due to different standards of peer review. We also excluded studies not available in English. The primary meta-analysis was limited to studies reporting adjusted HR and associated 95% CI (or other information allowing for their calculation) for an association between psychological distress and a relevant CVD outcome. Studies that only reported continuous HR were excluded because our primary interest was in determining whether high distress (relative to low or no distress) was associated with CVD risk.
INFORMATION SOURCES AND SEARCH STRATEGYA medical librarian (L.M.F.) searched the MEDLINE (Ovid), Embase (Embase.com), and American Psychological Association (APA) PsycInfo (EBSCO) databases for relevant journal articles. The final search was conducted on May 16, 2022. The following search terms were among those used to identify the appropriate articles: anxiety; depression; depressive disorder; stress disorders, posttraumatic; posttraumatic stress disorder; perceived stress; psychosocial stress; stress; GAD-7; PHQ-9; Patient Health or Penn State Worry or General Health Questionnaire; DBI or STAI or BAI or BDI-II; or state-trait or (Spielberger or mental health) W3 (inventory HDRS or Ham-D or HADS or CESD or CES-D or HDI or SDS or GDS or HADS-D; Hamilton or hospital or center for epidemiologic studies or self-rating or geriatric or Zung self-rating) W3 (depression scale); CVD; coronary disease; myocardial infarction; myocardial ischemia; death, sudden, cardiac; coronary artery disease; atrial fibrillation; heart failure; peripheral artery disease; peripheral vascular diseases; risk; incidence; or new or onset or risk or predict; and all the possible combinations of these terms.
Duplicate records were removed via auto-deduplication in EndNote 20 and manual deduplication. Title and abstract screening were completed in Covidence according to inclusion and exclusion criteria outlined earlier, and irrelevant articles were excluded. Next, the full texts of the remaining articles were thoroughly examined according to the criteria, and unrelated studies were again excluded in EndNote. To maintain objectivity, screening and data extraction activities were performed by two independent reviewers (A.E.G. and E.C.G.). To ensure a comprehensive search, the reference lists used within all the collected articles were manually reviewed. Interrater reliability was assessed for full-text review, with raters agreeing on 77% of the records. Discrepancies were resolved through discussion until consensus was reached.
STUDY SELECTION AND DATA EXTRACTIONA total of 3943 records were initially identified through the database searches: MEDLINE (n = 1616), Embase (n = 1733), and APA PsycInfo (n = 594). Of the initial search, 498 duplicate records were removed, and 3445 records were eligible for title and abstract screening.
Data from the final studies were extracted using detailed coding forms. Items included: article title, name of first author, year of publication, place of study, sample size, assessment method, demographics of the sample (average age, sex, race and ethnicity, and marital status), type of study, the prevalence of depression, anxiety, and stress, method of assessing psychological distress, CVD outcomes, and statistical details (ie, maximally adjusted HR and 95% CI, covariates). For inclusion in the meta-analysis, when studies with overlapping samples were identified, we prioritized the study with the largest sample, which reported an association between baseline psychological distress and a relevant outcome. When studies with overlapping samples reported different cardiovascular outcomes, we prioritized the study reporting the most relevant cardiovascular outcome. If studies reported HR associated with tertiles or quantiles, the highest category was included. Fixed-effects methods were used to combine subgroups and derive a study-level effect. For studies reporting outcomes associated with more than one metric of psychological distress (ie, depression and anxiety), we prioritized the nondepression psychological construct, given the more limited number of such studies. We requested additional information from authors of five additional studies, but none responded in the allotted time (ie, 4 mo).
STATISTICAL ANALYSISFor the primary analysis, adjusted HRs reflecting the association between psychological distress and CVD morbidity risk were used as the measure of effect; other measures of relative risk were considered equivalent for the purposes of this analysis. Hazard ratios > 1 indicated that psychological distress (eg, high symptoms of depression) was associated with a greater incidence of CVD. As part of a sensitivity analysis, a broader definition of relative risk was used to pool adjusted HRs and unadjusted or adjusted ORs of associations between psychological distress and risk of CVD morbidity or mortality.
Random-effects procedures with a restricted information maximum likelihood approach were used to aggregate effect sizes (ie, logarithmic adjusted HR) and corresponding 95% CI to estimate the overall effect, which was converted back to an HR.28,29 The Q statistic was computed to assess heterogeneity (ie, inferred from a significant value). Outcome consistency across studies was estimated based on the I2 index and its corresponding 95% CI.30,31I2 values of 25%, 50%, and 75% are interpreted as low, medium, or high heterogeneity.32 Analyses were conducted using the Stata meta package Version 16 (Stata Corp., College Station, Texas).33
We assessed publication bias for analyses with outcomes that were reported in ≥10 studies.34 Visual inspection of funnel plots and Egger's test were used to evaluate the possibility of publication bias and small study effects, respectively.35–37
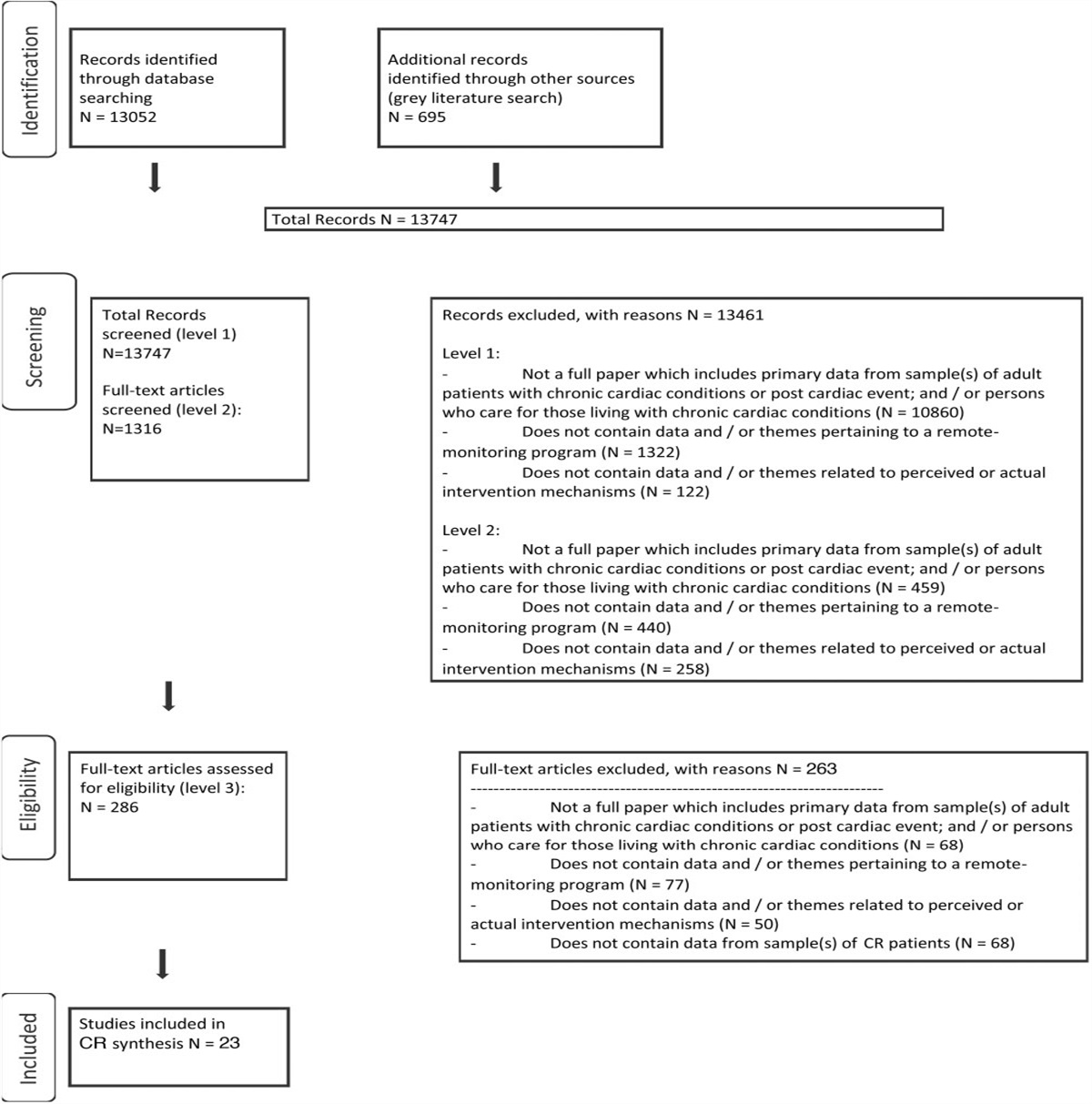
RESULTSOf the 3445 records from the original search, 3251 were excluded in the title and abstract review, and 166 records were excluded in the full-text review. Ultimately, 28 investigations met the inclusion criteria and had an endpoint of CVD morbidity or mortality, of which 18 were included in our analyses (Figure 1 includes additional details of the study selection process).
 Figure 1.: PRISMA 2020 flow diagram of screening and selection procedures. This figure is available in color online (www.jcrpjournal.com).SAMPLE CHARACTERISTICS
Figure 1.: PRISMA 2020 flow diagram of screening and selection procedures. This figure is available in color online (www.jcrpjournal.com).SAMPLE CHARACTERISTICS
Altogether, the studies represented 658 331 participants (58.1% women; 66.9% White [n = 13 reported data on race]; and 67.0% married or cohabiting [n = 11 reported relevant data]). Characteristics of the included prospective cohort studies are depicted in the Table, separated by the type of psychological distress. Most investigations included samples of healthy adults (n = 13), although others were limited to adults of middle-aged and older (n = 10), members of specific racial/ethnic groups (n = 3), men (n = 2), post-9/11 emergency workers (n = 1), or US military veterans (n = 1). Most participants were self-selected from the broader population (n = 21), but some were recruited through a clinical contact (n = 4), electronic health records (n = 1), or other means (n = 4; eg, employed in the British Civil Service). In terms of risk factors for CVD, 21.9% of participants smoked (n = 24), 11.2% had diabetes (n = 19), 41.7% had hypertension (n = 17), and the average body mass index was 26.3 ± 4.4 (n = 11).
Table - Characteristics of the Included Studies, Separated by Type of Psychological Distress Study Region Baseline, yr Sample, n Follow-up Duration, mo Age, Mean or Median, yr Women, % Measure of Psychological Distress CVD Outcomes Covariates Depression Deschenes et al (2020)38 Quebec, Canada 2009-2010 33 455 84 53 57 PHQ CAD, HF, MI Age, sex, ethnicity, education, smoking, alcohol, PA, cholesterol, DM, HTN Dixon et al (2022)39 12 Southeastern US states 2002-2009 23 937 132 53 (median) 64 CES-D HF Age, sex, race, HTN, HLD, DM, BMI, smoking, income, education, employment, marital status, alcohol, PA, number of close friends, depression, antidepressant use, cerebrovascular disease Feng et al (2020)40 Nord-Trøndelag County, Norway 2006-2008 37 402 96 53 57 HADS-Depression AF Age, sex, weight, height, smoking, occupation, marital status, PA, alcohol use, chronic disorders, blood glucose, BP, triglycerides, HDL, CRP Gaffey et al (2022)41 Jackson, Mississippi, USA 2000-2004 2 651 120 53 (median) 64 CES-D HF Age, education, income, HTN, DM, CHD, eGFR, total cholesterol, LVEF, alcohol abuse, smoking, obesity, PA, HR, SBP Garg et al (2019)42 Six US sites (Baltimore, MD; Chicago, IL; Forsyth County, NC; Los Angeles, CA; New York City, NY; St Paul, MN) 2000-2002 6 664 156 62 53 CES-D AF Age, sex, race, education, income, clinic site, cigarette smoking, BMI, height, DM, glucose, SBP, PA, statin use, antihypertensive use, alcohol use Han et al (2021)43 28 provinces in China 2011-2012 8 621 84 58 48 CES-D Composite Age, sex, zip code, education, smoking, alcohol use, BMI, SBP, antidepressant use, medical history Harshfield et al (2020)44 Consortium of 21 studies from Europe, North America, and Australia ERFC: 1974-2010 162 036 114 63 73 CES-D CAD Age, sex (stratified), smoking, DM Karlsen et al (2021)45 Six US sites (Birmingham, AL; Minneapolis, MN; Palo Alto, CA; Pittsburg, PA; Portland, OR; San Diego, CA) 2003-2005 3 095 144 76 0 GADS MI, HF, other Age, anxiety, education, ethnicity, DM, antidepressant use, smoking, alcohol use, BP, cholesterol, BMI, PA Ladwig et al (2017)46 Germany 1984-1985 3 428 120 58 0 von Zerssen symptom checklist: Depression/Exhaustion subscale CAD mortality Age, HCL, obesity, HTN, smoking, DM Lemogne et al (2017)47 France 1993 10 541 252 48 26 CES-D Composite Age, sex, occupational grade, parental history of CVD, alcohol use, smoking, PA, BMI, HTN, dyslipidemia, DM, sleep complaints Li et al (2019)48 28 provinces in China 2011-2012 12 417 48 58 51 CES-D Composite Age, sex, residence, marital status, education, smoking, alcohol use, SBP, BMI, history of diabetes, HTN, DLP, CKD, antihypertensives, DM medication, lipid lowering therapy Li et al (2020)49 28 provinces in China 2011-2012 6 810 24 58 53 CES-D Composite Age, sex, residence, marital status, baseline CES-D, education, smoking, alcohol use, obesity, HTN, DM, DLP, chronic kidney disease, inflammation Piantella et al (2021)50 London, England 1997-1999 7 610 132 56 3 General Health Questionnaire-Depression CAD Age, gender, smoking, BMI Poole and Steptoe (2018)51 England 2004 2 472 120 63 51 CES-D CAD Age, sex, ethnicity, cohabitation, wealth, smoking, SMI, alcohol use, regular physical activity, cognitive function, HTN Poole and Jackowska (2019)52 England 2014-2015 5 034 72 66 55 CES-D MI, other Age, sex, relationship status, income, BMI, smoker, alcohol use, PA, HTN, sleep problems Rantanen et al (2020)53 Harjavalta and Kokemäki, Finland 2005-2007 2 522 96 58 56 Beck Depression Inventory MI, PAD, angina, CAD Age, gender, education, smoking, alcohol use, PA, HTN, DLP Remch et al (2018)54 New York City, USA 2012-2013 5 971 48 51 17 PHQ MI, CV events Age, sex, BP, total cholesterol, BMI, tobacco use, respirator use Vu et al (2021)55 Four US sites: Washington County, MD, Forsyth County, NC, Suburbs of Minneapolis, MN, and Jackson, MS 2011-2013 6 025 66 75 59 CES-D HF Age, sex, race, education, income, smoking, alcohol use, PA, DM, BMI, HR, eGFR Yu et al (2022)56 Guizhou province, China 2010-2012 7 735 84 44 52 PHQ MI Age, sex, ethnicity, education, marriage, occupation, smoking, alcohol use, PA, history of T2DM, HTN, DLP, BMI Zhu et al (2022)57 28 provinces in China 2013-2014 9 595 60 58 52 CES-D CAD, HF, MI angina, other Age, gender, marital status, education, residency, smoking, alcohol use, HTN, DM, DLP, sleep duration Anxiety Feng et al (2020)40 Nord-Trøndelag County, Norway 2006-2008 37 402 96 53 57 HADS-Anxiety AF Age, sex, weight, height, smoking, occupation, marital status, physical activity, alcohol use, chronic disorders, metabolic components (glucose, BP, triglycerides, HDL, CRP) Karlsen et al (2020)45 Six US sites (Birmingham, AL; Minneapolis, MN; Palo Alto, CA; Pittsburg, PA; Portland, OR; San Diego, CA) 2000-2002 3 095 180 76 0 GADS MI, HF, other Age, education, ethnicity, smoking, BMI, PA, alcohol use, DM, BP, cholesterol, antidepressant use, anxiety PTSD Remch et al (2018)54 New York City, USA 2012-2013 5 971 48 51 17 PCL-C (civilian) MI, composite Age, sex, BMI, use of a respirator, BP, total cholesterol, tobacco use Scherrer et al (2020)58 USA 2008-2012 1 079 84 49 17 PCL Composite Age, race, gender, marital status, health insurance, depression, anxiety, sleep disorder, substance use, smoking, DM, HTN, HLD, obesity, duration of PTSD psychotherapy, antidepressant use Psychosocial stress Graff et al (2017)59 Denmark 2010 114 337 48 Largest age group: 55-64 (22.6%) 54 PSS AF Physical and psychiatric comorbid conditions, SES, lifestyle factors Santosa et al (2021)60 21 countries 2001-2003 118 706 122 50 59 Composite: PSS, Recent Adverse Life Events, Financial Stress CAD Age, sex, education, marital status, location, obesity, HTN, smoking, DM, family history of CVD, center General mental health/health-related quality of life Bonaccio et al (2018)61 Molise region, Italy 2005 17 102 60 53 53 Mental HRQoL CAD Age, sex, education, household income, occupational class, marital status, cancer, DM, HTN, HCL, psychological assessment, PA, BMI, diet, smoking, physical/metal health, CRP Nilsson et al (2020)62 County of Östergötland, Sweden 2003-2004 1 001 156 57 50 SF-36 Mental Health Subscale MI, composite Age, sex, and reporting at least one disease and/or neck/back pain Phyo et al (2021)63 Australia, USA 2010-2014 19 106 56 74 (median) 56 Medical Outcomes Study, SF-12 Mental Component Scale Composite Age, sex, race and ethnicity, education, living situation, country, smoking, alcohol use, PA Pinheiro et al (2019)64 USA 2003-2007 22 229 101 64 58 HRQoL, SF-12 Mental Component Summary score MI, composite Age, sex, race, education, relationship status, access to care, income, health insurance, residence, DM, HTN, AF, medication use, LVH, BMI, cholesterol, hsCRP, eGFR, CKD Wimmelman et al (2021)65 Copenhagen, Denmark 2009-2011 6 750 72 54 31 Satisfaction with Life Scale, SF-36 Vitality subscale Composite Age, sex, education, BMI, smoking, alcohol use, coronary calcium index, employment, social supportAbbreviations: AF, atrial fibrillation; BMI, body mass index; BP, blood pressure; CAD, coronary artery disease; CES-D, Center for Epidemiologic Studies Depression Scale; CHD, coronary heart disease; CKD, chronic kidney disease; CV, cardiovascular; CVD, cardiovascular disease; DLP, dyslipidemia; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; ERFC; GADS, Goldberg Anxiety and Depression Scales; HADS, Hospital Anxiety and Depression Scales; HCL, hypercholesterolemia; HDL, high-density lipoprotein; HF, heart failure; HR, heart rate; HRQoL, health-related quality of life; hsCRP, high-sensitivity c-reactive protein; HLD, hyperlipidemia; HTN, hypertension; LVH, left ventricular hypertrophy; LVEF, left ventricular ejection fraction; MI, myocardial infarction; PA, physical activity; PAD, peripheral artery disease; PCL, PTSD Checklist; PHQ, Patient Health Questionnaire; PSS, Perceived Stress Scale; PTSD, post-traumatic stress disorder; SBP, systolic blood pressure; SES, socioeconomic status; SF-12, Short Form-12; SF-36, Short Form-36; T2DM, type 2 diabetes mellitus.
aDuration of follow-up is reported as average rather than total.
The period of data collection ranged considerably, with the earliest baseline in 1974 and the most recent baseline in 2015. The average follow-up period was 98.3 ± 45.5 mo. Most investigations examined depressive symptoms (n = 20) or general mental health symptoms (n = 5), and a few examined symptoms of anxiety (n = 2), PTSD (n = 2), and stress (n = 2). Of the studies that focused on depression, the Center for Epidemiological Studies Depression Scale was particularly common (n = 12), and other measures consisted of the Patient Health Questionnaire (n = 3), the Beck Depression Inventory (n = 1), the Goldberg Anxiety and Depression Scales (n = 1), the Hospital Anxiety and Depression Scales-Depression subscale (n = 1), and the Depression and Exhaustion subscale of the von Zerssen symptom checklist. Anxiety was assessed with the Goldberg Anxiety and Depression Scales (n = 1), and the Hospital Anxiety and Depression Scales-Anxiety subscale (n = 1). Assessment of PTSD was conducted with the PTSD Checklist-Civilian version (n = 2). Stress was assessed with the Perceived Stress Scale (n = 1) or a composite of that scale, major adverse life events, and financial stress in the past year (n = 1). Finally, other general mental health screening was conducted with the SF-36 Mental Health Subscale (n = 1), Mental Health Related Quality of Life Scale (n = 1), SF-12 Mental Component Summary score (n = 2), and the Satisfaction with Life Scale (n = 1).
Outcomes consisted of a composite endpoint (n = 10), coronary artery disease (n = 9), myocardial infarction (n = 8), atrial fibrillation (n = 3), and heart failure (n = 6), although many studies included distinct tests of more than one outcome. Documentation of outcomes was most often based on a diagnosis or an event (eg, hospitalization; n = 15), and data were collected via self-report (n = 13), from a national register/database (n = 9), or by medical chart review (n = 6).
META-ANALYTIC RESULTSOut of the studies that met criteria and were reviewed, 15 studies that reported associations between baseline psychological distress and subsequent risk of CVD had sufficient data to include in the primary analysis. Overall, high symptoms of distress were associated with a 28% greater risk of CVD morbidity (95% CI, 1.18-1.39; Figure 2). Analyses of heterogeneity among the studies showed that effects were moderately heterogenous (Q[14] = 28.99, P= .010, I2= 48%). Study results were also summarized by distinct dimensions of psychological health (Figure 3). Evidence of publication bias was not observed, and relevant plots are depicted in the Supplemental Digital Content Figure (available at: https://links.lww.com/JCRP/A422).
 Figure 2.: Forest plot depicting analyses of psychological distress identified via brief screening measures and CVD morbidity and mortality, published 2017-2022 (n = 15). This figure is available in color online (www.jcrpjournal.com).
Figure 2.: Forest plot depicting analyses of psychological distress identified via brief screening measures and CVD morbidity and mortality, published 2017-2022 (n = 15). This figure is available in color online (www.jcrpjournal.com). Figure 3.: Psychological distress and risk of incident CVD and related mortality, by type of measure. Abbreviations: HRQoL, health-related quality of life; MH, mental health; PTSD, post-traumatic stress disorder. This figure is available in color online (www.jcrpjournal.com).
Figure 3.: Psychological distress and risk of incident CVD and related mortality, by type of measure. Abbreviations: HRQoL, health-related quality of life; MH, mental health; PTSD, post-traumatic stress disorder. This figure is available in color online (www.jcrpjournal.com).A sensitivity analysis was conducted treating ORs as equivalent to HR and including studies with CVD mortality as the outcome (overall, n = 18; Figure 4). Like results from the primary analyses, high distress was associated with a 28% greater risk of CVD morbidity and mortality. Analyses of the studies showed that effects were heterogenous (Q[17] = 54.54, P< .001, I2=63%).
 Figure 4.: Forest plot depicting sensitivity analysis of psychological distress and CVD morbidity and mortality (n = 18). Abbreviations: HRQoL, health-related quality of life; MH, mental health; PTSD, post-traumatic stress disorder. This figure is available in color online (www.jcrpjournal.com).DISCUSSION
Figure 4.: Forest plot depicting sensitivity analysis of psychological distress and CVD morbidity and mortality (n = 18). Abbreviations: HRQoL, health-related quality of life; MH, mental health; PTSD, post-traumatic stress disorder. This figure is available in color online (www.jcrpjournal.com).DISCUSSION
This systematized review consisted of 28 studies published from 2017 to 2022, which focused on self-reported psychological distress identified by brief screeners and incident CVD morbidity and mortality. Variability in methodology and statistical reporting resulted in 15 investigations available for the primary systematized meta-analysis. Overall, psychological distress (ie, elevated symptoms of depression, anxiety, PTSD, stress, or worse mental health-related quality of life) was associated with a 28% increased risk of CVD morbidity or mortality. Although multiple dimensions of psychological health were combined for the primary analysis, the observed effects were in a similar direction and ran
Comments (0)