
記住我




In April 2020, the initial surge of pandemic of coronavirus disease 2019 (COVID-19) had hit Tokyo, Japan. Meanwhile, a critical shortage of life-saving resources such as mechanical ventilators (MV) and extracorporeal membrane oxygenation (ECMO) devices has become an imminent concern around the world. Residents of Tokyo were concerned about the situation worsening to the same standard as other countries. Our university hospital had performed approximately 30 cases of veno-arterial ECMO and 5 cases of veno-venous ECMO per year on average. Accordingly, in response to the COVID-19 surge plus the possible increasing demands of ECMO in Tokyo, we decided to accept severely hypoxic COVID-19 patients who need ECMO support to play a role as a tertiary referral center. We proactively established our own framework to deal with the dire situation. We formulated an in-house “guideline” for introducing ECMO to COVID-19 patients. What was unique about the guideline was that it adverted the issue of allocation and reallocation of the device. With limited experience and complicated information regarding severe COVID-19, we provisionally set the maximum duration of ECMO use to 14 days during times of limited resources when no lung recovery was observed based upon multiple reports and recommendations.1-3 Additionally, we launched a local ECMO support committee which consists of multidisciplinary medical professionals including attending physicians, nurses, and bioethicists who were involved in the patients' treatment. The committee held ethical/medical meetings twice a week to discuss whether ECMO continuation would be appropriate.
We herein report a severe COVID-19 case describing the struggle of physicians at the bedside under our local regulatory guideline resulting in ventilator-induced lung injury (VILI).
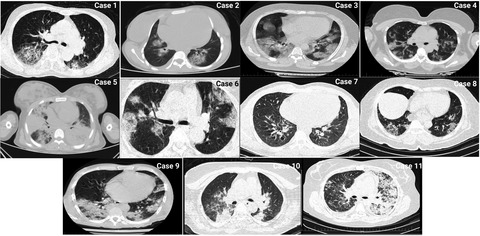
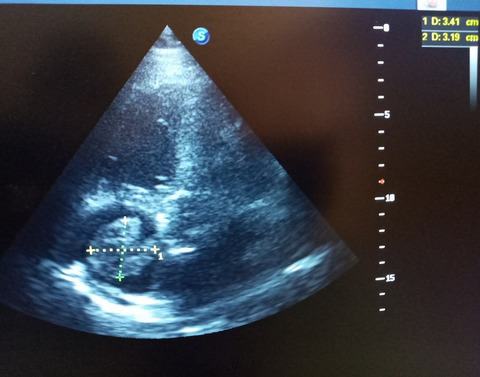
2 CASE HISTORYA 66-year-old man (63 kg, 21.6 kg/m2 of body mass index) with a history of hypertension and peptic ulcer disease with a smoking history of 76 pack-year was transferred to our ICU requiring invasive mechanical ventilation (MV) due to severe hypoxia by COVID-19 five days after disease onset. Computed tomography (CT) showed bilateral ground-glass opacities (Figure 1). Lung-protective strategy with anti-COVID-19 medication (Favipiravir, Hydroxychloroquine, Tocilizumab) and prone positioning therapy did not improve the patient's condition. After supine position replacement, the patient's PaO2/FiO2 (P/F) ratio decreased to 47, and he was immediately introduced to veno-venous ECMO on ICU day 8.

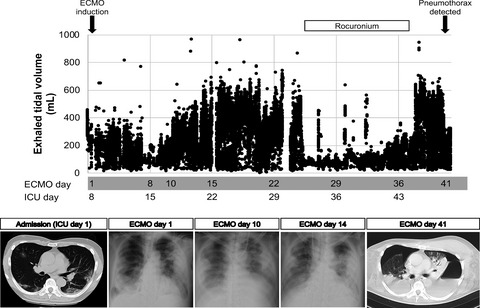
Tidal volume and chest radio-images. Each dot is the value of exhaled tidal volume extracted from mechanical ventilator (Evita® V300, Dräger, Germany), which was recorded every minute
The ECMO was placed via femoral vein and right jugular vein access, with Capiox EBS EMERSAVE® (TERUMO, Tokyo, Japan). We set the MV to achieve lung rest to have limited tidal volume (Figure 1, Ppeak 15–20 cm H2O, PEEP 10 cm H2O). Sedation (Propofol and/or Dexmedetomidine) was crucial to maintain synchrony between the MV and the patient's spontaneous breathing efforts as physicians observed abnormal breathing pattern such as paradoxical seesaw breathing which we surmised will also increase transpulmonary pressure. Despite carefully maintaining the patient under lung rest condition, the patient's respiratory parameters never improved by 10 days after initiating ECMO (E-day 10) and the designated 14-day ECMO period was about to expire. Physicians tried to liberate the patient from ECMO and accept a greater dependence on mechanical ventilation, in accordance with our in-house ECMO guidelines and to the ELSO guidelines1 that recommended the duration of ECMO within 14 days. We allowed spontaneous breathing to have tolerable tidal volume even at the cost of tolerating labored breathing. However, we failed to wean the patient from ECMO within the designated 14 days. The lung CT showed massive atelectasis and pleural fluid, which indicated a chance of improvement with appropriate intervention. Since there was no immediate demand of ECMO devices, the decision was made to continue ECMO therapy. In addition to ECMO therapy, we performed prone positioning, thoracentesis to remove pleural fluid, and high PEEP therapy for lung recruitment. After these therapeutic strategies, we attempted again to try weaning ECMO from the patient by shifting to a higher dependence on MV for another week allowing labored spontaneous breathing. Nonetheless, we failed to liberate the patient from ECMO. Under the allowance of the ECMO support team monitoring the number of COVID-19 patients in Tokyo, there was less concern about shortage of medical devices. Thus, we finally decided to wait for the patient's pulmonary function to improve under the lung rest condition achieved with rocuronium administration and an adequate ECMO support. On E-day 31, we exchanged the ECMO catheter with a new double-lumen single catheter (Avalon®, Maquet cardiopulmonary GmbH, Rastatt, Germany) via right internal jugular vein due to suspected catheter infection with Staphylococcus aureus. In addition, we administered methylprednisolone 1000 mg daily on E-day 33–37, and E-day 54–56, expecting suppression of inflammation and lung tissue recovery. These interventions for complete lung rest brought about a gradual increase of tidal volume under the fixed ventilator setting (Figure 1).
Subsequently, we discontinued rocuronium and cautiously managed the patient's breathing pattern adjusting sedation depth to keep acceptable tidal volume (Figure 1). However, on E-day 41, the patient developed bilateral pneumothorax (Figure 1) which developed into a nonresolving pneumothorax requiring multiple chest tubes. Although we attempted additional and aggressive treatments such as endobronchial embolization and surgical intervention, the pneumothorax remained refractory. Meanwhile, the patient developed pyothorax and sepsis. On E-day 82 (ICU day 89), the patient expired due to multiorgan failure derived from sepsis despite extensive antibiotic therapy.
On autopsy, there were hematomas on the thorax, pericardium, diaphragm, and within the lung tissue. There was premature fibrosis in the alveoli with lymphocyte infiltration. Alveolar wall damage was profoundly noted, and the preserved alveoli epithelium showed bronchiolar epithelial transformation with mucous within the alveolar space. There was no evidence of thrombosis in the lung, and no bacterium was found on gram staining and Grocott staining. Thrombi were noted only on ECMO catheter insertion sites, and there was no evidence of micro-thrombi. Interestingly, no other major abnormalities besides diffuse alveolar damage, which is commonly seen in COVID-19 infection,4 were found on pathological analysis. Thus, the lung injury is the primary cause of death on which the refractory pneumothorax should be a trigger of the fatal course followed by additional bacterial infection resulting in multiorgan failure.
3 DISCUSSIONIncomplete lung rest achievement may be the biggest reason to lose this case. Pneumothorax, the critical complication due to barotrauma or VILI in mechanically ventilated patients, has an established association with COVID-19.5 Steroid might have also boosted the development of pneumothorax in this case. Typical pathologic findings in COVID-19 pneumonia including interstitial pneumonia, consolidation, and in situ thrombosis may increase the friability of lung parenchyma and pleura, causing higher risk of fistulation between the distal airways and pleural space or hilum.5 Accordingly, a lung-protective strategy should be an essential therapeutic approach in severe COVID-19 patients. VV-ECMO management is one of these promising approaches to achieve lung rest and to allow a bridging period for lung recovery.6 However, we could not accomplish this strategy on this case.
What prevented us from achieving lung rest in this case even though we understood the importance? We believe that there are two reasons: (1) our lack of experience of severe COVID-19 patients, and (2) our strict accordance with the in-house ECMO guidelines, especially the designed duration of 14 days.
We experienced this case during the first surge of pandemic in a chaotic and unprecedented situation. We were groping for the appropriate treatment strategy against the deadly emerging infectious disease in the unknown: We had scarce knowledge on the pathophysiology or natural course of severe COVID-19 infection; we were confused by a lot of information regarding potential but unestablished treatment options at that time; and most of all, we were unsure how long we should wait and observe until we realize the effect of each treatment and detect a sign of recovery. We had no choice but to apply general ECMO management for severe ARDS correspondingly to the COVID-19 patient; however, we had no proof whether the lung condition of our patient was reversible or not. Thus, we were in the chimerical situation where we hesitated in determining the treatment strategy for the emerging lethal infectious disease.
On the other hand, the number of COVID-19 patients was increasing dramatically regardless of the clinical chaotic situation.7 A shortage of ECMO in Tokyo sounded still compulsive but more realistic at that time. Indeed, the discussion of future ECMO reallocation was brought in our daily conversation at bedside, which made clinicians tremendously burdened. Under the circumstance, we tried to strictly adhere to the 14-day period according to our guideline. We had no choice of transferring ECMO-dependent patients to the other hospital at that time because there were no other established ECMO centers in Tokyo. In fact, we tried multiple ECMO-withdrawal trials within the 14-day period, acknowledging compromised lung rest, as the ELSO guideline states “Given that ECMO is a finite resource, patients may have to be liberated from ECMO expeditiously where possible accepting a greater dependence on mechanical ventilation”.1 As a result, our direction of the patient's clinical management had lost the consistency. We had eventually wavered back and forth between the complete lung rest management and the aggressive mechanical ventilation, which might pose a great impact on the patient's prognosis.
What could we have done to avoid the unstable shift of clinical direction in the chaotic situation? The problem is the situation where the clinicians who were working for maximizing individual patients' benefits were required to consider social benefits, simultaneously, which could also cause clinicians moral stress and lead to professional burnout.8 Therefore, the possible answer for the question is establishing a third-party ethics support structure to separate bedside clinical teams from officers who determine social benefits.8-10 This approach will allow clinicians to focus on treatments based on egalitarianism with consistent and unbiased decision. Although our local ECMO support committee contributed to the case in overseeing and integrating management of our patients, most of our committee members were directly or indirectly involved in the individual patient care, which could have potentially caused bias. Additionally, the proposed third-party ethics support team could regulate its rationing criteria according to the local pandemic status, to provide the best outcomes from the utilitarian perspective. This is still an ongoing issue within our facility; although a year has passed, since the initiation of pandemic, explicit withdrawal criteria are yet to be established. However, we need to involve the entire community, not just one medical center, in such ethical discussion for reallocation of life-saving resources.11 There were reports of heterogeneity in the public opinion regarding resource allocation that differ from medical standpoints. Standardized criteria that reflect the community's opinion should be launched for a morally reliable measure that healthcare workers can depend on.
By the way, currently in Japan, Japan ECMOnet for COVID-19 has been developed to manage the demand for ECMO. This system conducts telephone consultations as well as further coordination including transport and ECMO physician dispatch.12 If resource scarcity could be handled by a multi-facility entity, quality of patient care in such pandemics could improve, and we can feel more comfortable in treating each patient, without worrying excessively about device reallocation. We are looking forward for beneficial outcomes of this newly established system.
4 CONCLUSIONAmid the compulsive concern of a shortage of ECMO under the chaotic situation with the pandemics of emerging lethal infectious disease, the utilitaristic view for ECMO management had interfered bedside clinicians to make appropriate clinical decisions. It is desirable to leave a role to make decisions for maximizing social benefits, such as reallocation and redistribution of life-saving resources including ECMO, to a third-party structure separated from bedside clinicians. Continuous discussion is warranted on the ethical dilemmas, and reallocation of the critical care resources involving with the entire community to prepare future pandemics and disasters.
ACKNOWLEDGMENTSWe would like to thank our ICU nursing staff, the members of palliative care team, the members of ECMO supporting team, and Prof. Hirokuni Arai of Department of Cardiovascular Surgery, in Tokyo Medical and Dental University for their professional support to provide the best care for the patient.
CONFLICT OF INTERESTNone.
AUTHOR CONTRIBUTIONSYI and NN drafted the manuscript and contributed to treating the patient. YM and TM performed literature review and contributed to treating the patient. MN contributed to the first draft and finalization of the manuscript. YT and KY performed pathophysiology test and drafted the manuscript. MY contributed to supporting evidence in medical ethics and critically revised and edited the manuscript. HS supervised the case report, critically revised and edited the manuscript. All authors have read and approved the final manuscript.
ETHICAL APPROVALNot applicable.
CONSENTWritten informed consent was obtained from the patient's next of kin to publish this report in accordance with the journal's patient consent policy.
REFERENCES
1Bartlett RH, Ogino MT, Brodie D, et al. Initial ELSO guidance document: ECMO for COVID-19 patients with severe cardiopulmonary failure. ASAIO J. 2020; 66(5): 472- 474. 2Rosenberg AA, Haft JW, Bartlett R, et al. Prolonged duration ECMO for ARDS: futility, native lung recovery, or transplantation? ASAIO J. 2013; 59: 642- 650. 3Posluszny J, Rycus PT, Bartlett RH, et al. Outcome of adult respiratory failure patients receiving prolonged (≥14 days) ECMO. Ann Surg. 2016; 263: 573- 581. 4Deshmukh V, Motwani R, Kumar A, Kumari C, Raza K. Histopathological observations in COVID-19: a systematic review. J Clin Pathol. 2020; 74(2): 76- 83. 5Zantah M, Dominguez Castillo E, Townsend R, Dikengil F, Criner GJ. Pneumothorax in COVID-19 disease- incidence and clinical characteristics. Respir Res. 2020; 21: 1- 9. 6Martinelli AW, Ingle T, Newman J, et al. COVID-19 and pneumothorax: a multicentre retrospective case series. Eur Respir J. 2020; 56: 2002697. 7Kim S, Misono E. As Japan coronavirus cases climb, pressure to secure medical equipment, staff rises. Mainichi Shimbun. 2020. 8Pawlikowski J. The ethical dimension of prioritization and allocation decisions within the context of the coronavirus disease 2019 pandemic. Polish Arch Intern Med. 2020; 130: 466- 472. 9Robert R, Kentish-Barnes N, Boyer A, Laurent A, Azoulay E, Reignier J. Ethical dilemmas due to the Covid-19 pandemic. Ann Intens Care. 2020; 10: 84. 10Lurie N, Saville M, Hatchett R, Halton J. The toughest triage. N Engl J Med. 2020; 382: 1969- 1973. 11Fallucchi F, Faravelli M, Quercia S. Fair allocation of scarce medical resources in the time of COVID-19: what do people think? J Med Ethics. 2021; 47: 3- 6. 12Ogura T, Ohshimo S, Liu K, Iwashita Y, Hashimoto S, Takeda S. Establishment of a disaster management-like system for COVID-19 patients requiring veno-venous extracorporeal membrane oxygenation in Japan. Membranes. 2021; 11(8): 625.
留言 (0)