1 INTRODUCTION
Encephalopathy associated with autoimmune thyroid disease (EAATD) is a rare neuropsychiatric syndrome characterized by symptoms of acute or subacute encephalopathy associated with anti-thyroid (anti-thyroid peroxidase [anti-TPO] and/or anti-thyroglobulin [anti-TG]) antibodies in the absence of alternative causes.1 EAATD either might be characterized by acute conditions such as episodes of cerebral ischemia, seizure, and psychosis or may happen in an indolent form accompanied by depression, cognitive decline, myoclonus, tremor, and fluctuations in the level of consciousness (LOC).2
Because of the low specificity of plasma anti-thyroid antibodies, cerebrospinal fluid (CSF) analysis and brain MRI are requested. Most patients respond well to steroid therapy with complete relief of symptoms, but they might have a relapse-recovery period. Hence, treatment duration and factors associated with treatment failure remain to be established.3, 4
Hashimoto's encephalopathy (HE), which is equivalent to corticosteroid-responsive encephalopathy related to autoimmune thyroiditis, is a rare, poorly mentioned, and often misdiagnosed neuropsychiatric status. Treatment should be tailored for an at least 6-month duration, and most cases do not require more than 12 months.5, 6 Here, we report a patient with HE who has shown auditory hallucinations (AH), behavioral disorders (BD), and severe problems in corticosteroid dose regulation.
2 CASE PRESENTATION
The case is a 42-year-old woman without psychiatric problems in the past. The patient has had no neuropsychiatric history, seizure, or any other neurological disorders characterized since the last 2 months she has been visiting the neurology clinic. She was admitted to a psychiatry hospital in a confusional state, with a history of progressive neurobehavioral symptoms such as dysphoric mood, sleep problems, speech difficulties, cognitive problems, and transient disorientation. Neurological examination revealed considerable time disorientation, inattention, anterograde amnesia, slurred speech, and stuttering.
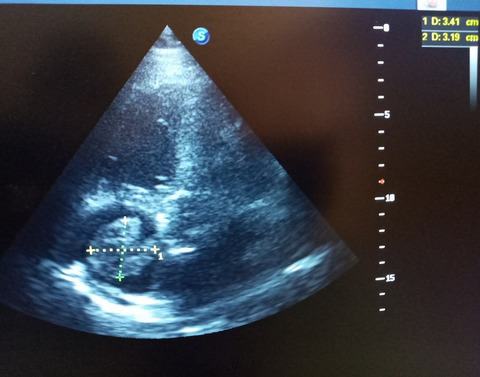
The laboratory data suggested hypothyroidism in the presence of very high levels of serum and CSF anti-TPO antibody (Table 1), while immunological laboratory tests were normal (Table 2). Brain MRI was also normal. However, electroencephalography (EEG) indicated slow background with transient sharp waves on bilateral temporal leads and thyroid ultrasound showed thyroid gland atrophy related to Hashimoto's disease. Laboratory evaluations are shown in Tables 1 and 2.
TABLE 1.
Laboratory findings in Hashimoto's encephalopathy
TSH
7.9 IU/mg
T3
0.9 IU/mg
T4
7.5 IU/mg
25-hydroxyvitamin D
52.3 IU
Anti-TPO
>1000
Abbreviations: IU/mg, unit per milligrams; T3, triiodothyronine; T4, thyroxine; TPO, thyroperoxidase; TSH, thyroid-stimulating hormone.
TABLE 2.
Immunological laboratory tests
anti-NMDR-R
Negative
p-ANCA
Negative
c-ANCA
Negative
anti-dsDNA
Negative
ANA
Negative
AMPAR
Negative
GABARB1
Negative
Caspr2
Negative
LGI1
Negative
anti-VGKC
Negative
Abbreviations: AMPAR, α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid; ANA, antinuclear antibody; anti-dsDNA, anti-double-stranded DNA; c-ANCA, antineutrophil cytoplasmic antibodies; Caspr2, contactin-associated protein 2; GABARB1, γ-aminobutyric acid receptor-B; LGI1, leucine-rich glioma-inactivated 1; NMDR-R, N-methyl-D-aspartate-receptor; p-ANCA, perinuclear antineutrophil cytoplasmic antibodies; VGKC, voltage-gated potassium channel antibodies.
Therefore, the patient was diagnosed with HE, and treatment with methylprednisolone 1 g daily started. The patient's condition improved dramatically after she received the second dose of corticosteroid and while being under the intravenous steroid therapy for five more days. Moreover, she had symptoms of catatonia and received 6 sessions of electroconvulsive therapy (ECT). The patient was discharged with 75 mg oral prednisolone per day, which was reduced to every other day after 3 months. Other medications include melatonin 3 mg every night for sleep problems, escitalopram 10 mg daily, and levothyroxine 0.1 mg every morning in addition to vitamin D3 supplement and pantoprazole for GI protection.
We have clinically monitored the patient every month. We conducted thyroid function tests, checked anti-TPO antibody serum level, and gradually reduced prednisolone 5–10 mg every month. Yet, after 3 years of corticosteroid treatment, steroid cessation has not been accomplished. If we reduce the prednisolone lower than 25 mg every other day, then the patient shows behaviors of irritability and aggression, her sleep time increases, and mood changes arise, as well as anti-TPO antibody serum level grows. Before the treatment, the level of anti-TPO antibody was 1120, but both during and after treatment, the level reached 620 and 20, respectively. In the next follow-up visit, thyroid ultrasonography and laboratory tests were normal.
3 DISCUSSION
With reference to the clinical presentation and paraclinical evaluations, HE or steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) was suggested. In addition, appropriate and first-choice treatment was corticosteroid therapy.
Clinical severity HE does not correlate with antibody titers.7 The antibody titers have not been found in correlation with the clinical severity of encephalopathy in HE treatment modalities. Previous documents suggest that steroid dosage should be initiated at 500–1000 mg/day for the first 3–5 days and administration of prednisolone may be continued orally (1–2 mg/kg/day) for few weeks to months, and finally, gradual tapering is needed.8
It is not known whether the level of antibodies is related to the severity of clinical symptoms.7 Our experience showed a correlation between increasing the autoantibody level and clinical symptoms after reducing the corticosteroid under 25 mg every other day. We suggest that there might be a correlation between autoantibody titers and the severity of psychiatric symptoms. We had a challenge in corticosteroid tapering after HE symptoms subsided because it needs clinical trials and meta-analysis studies.
Before treatment, Montreal Cognitive Assessment (MOCA) score was 8, and the EEG rhythm was abnormal.
Initial treatment in an early phase of acute encephalitis was administration of pulse corticosteroid 1 g/day until 5 days. At this time, the patient was alert and oriented and encephalitis symptoms were subsided. MOCA test score was 19, EEG rhythm was normal, and anti-TPO level was 206. The patient was discharged with prednisolone 1 mg/kg. In the next month, the dosage was decreased to every other time. Then, we tapered prednisolone 10 mg monthly. When the dosage prednisolone was 20 mg, every other time, agitation and confusion appeared and slow background EEG was detected. Then, we increased it to 30 mg/ daily, and the confusion was resolved while EEG rhythm became normal again. After 6 months, prednisolone was tapered. Finally, the patient got stable with prednisolone 20 mg every other time. The cognitive and behavioral symptoms and signs were controlled. The thyroid function tests and anti-TPO were intact.
In a previous study, it was assumed that treatment of this condition is specific.9, 10 We believe that it is a challenging one and individual treatment should be tailored as a case. Furthermore, there could be a correlation between the type of response to corticosteroid therapy, mood and behavioral changes, and changes in the dosage of corticosteroids. As a loss of determined guidelines, we recommend designing an eligible therapeutic protocol for corticosteroid therapy in the treatment of Hashimoto's disease and neuropsychiatry symptoms.
4 CONCLUSION
This study proved the relation between increased levels of autoantibody and clinical symptoms after reducing the corticosteroid under 25 mg every other day. In addition, there could be a relationship between the type of response to corticosteroid therapy, behavioral changes, and variations in the dosage of corticosteroids. Current pretreatment criteria of HE do not predict steroid responsiveness. We recommend designing an eligible therapeutic protocol for corticosteroid therapy in Hashimoto's disease and neuropsychiatry symptoms.
ACKNOWLEDGMENT
Many thanks to the patient and her family. We appreciate their cooperation in this survey.
CONFLICT OF INTEREST
No potential conflict of interest.
AUTHOR CONTRIBUTIONS
VA and RB visited the patient and collected the data. AA, MR, SA, and RB wrote the draft of the manuscript. FS revised and finalized the manuscript. All the authors have read and confirmed the final version.
ETHICAL APPROVAL
The patient signed an informed consent form prior to participation in the study. This study approved by the Ethics Committee of Roozbeh Hospital of Tehran University of Medical Sciences.
The authors confirm that the data supporting the findings of this case are available within the article.
REFERENCES
1Liu C-Y, Tseng M-CM, Lin P-H. Encephalopathy associated with autoimmune thyroid disease (Hashimoto's thyroiditis) presenting as depression: a case report. Gen Hosp Psychiatry. 2011; 33(6): 641.e7- 641.e9.
2Chong JY, Rowland LP, Utiger RD. Hashimoto encephalopathy: syndrome or myth? Arch Neurol. 2003; 60(2): 164- 171.
3Ercoli T, Defazio G, Muroni A. Status epilepticus in Hashimoto’s encephalopathy. Seizure. 2019; 70: 1- 5.
4Laurent C, Capron J, Quillerou B, et al. Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): characteristics, treatment and outcome in 251 cases from the literature. Autoimmun Rev. 2016; 15(12): 1129- 1133.
5Castillo P, Woodruff B, Caselli R, et al. Steroid-responsive encephalopathy associated with autoimmune thyroiditis. Arch Neurol. 2006; 63(2): 197- 202.
6Tomkins M, Cavalcoli F, Stanley E, et al. Autonomic alterations as a clinical manifestation of encephalopathy associated with autoimmune thyroid disease. Endocr J. 2018; 65(8): 869- 875.
7Correia I, Marques IB, Ferreira R, Sousa L. Encephalopathy associated with autoimmune thyroid disease: a potentially reversible condition. Case Rep Med. 2016; 2016: 1- 6.
8Menon V, Subramanian K, Thamizh JS. Psychiatric presentations heralding Hashimoto's encephalopathy: a systematic review and analysis of cases reported in literature. J Neurosci Rural Pract. 2017; 8(2): 261- 267.
9Zhou J, Xu B, Lopes J, Blamoun J, Li L. Hashimoto encephalopathy: literature review. Acta Neurol Scand. 2017; 135(3): 285- 290.
10Szydełko J, Litwińczuk M, Szydełko M. Hashimoto’s encephalopathy–an up-to-date overview. J Educ Health Sport. 2019; 9(9): 852- 873.





留言 (0)