
記住我

The global epidemic of type 2 diabetes is largely fueled by rapid urbanization and its impact on nutrition and lifestyle. An estimated 439 million people worldwide are projected to be affected by diabetes by the year 2030 [1]. The rise in the incidence and prevalence of diabetes is also paralleled by a continued rise in its systemic complications. Atrial fibrillation (AF) is one of the most commonly encountered cardiovascular complications of diabetes, with an overall risk of incident AF of more than 40% in some cohorts [2]. Encouragingly, oral antidiabetic agents such as biguanides (e.g. metformin) and sodium-glucose cotransporter-2 inhibitors (SGLT-2i) have shown promise in the mitigation of this heightened risk of AF in patients with diabetes [3]. However, limited existing evidence suggests that other antidiabetic agents such as glucagon-like peptide-1 receptor agonists (GLP-1 RA) and dipeptidyl peptidase-4 inhibitors (DPP-4i) may not offer similar benefits in overall risk reduction of AF in diabetes [4]. Therefore, we sought to study the association between AF-related adverse events (AEs) and GLP-1 RA, DPP-4i using the Food and Drug Administration’s Adverse Event Reporting System (FAERS) database.
Materials and methodsWe interrogated the FAERS database for reports of AF with GLP-1 RA and DPP-4i from January 2017 to 30 September 2021. We limited our search period to only the last 5 years to help exclude a potential selection bias, since semaglutide (a GLP-1 RA) was approved by the FDA in 2017. Search terms used to include drugs in the DPP-4i group were “sitagliptin” OR “sitagliptin hydrochloride” OR “sitagliptin phosphate” OR “saxagliptin” OR “saxagliptin benzoate hydrate” OR “saxagliptin hydrochloride” OR “saxagliptin monohydrate” OR “linagliptin”. Search terms used to include drugs in GLP-1 RA group were “dulaglutide” OR “exenatide” OR “exenatide synthetic” OR “liraglutide” OR “semaglutide”. Search terms also included “metformin”, “metformin hydrochloride” for biguanides; “glipizide”, “glimepiride”, “glyburide” for sulfonylureases, and “canagliflozin”, “empagliflozin”, “dapagliflozin” for SGLT-2i. The search term used to identify signals for the AE of interest was “atrial fibrillation”. The total number of AE reports and reports under “atrial fibrillation” were extracted for each drug for inclusion in the final analysis. The drugs “alogliptin” and “albiglutide” were excluded from the final analysis as the total reported AEs of interest were less than four for both of these drugs. The reporting of the AE of interest (i.e. AF) for the drugs included in the final analysis was compared with all the other drugs in FAERS. In large pharmacovigilance database studies, disproportionality analysis (also known as case-noncase analysis) is a tool that is employed to generate hypotheses on possible causal relationships between drugs and AEs. The detailed methodology of the disproportionality analysis has been previously described [5]. In the current study, we used the reporting odds ratio (ROR); defined as the odds of a certain event occurring with the given drug in comparison to all the other drugs in a database, to perform the disproportionality analysis. A signal-to-noise ratio was considered to be detected and significant if the confidence interval (CI) did not include the number “one (1)”. Data were collected and analyzed using JMP 15 (SAS Institute, Cary, North Carolina, USA).
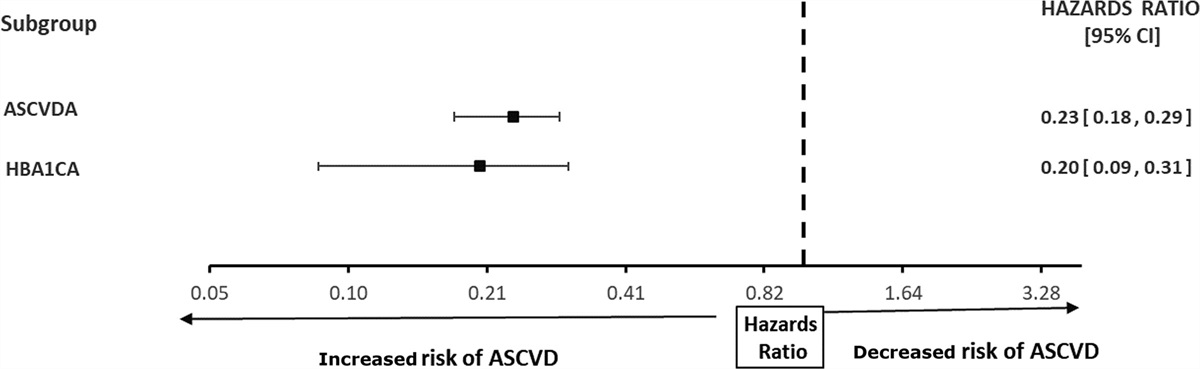
ResultsDuring the search period, a total of 10 182 525 AE reports were identified in the FAERS database, out of which 75 264 and 12 872 AE reports were in the GLP-1 RA DPP-4i groups, respectively. When analyzed for AF events as a proportion of total AE for individual drugs, linagliptin (40/3363, 1.18%) had the highest proportion of AF events followed by saxagliptin (12/1138, 1.05%), liraglutide (75/9829, 0.76%), sitagliptin (48/8371, 0.57%), semaglutide (39/9128, 0.42%), and exenatide (52/17 335, 0.29%) (Table 1). The proportion of cardiac AE attributable to AF was the highest for liraglutide (75/431, 17.4%) followed by semaglutide (39/298, 13.1%), exenatide (52/17 335, 11.7%), linagliptin (40/3363, 11.1%), and dulaglutide (81/792, 10.2%). As shown in Fig. 1, the signal of disproportionate reporting of AF was highest with linagliptin with an ROR of 3.93 (95% CI, 2.88–5.37) followed by saxagliptin (ROR, 3.48; 95% CI, 1.97–6.15), liraglutide (ROR, 2.51; 95% CI, 2.00–3.15), sitagliptin (ROR, 1.88; 95% CI, 1.41–2.50), and semaglutide (ROR, 1.40; 95% CI, 1.02–1.92). The reporting of AF was disproportionately lower with dulaglutide (ROR, 0.67; 95% CI, 0.54–0.84), whereas there was no signal detection with exenatide (ROR, 0.98; 95% CI, 0.74–1.29). A signal of disproportionate reporting of AF was detected with the DPP-4i group compared with all the other drugs in the FAERS database (ROR, 2.56; 95% CI, 2.10–3.12), whereas there was no disproportionality signal detected with the GLP-1 RA group (ROR, 0.90; 95% CI, 0.78–1.03). ROR of AF for metformin, sulfonylureas, and SGLT-2i are shown in Fig. 1. A sensitivity analysis was performed by excluding the reports listing any other drugs to rule out the risk of indication and coprescription bias. The signal of disproportionate reporting of AF with the DPP-4i group persisted after the sensitivity analysis (ROR, 1.82; 95% CI, 1.33–2.50), whereas there was no disproportionality signal for metformin (ROR, 1.26; 95% CI, 0.93–1.71).
Table 1 - Total adverse event, cardiac adverse event, and atrial fibrillation events reported with different glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors group of drugs Drug Total adverse events Cardiac adverse events Atrial fibrillation Percentage of AF out of total AE DPP-4i 12 872 1357 100 0.77 Sitagliptin 8371 528 48 0.57 Saxagliptin 1138 468 12 1.05 Linagliptin 3363 361 40 1.18 GLP-1 RA 75 264 1964 208 0.27 Dulaglutide 38 972 792 81 0.20 Exenatide 17 335 443 52 0.29 Liraglutide 9829 431 75 0.76 Semaglutide 9128 298 39 0.42 SGLT-2i 34 008 1914 142 0.41 Canagliflozin 12 051 578 37 0.31 Empagliflozin 16 690 930 79 0.47 Dapagliflozin 5267 406 26 0.49 Metformin 46 320 4447 208 0.44 Sulfonylureas 5627 479 30 0.53AE, adverse events; DPP-4i, dipeptidyl peptidase-4 inhibitors; GLP-1 RA, glucagon-like peptide-1 receptor agonists; SGLT-2i, sodium-glucose cotransporter-2 inhibitors.
 Fig. 1:
Fig. 1: Forest plot demonstrating the reporting odds ratios of atrial fibrillation events associated with dipeptidyl peptidase-4 inhibitors and glucagon-like peptide-1 receptor agonists.
DiscussionIn this real-world disproportionality analysis using FAERS, we did not find any disproportionality signal of AF reporting with GLP-1 RA; however, we detected a disproportionality signal with reporting of AF in the DPP-4i group when compared with all the other drugs in the FAERS database. To the best of our knowledge, this is the first pharmacovigilance analysis investigating the impact of GLP-1 RA and DPP-4i on AF risk in diabetes.
In a recent meta-analysis of 43 clinical trials enrolling 63 134 patients, the use of GLP-1 RA did not correlate with an increased risk of AF [mantel-haenszel-OR, 0.94 (0.84–1.04)] [6]. Similarly, a phase IV clinical trial did not report an increased risk of AF with albiglutide (relative risk, 0.82; 95% CI, 0.64–1.06), reiterating the cardiac safety of the drug in this regard [7]. As discussed before, our disproportionality analysis with GLP-1 RA complements the available evidence. However, we identified a significantly high signal of disproportionality for AF reporting with liraglutide (ROR, 2.51; 95% CI, 2.00–3.15), which needs to be further investigated in real-time studies. Existing studies have shown no significant increase in the risk of AF associated with DPP-4i use in patients with diabetes. A case–control study of 14 410 patients demonstrated that DPP-4i were not significantly associated with AF (OR, 1.07; 95% CI, 0.94–1.21; P > 0.05) [8]. However, we detected a strong disproportionality signal with the reporting of AF in the DPP-4i group when compared with all the other drugs in the FAERS database. A significant disproportionality signal was detected with DPP-4i in the sensitivity analysis even after excluding all possible cases with coprescription, which further validates our findings. Interestingly, DPP-4i have been noted to cause sympathetic activation and potentiate the risk of heart failure in patients with diabetes. DPP-4i also result in augmented Ca++/calmodulin-dependent protein kinase II signaling, which has been linked with heart failure and arrhythmias including AF [9,10]. Perhaps, more rigorous translational research is needed to gain greater insight into the underlying mechanisms driving the arrhythmogenesis of AF related to DPP-4i in patients with diabetes. Our analysis also detected a small signal-to-noise ratio for AF with metformin, although prior studies demonstrated a lower risk of AF with metformin when used by itself or as compared with sulfonylureas [11,12]. This could be explained by a potential coprescription bias, because there was no disproportionality signal detected in the sensitivity analysis.
A crucial limitation of performing and interpreting a disproportionality analysis using the FAERS database is that baseline data on underlying cardiac comorbidities among patients on these antidiabetic drugs are unknown. As a result, we could not perform an adjusted analysis to eliminate potential confounders such as comorbidities, other chronic medications, etc. However, we used robust analytic strategies and vigorous vetting to mitigate the risk of biased findings, which are commonly encountered with pharmacovigilance disproportionality analyses [13].
The current analysis offers support to the existing body of literature demonstrating the cardiac safety of GLP-1 RA but raises concerns about the apparent increase in the risk of AF associated with DPP-4i. These findings underscore the need for stronger prospective clinical data to establish the cardiac safety of GLP-1 RA and DPP-4i and investigate their role in mitigating the AF risk in patients with diabetes.
AcknowledgementsThis study was supported by an Institutional Development Award from the National Institutes of General Medical Sciences of the National Institutes of Health (NIH) under grant number P20GM121307 to C.G. Kevil.
This current report was presented as an oral presentation at the American Heart Association Meeting held in Boston, Massachusetts, in November 2021.
Conflicts of interestThere are no conflicts of interest.
References 1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010; 87:4–14. 2. Dublin S, Glazer NL, Smith NL, Psaty BM, Lumley T, Wiggins KL, et al. Diabetes mellitus, glycemic control, and risk of atrial fibrillation. J Gen Intern Med 2010; 25:853–858. 3. Ong HT, Teo YH, Teo YN, Syn NL, Wee CF, Leong S, et al. Effects of sodium/glucose cotransporter inhibitors on atrial fibrillation and stroke: a meta-analysis. J Stroke Cerebrovasc Dis 2022; 31:106159. 4. Patoulias D, Toumpourleka M, Papadopoulos C, Doumas M. Meta-analysis evaluating the risk of atrial fibrillation with newer antidiabetics across the cardiovascular and renal outcome trials. Am J Cardiol 2021; 139:139–141. 5. Salem JE, Manouchehri A, Moey M, Lebrun-Vignes B, Bastarache L, Pariente A, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol 2018; 19:1579–1589. 6. Nreu B, Dicembrini I, Tinti F, Sesti G, Mannucci E, Monami M. Major cardiovascular events, heart failure, and atrial fibrillation in patients treated with glucagon-like peptide-1 receptor agonists: an updated meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis 2020; 30:1106–1114. 7. Hernandez AF, Green JB, Janmohamed S, D’Agostino RB Sr, Granger CB, Jones NP, et al.; Harmony Outcomes committees and investigators. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-controlled trial. Lancet 2018; 392:1519–1529. 8. Liou YS, Yang FY, Chen HY, Jong GP. Antihyperglycemic drugs use and new-onset atrial fibrillation: a population-based nested case control study. PLoS One 2018; 13:e0197245. 9. Packer M. Do DPP-4 inhibitors cause heart failure events by promoting adrenergically mediated cardiotoxicity? Clues from laboratory models and clinical trials. Circ Res 2018; 122:928–932. 10. Swaminathan PD, Purohit A, Hund TJ, Anderson ME. Calmodulin-dependent protein kinase II: linking heart failure and arrhythmias. Circ Res 2012; 110:1661–1677. 11. Ostropolets A, Elias PA, Reyes MV, Wan EY, Pajvani UB, Hripcsak G, Morrow JP. Metformin is associated with a lower risk of atrial fibrillation and ventricular arrhythmias compared with sulfonylureas: an observational study. Circ Arrhythm Electrophysiol 2021; 14:e009115. 12. Chang SH, Wu LS, Chiou MJ, Liu JR, Yu KH, Kuo CF, et al. Association of metformin with lower atrial fibrillation risk among patients with type 2 diabetes mellitus: a population-based dynamic cohort and in vitro studies. Cardiovasc Diabetol 2014; 13:123. 13. Raschi E, Poluzzi E, Salvo F, Pariente A, De Ponti F, Marchesini G, Moretti U. Pharmacovigilance of sodium-glucose cotransporter-2 inhibitors: what a clinician should know on disproportionality analysis of spontaneous reporting systems. Nutr Metab Cardiovasc Dis 2018; 28:533–542.
留言 (0)