
記住我

The use of personalised care planning has been effective at improving the health outcomes and the experience of care among people with type 2 diabetes (T2DM) and other long-term health conditions [1,2].
It has been recognised for many years that the achievement of a target HbA1c level for people with T2DM is associated with a reduced risk of cardiovascular events and a reduced mortality rate [3]. There are significant financial, organisational, information technology and time barriers among multidisciplinary teams of healthcare professionals in primary care that make it hard to co-create integrated plans of care, support and education for people with T2DM which impact on outcome [4].
This study was designed to evaluate whether personalised care planning software and a patient-facing mobile app could aid help patients to manage their diabetes more effectively – and for healthcare professionals working in primary care to improve health outcomes among patients with T2DM through the delivery of personalised plans of care, support and education, accessible on a mobile device.
MethodsPeople with T2DM with glycosylated haemoglobin (HbA1c) greater than 58 mmol/mol (7.5%) were randomised to either the active intervention group (app + usual care) or the control group (usual care).
Potential participants were identified by clinicians in each of the participating general practices according to the criteria defined in the methods section. Selection bias was minimised by recruitment through routine general practice diabetes clinics where consecutive clinic attendees fulfilling the inclusion criteria were invited.
The intervention group received a personalised care plan created by a healthcare professional, involving daily lifestyle prompts on the participant’s telephone and offering access to a range of online resources via an App for 6 months. Randomisation did not influence other decisions about diabetes management. Randomisation was performed using the ‘sealed envelope’ technique [5]. For participating patients the digital intervention was additional to usual care. Clinicians were not made aware of which patients were accessing the App.
In the first report to be generated from the study, we analysed data on a preliminary sample of 36 participants from Eastern Cheshire (out of a projected total of 250 participants) in relation to changes in BMI and HbA1c.
Uptake was 72% of those invited across the general practices.
Ethical approval was given by the Greater Manchester West Ethics Committee Reference Number: 20/NW/0203.
ResultsThe age range of participants was 42–84 years. Out of the total 36 participants, 20 were male and 16 were female, making up 55.6 and 44.4%, respectively. The treatment group (App + usual care) and control (usual care) groups were made up of 17 and 19 participants, respectively. For the treatment group, all 17 participants had HbA1c data, while only 14 had BMI data. Of those in the control group, 19 had HbA1c data and 18 had BMI data.
The mean starting HbA1c for the treatment group was 71.1 mmol/mol (±se 5.0 mmol/mol) and for the control group was 72.1 mmol/mol (±se 4.2 mmol/mol). For the treatment group, the end HbA1c result dropped to a mean average of 63.0 mmol/mol (±se 2.7 mmol/mol), with the control group end HbA1c dropping to 68.7 mmol/mol (±se 2.2 mmol/mol) on average (Fig. 1).
 Fig. 1:
Fig. 1: Change in (a) HbA1c and (b) BMI for each participant for the control (usual care) and treatment groups for each of the 36 participants.
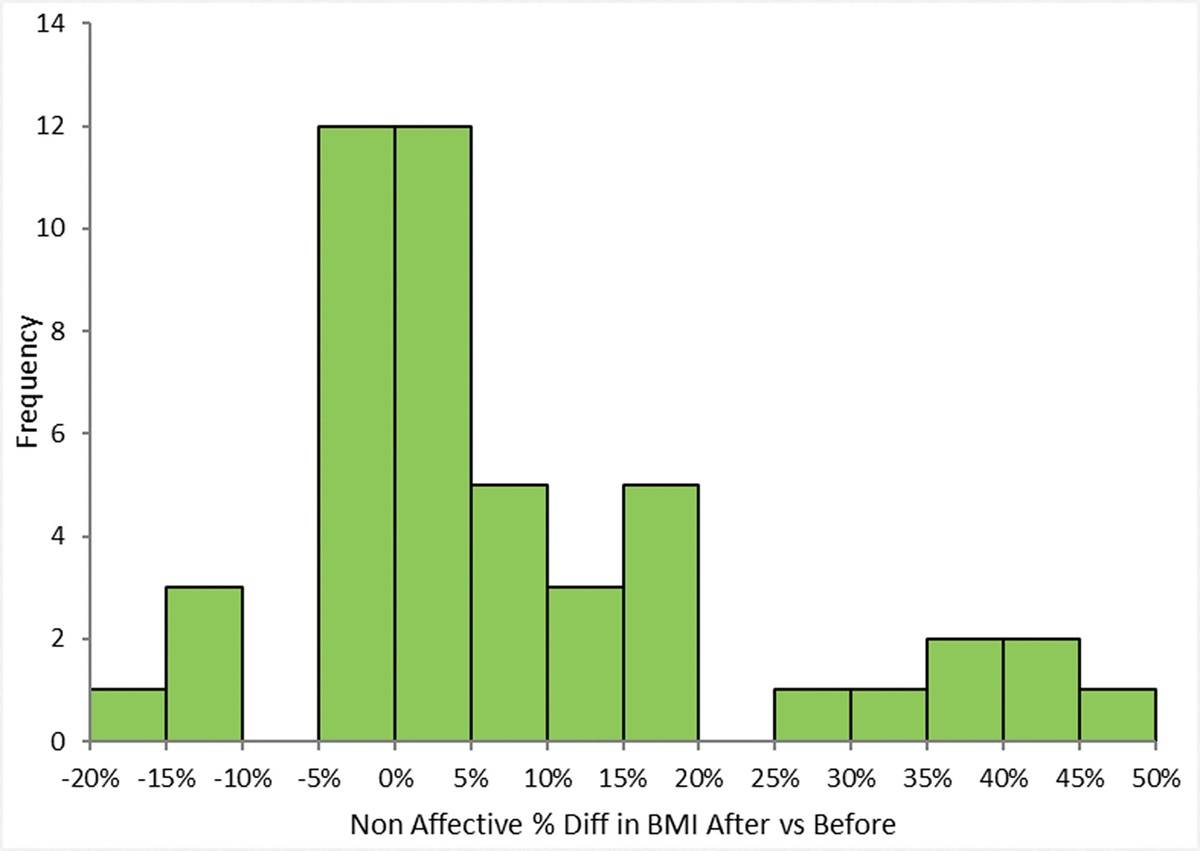
The mean starting BMI for the treatment group was 30.1 kg/m² (±se 1.3 kg/m²) and for the control group, who were receiving usual care, was 31.4 kg/m² (±se 1.0 kg/m²). For the treatment group, the latest BMI mean dropped to 30.0 kg/m² (±se 1.3 kg/m²), with the control group’s latest BMI average increasing to 31.4 kg/m² (±se 1.0 kg/m²) (Fig. 1).
The average percentage change in HbA1c for the treatment group was −9.5%, but just −2% for the control (usual care) group (P 0.015 for the difference). The average percentage change in BMI for the treatment group was −0.4%, but 0.1% for the control group (P 0.03 for the difference) (Fig. 2).
 Fig. 2.:
Fig. 2.: Average change in %HbA1c and %BMI for the control (usual care) and treatment groups.
DiscussionThese preliminary findings point to how the provision of personalised plans of care, support and education linked to a mobile app, can result in HbA1c and BMI reduction over a 6-month period for many individuals with T2DM. It has been shown that reducing HbA1c to target and reducing BMI can improve cardiovascular outcomes in people with T2DM. Specifically, in the multi-site Look AHEAD study [6] which randomised participants to intensive lifestyle intervention or diabetes support and education, those who lost at least 10% of their bodyweight vs. controls had a 20% lower risk of the primary outcome composite of death from cardiovascular causes, nonfatal acute myocardial infarction, nonfatal stroke, or admission to hospital for angina [6].
Our findings are in keeping with other studies that have examined how App-based solutions may improve glycaemic control when used as adjuncts to usual care [7–10].
Following these preliminary findings, the evaluation team will complete the recruitment and delivery of interventions for 250 remaining patients to power the statistical significance of the results from the study.
We accept that our findings only relate to a 6-month follow-up and that the full trial findings are awaited. Nevertheless, we feel that these encouraging results merit reporting.
Further research into the observed real-world experiences of patients who are using the mobile app will also be captured through a series of 1 to 1 interviews and will be cross-referenced with ‘in app’ analytics. These results, combined with the comparison of pre- and post-study completion of quality of life surveys for patients in both the control and treatment groups, will enable the evaluation team to further understand the mechanisms by which patient choices and actions are influenced by the educational content, services and experiences that healthcare professionals working in primary care utilise on a day to day basis.
AcknowledgementsThe research project was funded by Innovate UK.
Conflicts of interestThere are no conflicts of interest.
References 1. Velardo C, Shah SA, Gibson O, Clifford G, Heneghan C, Rutter H, et al.; EDGE COPD Team. Digital health system for personalised COPD long-term management. BMC Med Inform Decis Mak 2017; 17:19. 2. Foley P, Steinberg D, Levine E, Askew S, Batch BC, Puleo EM, et al. Track: a randomized controlled trial of a digital health obesity treatment intervention for medically vulnerable primary care patients. Contemp Clin Trials 2016; 48:12–20. 3. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000; 321:405–412. 4. Fisher L, Polonsky WH, Hessler D. Addressing diabetes distress in clinical care: a practical guide. Diabet Med 2019; 36:803–812. 6. Gregg EW, Jakicic JM, Blackburn G, Bloomquist P, Bray GA, Clark JM, et al.; Look AHEAD Research Group. Association of the magnitude of weight loss and changes in physical fitness with long-term cardiovascular disease outcomes in overweight or obese people with type 2 diabetes: a post-hoc analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol 2016; 4:913–921. 7. Bennett GG, Steinberg D, Askew S, Levine E, Foley P, Batch BC, et al. Effectiveness of an app and provider counseling for obesity treatment in primary care. Am J Prev Med 2018; 55:777–786. 8. Salari R, R Niakan Kalhori S, GhaziSaeedi M, Jeddi M, Nazari M, Fatehi F. Mobile-based and cloud-based system for self-management of people with type 2 diabetes: development and usability evaluation. J Med Internet Res 2021; 23:e18167. 9. Larsen K, Akindele B, Head H, Evans R, Mehta P, Hlatky Q, et al. Developing a user-centered digital clinical decision support app for evidence-based medication recommendations for type 2 diabetes mellitus: prototype user testing and validation study. JMIR Hum Factors 2022; 9:e33470. 10. Zimmermann G, Venkatesan A, Rawlings K, Scahill MD. Improved glycemic control with a digital health intervention in adults with type 2 diabetes: retrospective study. JMIR Diabetes 2021; 6:e28033.
留言 (0)